
Abstract
By the recent introduction of molecular targeting drugs against BRAF mutation and immune checkpoint inhibitors, the prognosis of patients with melanoma in advanced stage is now improving, but still in the minority. Mucosal melanoma lacks the BRAF mutations, and hence conventional chemotherapeutic regimens must be improved. We have conventionally used dacarbazine (DTIC) for patients with metastatic mucosal melanoma. However, the efficacy of DTIC in patients with metastatic mucosal melanoma has been limited. Therefore, we explored other possibilities to improve the prognosis of patients suffering from metastatic mucosal melanoma. In this communication, we present a retrospective analysis of the sequential combination chemotherapy of DTIC with carboplatin and paclitaxel (CP) for metastatic mucosal melanoma of nasal cavity and paranasal sinuses. The objective response rate of seven patients is 14.3% by RECIST 1.1 and the overall survival (OS) is 12.5 months. These data indicate that the sequential combination chemotherapy of DTIC with CP could be an option for patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses who are currently ending into dismal prognosis.
Keywords
Introduction
Malignant melanoma is the sixth most commonly diagnosed cancer in the United States. 1 However, it is relatively uncommon among Africans, Hispanics, and Asians. Age-standardized morbidity rate in America was 161.7/1000,000 per year. 2 In contrast, very low incidence rates (0.6/100,000 in males and 0.5/100,000 in females) are estimated in Asia. 3 Among the different types of melanomas, extracutaneous melanoma that encompasses mucosal, ocular, and leptomeningeal types is rare compared with cutaneous melanoma. 4
The distribution of the primary site of melanoma in the Asian population seems to be different from that among Caucasians.5,6 A retrospective study from Duke University found that mucosal melanoma accounts for only 1.1% of 10,393 melanomas. 7 In contrast, it was reported that mucosal melanoma constitutes 24% of all malignant melanomas in China. 8 Similarly, mucosal melanoma constitutes a greater proportion of all melanomas in Japan, eg, 8%. 9 Due to its rarity, mucosal melanoma has not been studied enough and thus poorly characterized. Previous studies suggest that there are distinct characteristics between mucosal and cutaneous melanomas in terms of the biology, clinical course, and prognosis. 10 Therefore, a standard chemotherapy for metastatic mucosal melanoma has not been well established.
Our department of dermatologic oncology in National Cancer Center Hospital (Tokyo, Japan) is one of the referral centers of melanoma, especially when the melanoma becomes difficult to be treated, advanced, and metastasized. Patients with metastatic melanoma of nasal cavity and paranasal sinuses, although rare, are referred to our department.
Dacarbazine (DTIC) has long been used as the standard of chemotherapy for metastatic melanoma since the 1970s. 11 Several combination chemotherapies with DTIC have been tested, but no survival benefit has been demonstrated by the combinations.12,13 In 2002, Hodi et al. 14 first reported the results of the combination of carboplatin and paclitaxel (CP) for metastatic melanoma. In that study, of the 15 patients administered paclitaxel of 175 mg/m2 and carboplatin dosed to yield an area under the curve of 7.5 calculated according to the Calvert method with a 21-day cycle, 3 (20%) had partial responses (PR), 7 (47%) had stable disease (SD), and 5 (33%) showed evidence of progressive disease (PD).
In our retrospective cohort study, we validated the benefits of DTIC followed by combination of CP for patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses seen at our institution from 2011 to 2013. The results may serve as one of the real-world data in mucosal melanoma of nasal cavity and paranasal sinuses with distant metastases.
Patients and Methods
Patients
We retrospectively analyzed patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses who received DTIC followed by combination of CP at National Cancer Center Hospital from 2011 to 2013. During this period, 551 cases of melanoma were referred to our department. Of these cases, 77 (14.0%) were mucosal melanoma, including 27 of nasal cavity and paranasal sinuses origin.
Of these 27 cases, 23 were metastatic melanoma of nasal cavity and paranasal sinuses. Of the 23 cases, 7 were treated with DTIC followed by combination of CP, which we retrospectively analyzed in this study. All the seven patients were in Stage IV C (Tables 1 and 3). Of the other 16 cases, 4 cases were treated with DTIC monotherapy, 4 with palliative care alone, 4 to clinical trials, 1 received nivolumab, 1 underwent surgery, 1 was treated by CP alone, and 1 was transferred to another hospital.
Clinical characteristics of 7 patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses.

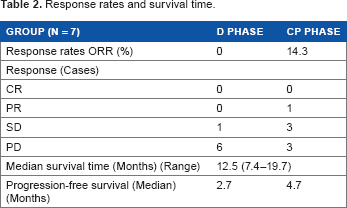
Response rates and survival time.
Clinical features and treatment response in 7 patients.

It was reported that the combination therapy of CP treatment was effective in head and neck malignancies. 15 Thus, the cost for combination of CP could be covered by the Japanese governmental health insurance plan, and when DTIC failed, we were able to give the combination to nasal and paranasal metastatic melanomas, which were located in the head and neck region.
Attending doctors decided to change from DTIC to the combination of CP after obtaining consent from individual patients with the explanation that, although it was reported that CP combination therapy may be effective for head and neck malignancies, and thus covered by the Japanese governmental health insurance plan, the effectiveness of CP combination was not directly proven in metastatic mucosal melanoma.
The medical records of all eligible patients were reviewed, and clinical parameters, including sex, age, primary site, performance status, number of metastatic organs, serum lactate dehydrogenase levels, and number of treatment cycles, were recorded.
Study design and treatment
Of the seven patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses, six patients received intravenous DTIC (800 mg/m2 or 1,000 mg/m2 on day 1 every three weeks) and one patient received intravenous DTIC (220 mg/m2 on days 1–5 every four weeks). Patients were offered to have additional combination of CP before or during DTIC therapy with explanation of possible benefit and disadvantages, especially side effects. All seven patients received sequential intravenous carboplatin (area under the curve = 6) and paclitaxel (200 mg/m2) on day 1 every three weeks. In all cases, DTIC was given until disease progression, whereas CP was continued until disease progression or development of severe adverse events.
Treatment outcomes
Clinical tumor response was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST Version 1.1). 16 Complete response (CR) was defined as the disappearance of disease, PR was defined as more than 30% decrease in tumor size without the appearance of new disease, PD was defined as more than 20% increase in tumor size or the appearance of a new lesion, and we added, as patent clinical progression, SD defined as neither PR nor PD.
Statistical analysis
Statistical analysis was performed using IBM SPSS statistics 24.0 software for windows. Survival probabilities were calculated according to the Kaplan–Meier method.
Results
Patient characteristics and follow-up period
Of seven patients (4 males and 3 males) with a median age of 71 years (range 46–76 years), all patients had performance status either 0 or 1 (Table 1). In this series of seven patients, as a treatment of primary sites, none received surgery, six were treated by proton beam, and one was treated by radiation therapy. Serum LDH level was within normal limit in two cases. Median number of metastatic organs was 3 with a range of 1–7. Three patients received two or less cycles of additional treatment of CP, whereas four patients received three or more cycles. Overall median follow-up period (from the first day of diagnosis to the last follow-up visit or demise) was 13.0 months, ranging from 5.9 to 20.3 months.
Response rate and survival time
No patient achieved CR. In “D phase” (D phase equals to the period of receiving DTIC), no patient showed PR, one patient had SD, and six patients had PD (Table 2). In “CP phase” (CP phase equals to the period of receiving CP), one patient achieved PR, three patients had SD, and three patients had PD (Table 2). The median overall survival (OS) was 12.5 months (range: 7.4–19.7 months; Fig. 1). The median PFS for “D phase” and “CP phase” were 2.7 and 4.7 months, respectively (Table 2). The one-year survival rate was 42.9% (three of seven cases). We described metastatic sites, LDH level, performance status, stages, treatment response, PFS, and OS in all seven patients (Table 3).

Overall survival of sequential combination chemotherapy of dacarbazine with carboplatin and paclitaxel.
Toxicity profiles
The toxicity profiles are presented in Table 4A and B. Toxicity event is referred to Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. No grade 3 or grade 4 was observed in “D phase” (Table 4A and B). In contrast, we found that two of seven patients (28.6%) developed grade 3 or grade 4 leukocytopenia and neutropenia, and anemia in “CP phase” (Table 4A and B). However, none stopped treatment because of the side effects of CP therapy.
(A) Toxicity profiles of D phase (n = 7). (B) Toxicity profiles of CP phase (n = 7).

(B) Toxicity profiles of CP phase (n = 7)

Discussion
Our department probably has the largest collection of melanoma patients in Japan. Of the patients seen for the last 10 years in our oncology department from 2005 to 2014, 1,170 cases of melanoma (cutaneous, ocular, and mucosal) were referred to our department. Of these, 166 cases (14.2%) were mucosal in origin, and 52 cases (4.4%) were nasal and paranasal sinuses (data not shown). Bishop and Olszewski 4 reported that mucosal melanoma of the nasal cavity and paranasal sinuses were 0.3% in the 229,714 cases of melanoma (cutaneous, ocular, and mucosal) from 1988 to 2010 in the Surveillance Epidemiology and End Results (SEER) database. Our institution is one of the referral centers of advanced malignancies, it is utmost important to improve the prognosis of patients with melanoma in advanced stages, especially those of metastatic mucosal melanoma and metastatic mucosal melanoma of nasal cavity and paranasal sinuses.
DTIC has been used as the standard of chemotherapy for metastatic melanoma for long since 1970s, and there are many studies of DTIC for advanced melanoma. More than 1,000 patients have been treated with DTIC in 8 randomized trials since 1992, with an overall response rate of 13.4% and median survival rate ranging from 5.6 to 11 months.12,17–23
Because most studies coalesce all metastatic cases regardless of sites of the primary, there are very few data available regarding the prognosis that was restricted to metastatic mucosal melanoma. Yi et al. 24 reported that the OS of 35 patients with metastatic mucosal melanoma (mucosa of head and neck, eye, gastrointestinal and genitourinary tract) treated with DTIC-based chemotherapy was 9.2 months. Regarding combination of CP, Chang et al. 25 reported that 10 cutaneous and 22 noncutaneous (mucosal, ocular, and primary unknown) melanomas were treated with DTIC or DTIC-based regimen followed by combination of CP and concluded that there were no significant differences in response rates (20% vs. 23%). However, the duration was longer in noncutaneous (5.3 months) than cutaneous (2.1 months) melanoma, and the duration of PFS was longer in noncutaneous (3.7 months) than cutaneous (1.6 months) melanoma.
From our institution, Kato et al. 26 reported a PR case of metastatic mucosal melanoma of nasal cavity treated with DTIC followed by combination of CP in 2014. Since mucosal melanoma of nasal cavity and paranasal sinuses with distant metastases currently does not have many options to salvage the patients.
BRAF mutations in mucosal melanoma are uncommon; mutation has been detected in less than 10% of mucosal melanoma. 9 It was reported that the BRAF mutation frequency of mucosal melanoma of nasal cavity and paranasal sinuses was only 3%. 27 Therefore, BRAF and MEK inhibitors are unlikely to change clinical practice for metastatic mucosal melanoma compared with metastatic cutaneous melanoma.
Three recent studies of ipilimumab for metastatic mucosal melanoma revealed PFS of 2.7–4.3 months and OS of 5.8–6.4 months, 28 30 which was not so remarkably different from chemotherapy (Table 5). However, obvious difference is that the long durable responses reached 20% or more. 31 In addition, nivolumab for 35 patients with metastatic mucosal melanoma showed PFS of 3.9 months and OS of 12.4 months. 32 Thus, immune checkpoint inhibitors are now changing the paradigm in a portion of patients suffering from metastatic melanoma in advanced stages.
Prognosis of metastatic mucosal melanoma treated by chemotherapy in literature.

Melanoma arising from mucosal commonly have activating KIT mutations, eg, 15.6%–21% of cases.33,34 In a phase II trial, 13 patients with metastatic mucosal melanoma with KIT mutations were enrolled and received imatinib. PR rate was 7 of 13 or 53.8%, PFS ranged from 0.9 to 27.1 months, and OS was from 1.5 to 27.1 months. 35 Thus, this treatment could be a treatment option for certain fraction of mucosal melanoma in the future.
Although DTIC has been the first-line treatment option for a long time, the current study with equal or better response rate by CP suggests that combination of CP could be the first-line therapy if the side effects can be managed.
We believe this study can be a step forward to propose that the sequential combination chemotherapy of DTIC with CP is one of the treatment options for patients with metastatic mucosal melanoma of nasal cavity and paranasal sinuses lacking BRAF mutation. In particular, earlier judgment of introduction of the combination of CP may offer benefits before patients are really deteriorated.
However, there are several drawbacks in this study because of retrospective and nonrandomized nature in small number of patients. Moreover, combination of CP has severe side effects (Table 4A and B). Therefore, attending physicians may allocate combination of CP to patients with better physical condition and naturally biased the results.
Conclusion
Although molecular target therapy and immune checkpoint inhibitors for advanced melanoma is in rapid and in remarkable progress, our retrospective data indicate that sequential combination chemotherapy of DTIC with CP could be considered as one of the treatment options for metastatic mucosal melanoma of nasal cavity and paranasal sinuses, till more specific treatment will become available.
Author Contributions
Conceived and designed the experiments: WO. Analyzed the data: WO. Wrote the first draft of the manuscript: WO. Contributed to the writing of the manuscript: WO, AT, KN, AT, KO, NY. Agree with manuscripts results conclusions: WO, AT, KN, AT, KO, NY. Jointly developed the structure and arguments for the paper: WO. Made critical revisions and approved final version: WO. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgements
We would like to thank Professor Hiroyuki Matsue, Department of Dermatology, Chiba University Graduate School of Medicine.