
Abstract
Coronary ostial stenosis is a rare but potentially life-threatening complication of aortic valve replacement (AVR). It can present potential complications such as acute coronary syndrome, left ventricular failure, ventricular arrhythmias, or sudden death. Exact pathogenetic mechanism is not known, but a few hypotheses have been proposed. We present a case of left main coronary stenosis 11 months after AV R was done for symptomatic critical aortic stenosis. High index of clinical suspicion and timely coronary angiography helped to determine the exact etiology. A percutaneous coronary intervention was done emergently. The patient has done very well so far.
Introduction
Surgical aortic valve replacement (AVR) remains the cornerstone of treatment for symptomatic critical aortic stenosis (AS). It is rewarding for most of the patients, but it can have several associated complications. Coronary ostial stenosis is a rare but potentially serious complication of AVR. It was first described by Roberts and Morrow in 1967. 1 It is estimated to occur in about 1–5% of all AVR procedures. 2 6 The exact cause of coronary ostial stenosis is still undetermined, but few hypotheses have been proposed. 5 Symptoms are severe and generally appear within 1–6 months postoperatively. Coronary artery bypass grafting (CABG) is the typical treatment, but percutaneous coronary intervention (PCI) has also yielded favorable outcomes. 7 11 We present a case of left main coronary ostial stenosis 11 months after AVR was done for symptomatic critical AS, which was successfully managed with primary stent placement.
Case Report
In June 2015, a 67-year-old female with a long-standing history of asymptomatic critical AS was referred for AVR after new onset of shortness of breath. A preoperative transesophageal echocardiogram showed aortic valve area of 0.6 cm2 with 2
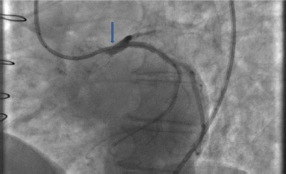
19-mm St Jude Biocor bioprosthetic aortic valve. The patient did well postoperatively. She was started on warfarin and discharged home. In May 2016, the patient experienced shortness of breath with moderate exertion, which was new. She underwent a stress cardiolite test, which was abnormal (Figs. 1–3). Repeat coronary angiography revealed 99% narrowing of left main coronary artery (LMCA) (Fig. 4). The left anterior descending artery, left circumflex, and right coronary artery (RCA) did not reveal any discrete stenosis. After consultation with the cardiac surgeon and the family, the patient underwent urgent primary stent deployment of LMCA (Fig. 5). A successful placement of intra-aortic balloon pump was also done in the left femoral artery since this was a high-risk procedure. The patient recovered very well and antiplatelet therapy was recommended for 12 months.

EKG during rest phase of stress test.

A 3-mm ST depression in Lead II in recovery phase of stress test.
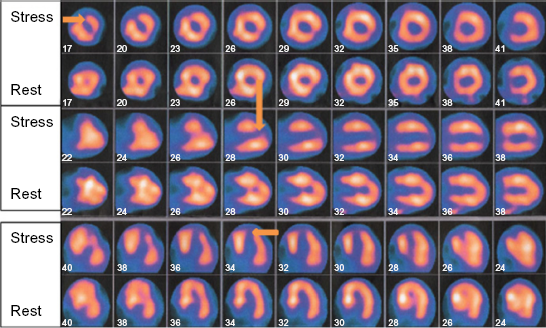
Apical ischemia with left ventricular cavity dilatation (arrow) on cardiolite imaging.

Ostial left main stenosis (arrow).
Ostial left main post stent placement (arrow).
Discussion
Coronary ostial stenosis after AVR occurs most commonly in the LMCA, but RCA can also be affected. 3 5 Exact pathophysiologic mechanism of coronary ostial stenosis has not been determined. Various theories have been proposed. Roberts and Morrow 1 discovered AVR fibrous thickening in the aortic root and proximal coronary artery in autopsy subjects. No evidence of atherosclerosis was seen on histological examination. 5 Intimal thickening and fibrosis near the aortic root have been proposed to be due to turbulent flow around the prosthetic valve leading to obstruction of the coronary ostia. 1
There may be microinjury and local hyperplastic reaction due to cardioplegic fluid and over dilation of the vessel by the tip of the catheter during AVR, and Tukiji et al. 12 have suggested immunologic reaction to the bioprosthesis. 13
Coronary ostial stenosis after AVR generally presents as unstable angina, left ventricular heart failure, ventricular arrhythmias, or sudden death. 7 High clinical suspicion is crucial. Prompt coronary angiography and emergent reperfusion strategies are vital for management. CABG may not always be a safe option, mainly due to the proximity of the graft site to the area of prior operation. 7 High incidence of perioperative infarction, increased mortality, and poor long-term outcome have been reported with CABG.2,3 Several reports have shown good early and late outcomes with PCI and stent implantation.5,6,12,13
Conclusion
Though rare, coronary ostial stenosis after AVR should be suspected in patients presenting with new relevant symptoms. Mostly, such cases have been reported to occur within 1–6 months after AVR, but it can manifest even later, as evident by our case. Thorough history and physical examination and timely coronary angiography should be performed if suspicion of coronary ostial stenosis is high. It can be fatal due to potential complications of acute coronary syndrome, left ventricular heart failure, or ventricular arrhythmias. Immediate reperfusion strategies are crucial in management. Although CABG is considered to be the typical treatment, PCI has shown to have good short-term results.
Author Contributions
Conceived and designed the experiments: MS, DM. Analyzed the data: MS, DM. Wrote the first draft of the manuscript: MS, DM. Contributed to the writing of the manuscript: MS, DM. Agree with manuscript results and conclusions: MS, DM. Jointly developed the structure and arguments for the paper: MS, DM. Made critical revisions and approved final version: MS, DM. Both authors reviewed and approved of the final manuscript.