
Abstract
This male patient presented with a scrotal abscess and urinary obstruction. The patient's history included a perineal abscess and the development of urethrocutaneous fistulae (watering-can perineum). He underwent multiple debridement procedures without resolution. During the fifth debridement for Fournier's gangrene, a biopsy revealed invasive squamous cell carcinoma. The patient was bedridden because of the large mass, a wide en bloc resection with lymphadenectomy and reconstruction was performed revealing a large (22 cm) squamous cell carcinoma originating from the urethra. He also received palliative chemoradiotherapy and hip hemiarthroplasty. Unfortunately, he succumbed to the disease. Given the recognized relationship between inflammation and the development of cancer, it is important to entertain a differential diagnosis of cancer, especially with erosive infections. This case report highlights the all too common late presentation of urethral cancer. Interestingly, despite correction of the bedridden state with palliative surgery, the patient did not perceive an improvement in quality of life based on the FACT-G questionnaire.
Keywords
Introduction
Most Urethral Carcinomas (UCs) are associated with invasive bladder tumors. 1 However, primary UC occurs and accounts for less than 1% of cases. Symptomatology includes obstructive or irritative voiding, and urethral strictures or stenosis. 2 In males, UCs primarily occur as squamous cell carcinoma (SCC). Other histological types include transitional cell carcinoma (urothelial carcinoma) and adenocarcinoma. The presence of different histology subclasses depends on the location in the urethra from which the primary tumor arises. 1 5
Symptoms typically occur at the late stage of the disease. Thus, most patients have a diagnosis of locally advanced disease and a poor prognosis.2,3 Treatment regimens remain controversial, 6 with limited cases to allow for consensus. Surgical intervention remains the leading form of therapy; however, approaches are case specific, depending on the location of the primary tumor and the degree of invasiveness. 1
While uncommon, UCs have a high mortality rate. Statistics remain inconclusive on long-term survival posttreatment. Most cases are diagnosed once the cancer is invasive, resulting in obtuse presentation of severe symptomatology.
Case Report
A male in his late 40s presented to an emergency department with a perineal abscess, which was surgically debrided and the bladder drained via a suprapubic catheter. One year later, he re-presented with further scrotal edema and abscess formation. The patient was unable to void transurethrally, developing urethrocutaneous fistulae (watering-can perineum) through which he voided voluntarily. There was extensive purulent and necrotic tissue involving the scrotum as well as 6.5 cm of bulbar urethral loss. The patient was started on IV antibiotics and a wound Vacuum Assisted Closure (VAC) was placed to promote healing. The patient underwent a total of four debridement procedures and was maintained on long-term antibiotics, without resolution.
Approximately six months later, he re-presented with Fournier's gangrene and underwent drainage of the scrotal abscess and further debridement of the chronic necrotic tissue. A sample of necrotic scrotal tissue was sent for differential diagnosis, and pathology revealed invasive moderately differentiated urethral SCC (Fig. 1). The patient had a 15 pack year history of smoking and a recent history of feeling weak and tired and having dyspnea. The patient described significant pain, stating that his pain ranged from 6 to 9/10.

Preoperative. This photo illustrates the extent of the scrotal abscess and cancer upon presentation. The urethra was obliterated. In addition to multiple areas of infection, there were nodular areas with squamous keratinization.
Further staging involved Computed Tomography (CT) and Fluorodeoxyglucose Positron Emission Tomography (FDG PET) scans, which revealed enlarged bilateral groin Lymph Nodes (LNs) (Fig. 2). In addition, there was direct invasion of the inferior pubic ramus and metastatic spread to the left femur intertrochanteric ridge. The patient's performance status was poor. He had been bedridden because of the large mass and had also developed sacral ulceration. Following interdisciplinary consultation, we elected to pursue surgery with the intent of effective palliation and debridement of the necrotic ulcer and chronic sepsis, as there was no evidence of distant lung metastasis.

Preoperative FDG-PET scans. The scans reveal enlarged PET avid bilateral groin LNs, in addition the PET avid scrotal and perineal tissue. (
He underwent an aggressive en bloc resection including radical penectomy, complete urethrectomy, radical scrotec-tomy, bilateral radical orchidectomy, bilateral pelvic lymphadenectomy, bilateral groin dissection, resection of inferior pubic rami with urogenital diaphragm, and en bloc resection of the rectum with permanent end colostomy positioned in the left lower quadrant. A cystotomy was positioned in the right lower quadrant. The large tumor resulted in a considerable defect (Fig. 3), requiring anterolateral thigh skin flap closure, performed by plastic surgery. The surgery took a total of six hours, without intraoperative complications.

Intraoperative. The photo shows the completed en bloc resection defect prior to flap closure.
Postoperatively, in the intensive care unit, the skin graft flap failed, requiring the installation of a new pedicle-based skin graft to the perineum from the opposite limb. After healing, he underwent a left femur hemiarthroplasty for the metastatic deposit in the intertrochanteric region. His total hospital stay postoperatively was three months. At discharge, the patient was able to ambulate. Interestingly, FACT-G questionnaire on the Quality of Life (QoL) pre- and post-operatively did not reveal a significant change [pre FACT-G 57; post FACT-G 61 (minimally important difference 6–7 points)]. 7
The en bloc resection revealed a large (22 cm maximal diameter) SCC, with lymphovascular and perineural invasion (Fig. 4). The tumor arose from the proximal region of the anterior urethra and involved almost the entire length. There were some condylomatous and verrucal features. Pelvic LNs were negative. However, LNs at the inguinal region tested positive for bilateral involvement. The inferior pubic bones were involved (Fig. 5). This placed the patient in a surgical stage pT4, N2, M1. The SCC tested negative for Human Papillomavirus (HPV), which was detected using p16 immunohistochemistry, suggesting that the identified condyloma was not the etiology of the SCC.
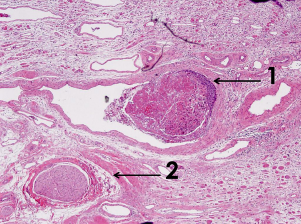
Histology specimen. This slide demonstrates the SCC with keratin and both (1) lymphatic invasion and (2) vascular invasion.

Metastasis to the pubic rami. This histopathology slide demonstrates the multifocal distant metastasis of the primary urethral tumor to the bone, in particular, to the right pubic inferior rami.
After discharge, the patient was followed up by medical oncology for consideration of adjuvant chemotherapy and radiation oncology for palliative radiotherapy. Restaging by whole-body FDG-PET scan revealed progression with multiple lung metastasis and recurrent pelvic disease, with left ischial and femoral bone metastases (Fig. 6). Despite this, the patient remained optimistic and proceeded with chemotherapy (seven cycles – carboplatin and gemcitabine) and palliative radiation for the painful bone metastasis.

Postoperative FDG-PET scan. Restaging revealed progression with multiple lung metastasis and recurrent pelvic disease, with left ischial and femoral bone metastases. (
Six months postsurgery, the patient was mobile and experiencing little pain. He had increasing leg edema, which was likely associated with progression of LN involvement. He was treated with further chemotherapy (four cycles – cisplatin and fluorouracil), which alleviated some symptoms. Unfortunately, the patient died of sepsis and metastatic disease two years after initial presentation of a perineal abscess.
Discussion
Primary UC is a rare disease that makes up less than 1% of all malignancies. 8 Three other cases where the primary tumor was mistaken for a urethral abscess and subsequently diagnosed as UC have been reported. 9 11 In two of the cases, the patients had a history of urethral stricture and ongoing infection that were managed with drainage of the abscess and multiple rounds of antibiotics with no resolution, similar to the patient presented in this case report.9,10
In our case, a tissue sample was not taken for differential diagnoses until the patient presented with Fournier's gangrene. Moreover, the patient's history was significant with the development of spontaneous urethrocutaneous fistulae, delayed presentation (possibly related to remote living situation), and a lifelong history of smoking, potentially affecting wound healing. This delayed presentation with advanced disease, however, is reportedly common for proximal UC, which carries a poor prognosis of 5%–15% five-year survival, despite aggressive treatment. 1
Although HPV is associated with urethral SCC, 12 it was not the etiologic agent in this case, leaving chronic inflammation as a potential etiologic risk factor. Well-known inflammatory conditions that increase a patient's risk for cancer include chronic inflammation and schistosomiasis in bladder SCC, Barrett's esophagitis in esophageal cancer, inflammatory bowel disease in colorectal cancers, and cholangitis in cholangiocarcinoma (reviewed by Coussens and Werb 13 ).
Distal and proximal UCs have different prognosis. 1 It is interesting to speculate that the more distal SCC may be HPV related and therefore more amendable to chemoradiotherapy similar to oropharyngeal SCC, 14 whereas the more proximal are inflammatory related requiring an aggressive surgical approach based on biology and disease extent. In this patient, aggressive demasculinizing surgery took him from a bedridden state to one of ambulation with the ability to receive chemoradiotherapy and possibly prolonged survival. However, the patient's perceived QoL was not significantly improved.
Conclusion
This case highlights the need for a high index of suspicion for cancer in erosive urethral strictures and the need for further multi-institutional research into the etiology, predictive markers, and management of these rare cases.
Author Contributions
Wrote the first draft of the manuscript: SM. Contributed to the writing of the manuscript: SM, OR, RM. Agreed with manuscript conclusions: SM, OR, RM. Jointly developed the structure and arguments for the paper: SM, OR, RM. Made critical revisions and approved the final version: SM, OR, RM. All the authors reviewed and approved the final manuscript.
Footnotes
Acknowledgment
The authors thank Ms. Nubia Zepeda for clerical assistance with the submission of this article.