
Abstract
Coronary artery ectasia is a rare angiographical finding, and it accounts for less than 5% of all coronary angiograms. We report a case of a 55-year-old male patient who presented with fatigue and exertional chest pain. Paraclinical tests revealed cardiac ischemia and sinus node dysfunction, as well as coronary artery ectasia without significant coronary stenosis. Factors involved in cardiac ischemia in this context comprise slow flow, poor collateral circulation, microcirculatory dysfunction, lack of adequate exertional coronary vasodilatation, and endothelial dysfunction. Moreover, poor collaterals with rudimentary sinus node artery may explain sinus node dysfunction. Discussion is made in light of the relevant medical literature.
Introduction
Coronary artery ectasia (CAE) is a rare angiographical finding, with an estimated prevalence of 1%–5% of all invasive coronary angiograms. 1 CAE is a dilatation of coronary arteries. It is defined angiographically as having a pathological segment with a diameter of at least 1.5 times greater than that of the intact adjacent segment; when the disease is spread so that no intact segment is present, qualitative visual estimate is used for diagnosis.1,2 According to its etiology, CAE is classified as congenital or acquired, and the acquired form is subdivided into atherosclerotic or isolated (not directly related to atherosclerosis) forms. 2 Of note, CAE is usually encountered as an incidental finding in the setting of coronary angiography.
Case Presentation
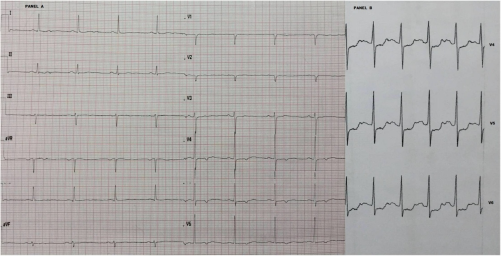
We report a case of a 55-year-old male patient with no relevant medical history presenting with exertional chest pain. He was not athletic and had no familial history of CAE. Physical examination was unremarkable and cardiac echogram was normal, namely, there was no regional wall motion abnormalities and no left ventricular hypertrophy. Cardiac biomarkers and C-reactive protein (CRP) were normal. Surface Electrocardiogram (EKG) showed sinus bradycardia at nearly 50 bpm with ST/T changes in anterolateral leads, and a stress test yielded typical chest pain with significant ST depression in lateral leads (Fig. 1). Moreover, there was a delayed and disproportional heart rate acceleration compared with the exercise load, suggesting chronotropic incompetence. Coronary angiogram (Fig. 2) showed extensive CAE with delayed sluggish flow and complete filling of distal territories, stasis, poor collaterals, and without significant stenosis. No other patent cause of cardiac ischemia (ie, myocardial bridge, abnormal coronary anatomy, etc.) was encountered on the coronary angiogram. Of note, the sinus node artery was not clearly visualized, and if present it was considered rudimentary; also, no coronary intraluminal thrombus was visible. The patient was managed with medical therapy consisting of antiplatelets, angiotensin-converting enzyme inhibitor, and a slow dose of beta-blocker with intrinsic sympathomimetic activity (acebutolol) in order to avoid exacerbating the bradycardia.
(

Coronary angiogram showing diffuse coronary ectasia; (
Discussion
The exact mechanisms that cause abnormal dilatation of the coronary arteries are still poorly understood, and many factors are involved in the pathophysiology of CAE, including molecular, cellular, and tissular factors. Enzymatic degradation of the extracellular matrix of the media is a major pathophysiologic process that leads to CAE.2,3 Though various hypotheses have been put forward, the most accredited hypothesis recognizes that uncontrolled activity of metalloproteinases is a major causal factor. 2
Inflammation, tissue remodeling, and upregulation of matrix metalloproteinases are key factors in the pathogenesis of CAE. The inflammatory component is represented by elevated levels of different inflammatory markers. 2 The inflammatory process, along with the upregulation of metalloproteinases, leads to destruction of the vascular media, as smooth muscles are replaced by hyalinized collagen, with subsequent attenuation of the vascular wall and dilation. 2
An increased incidence of atherosclerotic coronary artery disease in patients with CAE has been reported 1 ; however, many phenomena other than atherosclerotic coronary stenosis may be involved in cardiac ischemia in CAE, including formation of thrombus, slow flow, poor collateral circulation, microcirculatory dysfunction, lack of adequate exertional vasodilatation, and endothelial dysfunction.2,4 In the presented case, although there was no evidence of significant atherosclerotic stenosis, the patient's stress test was positive. This was our patient's first trouble. The involvement of each of the above-cited factors in cardiac ischemia could not be assessed in the presented patient; however, coronary angiogram showed a poor collateral circulation. In view of this, we conclude that the above-cited processes are likely mechanistic factors in the genesis of cardiac ischemia rather than simple epiphenomena of CAE.
In the presented patient, the etiology of CAE is not definite and we estimate that it belongs to the isolated idiopathic subtype. 2 The absence of coronary artery stenosis is an argument against the atherosclerotic acquired form; the absence of familial history of CAE is an argument against the congenital form; a normal CRP is an argument against the acquired inflammatory type. However, an extensive etiological workup was not completed, as stated in the “Limitations” section below.
The presence of sinus node dysfunction, potentially consecutive to CAE, was the second trouble encountered in this patient, manifested as baseline relative bradycardia and chronotropic incompetence during the stress test. The age of the patient was not in agreement with a primary sinus node disease, and he was also not an athletic nor taking any medication that blocks the sinus node. The sinus node artery arises from the proximal right coronary artery in more than 60% of cases and from the left coronary artery in less than 40% of cases. 5 The presence of rudimentary sinus node artery in the setting of poor collaterals in CAE is recognized as a potential cause of sinus node dysfunction. 6 Accordingly, we estimate that our patient's secondary sinus node dysfunction is a mechanistic association with CAE.
Management of CAE is mostly medical, consisting of antiplatelet therapy, beta-blockers, angiotensin-converting enzyme inhibitors, statins, and dihydropyridine calcium channel blockers. 2 In severe cases and/or when complications may occur (severe coronary aneurysm, thrombus, and coronary stenosis), anticoagulant therapy is needed, and percutaneous intervention (±thromboaspiration) or even coronary artery surgery may also be required. 2
Conclusion
CAE is an incidental finding in most cases, given its asymptomatic character. In the presented case, CAE is manifested as angina and fatigue, consecutive to cardiac ischemia and sinus node dysfunction, respectively. Moreover, the presence of cardiac ischemia and secondary sinus node dysfunction was consecutive to CAE, and therefore we estimate that the association is causal rather than epiphenomenal in this context.
Limitations
Though the most likely etiology, according to the available data, is isolated form, an extensive etiological workup regarding the possible etiology of CAE in this patient was not performed. Moreover, a 24-hour Holter monitoring, along with heart rate variability measurement, would have provided more evidence in favor of sinus node dysfunction.
Author Contributions
Conceived and designed the experiments: VR, AK. Analyzed the data: VR. Wrote the first draft of the manuscript: VR. Contributed to the writing of the manuscript: VR, AK. Agree with manuscript results and conclusions: VR, AK. Jointly developed the structure and arguments for the paper: VR, AK. Made critical revisions and approved final version: VR, AK. Both authors reviewed and approved of the final manuscript.