
Abstract
Disk fragment relocation is commonly limited to the anterior epidural space, although posterior epidural movement of a sequestrated disk piece to the posterior epidural space is in frequent. We present an uncommon case of dorsal extradural sequestration of lumbar disk herniation. A 77-year-old man presented with severe leg pain, low back pain, and urinary incontinence. Deep tendon reflexes were inattentive at the knee and ankle, and the motor power in terms of ankle dorsiflexion and great toe dorsiflexion was 2/5 in both lower limbs. There was hypoesthesia in the S1, S2, and S3 dermatomes. Magnetic resonance imaging displayed a large isointensity lesion at the L4–L5 level on the T2 sagittal image, indenting circumferentially the thecal sac from lateral to posterior of the thecal sac. The patient underwent an L4–L5 central laminectomy. A large, solid epidural disk fragment was recognized dorsally, with major compression of the thecal sac. The patient report improved lower extremity motor function at three-month follow-up. A displaced disk fragment should be considered as causative when patients present with cauda equine syndrome and be treated as a surgical emergency.
Keywords
Introduction
Disk fragment relocation is commonly limited to the anterior epidural space, which is well defined and surrounded by the posterior longitudinal ligament (PLL) and by the lateral membranes that are linked to PLL. 1 Migration of a disk fragment to the posterior epidural space is infrequent. Previously reported cases were related to middle-aged adults who suffered from radiculopathy over a comparatively small period. 2 4 In contrast, our patient was an older man and had a lengthier period of exhibiting minor symptoms. We present an uncommon case of dorsal extradural sequestration of lumbar disk herniation. The patient has given consent for publication of this report.
Case Presentation
History
The patient was a 77-year-old man who presented emergently with sudden onset of severe leg pain, serious low back pain, and urinary incontinence. He suffered from a chronic bilateral radiculopathy without any evidence of neurologic deficit. He had no previous trauma or family history of low back pain, and he had no history of a systemic disorder and any recent weight loss or fever.
Examination
Deep tendon reflexes were absent at the knee and ankle, and the motor power in terms of ankle dorsiflexion and great toe dorsiflexion was 2/5 in both lower limbs. There was hypoesthesia in the S1, S2, and S3 dermatomes. Rectal tone was diminished. In addition, the patient had bladder incontinency.
Magnetic resonance imaging (MRI) displayed a large isointensity lesion at the L4–L5 level on the T2 sagittal and axial images (Figs. 1 and 2), indenting circumferentially the thecal sac from lateral to posterior of the thecal sac, and extrusion of the disk compressing the thecal sac.
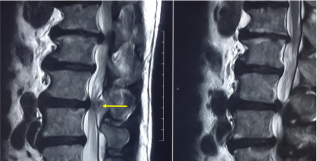
Sagittal T2 MR imaging revealing an isointensity lesion at the L4–L5 level and extrusion of the disk compressing the thecal sac.

Axial MR imaging revealing extrusion of the disk compressing the thecal sac.
The lesion was isointense to hyperintense on T2-weighted images. Because of the urgency of the case, lumbar spine MR imaging with gadolinium was not taken.
Laboratory standards comprised an erythrocyte sedimentation rate of 11 (normal range was between 9 and 15) and a C-reactive protein of 0.5 mg/L (>1.3 was abnormal), making an infectious course improbable.
Operation
The patient underwent an emergent L4–L5 central laminectomy and posterior fusion (due to intraoperative detection of instability) in prone position. A large, solid epidural disk material was recognized dorsally, with major compression of the thecal sac (Figs. 3 and 4). A lengthway division of the lateral boundary of the spinal canal exposed tracking of the disk fragment ventral to the L4–L5 disk space, as well as a significant annular deficiency along the lateral feature of the disk space.

A large (about 4 cm long), solid epidural disk material was recognized dorsally, with major compression of the thecal sac intraoperatively.

The operative field and spinal cord after decompression and some portion of posterior disk fragment.
Postoperative course
clinically, the patient had quick and complete return of motor task and a cessation of radicular pain. He did well postoperatively and had complete recovery of motor function with the motor power of 4/5 in all muscle groups on the first postoperative day. After a few sessions with the in-hospital physical therapists, the patient reports return of normal lower extremity motor strength, which is considered as sufficiently stable for home release. The patient identified the strength of the lower extremities improving at 3 months of follow-up.
Discussion
Disk sequestration can be distinguished as a herniated disk by a tear of the fibrous ring (or outermost annulus fibrosus) with movement of the disk piece to the epidural space. 1 The most common corridor in terms of disk fragment migration is a posterior and posterolateral route to the frontal epidural space. This is bordered by the connection of the PLL and its related “midline septum” and “lateral membranes”.1,4,5 Consequently, disk fragment migration frequently occurs cranially, caudally, or laterally, and only rarely lodging in the posterior epidural space. The relocation of a sequestrated disk fragment in this manner has been only rarely reported.2,4 Rather, the majority of the reported cases have concerned the lumbar area, and a small number of cases involving the cauda equine syndrome have been described.2,3 We searched the literature and found just three reports of dorsal disk herniations in elderly patients.6,7
MR imaging, particularly by means of gadolinium administration, appears to be the main option for diagnosis. Sequestrated fragments regularly demonstrate low signal intensity on T1-weighted images, and 80% of cases display a high signal intensity on T2-weighted images in relation to the degenerated disk from which the fragments are derived. 8 The high signal intensity on T2-weighted images can be explained as the herniated substance still having a higher water content compared to an unbroken disk or can be due to a reparative course leading to a temporary water increase. 8 The residual 20% had isointense signal intensity relative to the degenerated disk on T2-weighted images; a similar result was distinguished in our patient. Most of the disk fragments generate a peripheral contrast enhancement attributed to an inflammatory response with granulation tissue and recently formed vessels approximating to the sequestrated tissue. 9
There are numerous differential diagnoses with overlying features for a posterior epidural mass, which predominantly consist of meningioma, hemangioma, metastasis, lymphoma, epidural hematoma, synovial cyst, and abscess. 10 Meningiomas and hemangiomas usually reveal a solid and rather homogeneous postcontrast enhancement. In cases of metastases and lymphomas, the patients usually present with multisystem involvement and marrow abnormalities. Abscesses and hematomas usually demonstrate peripheral rim of enhancement with an associated infectious illness or history of trauma. 10
Owing to the usual natural history of disk herniation being in an upward or downward direction, there are very few reports of posterior extradural disk migration, given that it is not the first concept that springs to mind. 11 14 The earliest report of similar kind was presented by Lombardi in 1973. 15
In our case, the representative factor with regard to disk herniation was that the patient had an abrupt appearance of symptoms, but otherwise his general health was good. All these factors point toward the less probable likelihood of epidural tumor or abscess. The literature review shows 20 cases of cauda equine syndrome associated with dorsal extradural lumbar disk herniation since the first report by Lombardi 15 in 1973. We reviewed the literature and found only two reports of dorsal disk herniation in elderly patients.5,6
Some authors have suggested that heavy labor, traction, spinal manipulation, and conditions of hypermobility may predispose fragments of the disk to posterior migration.16,17 As noted by us in our review of similar cases, most of them have a history of some trauma before the onset of symptoms, which supports this hypothesis. Also, in all cases, prompt surgery involving an open procedure with complete decompression provided good results.
We described a case of cauda equine syndrome secondary to migration of a disk fragment to the posterior epidural space in an elderly man. Defining the site of the lumbar disk herniation, both extradural and intradural, is a diagnostic trial. Whenever there is distress associated with the diagnosis, suitable scans and different diagnostic styles should be applied. Any compressive lesion causing cauda equine syndrome even in the elderly patients should be considered as a sequestrated disk herniation and decompressed as a matter of urgency.
Lessons for Medical Practitioners
Posterior migration of a disk fragment is infrequent.
PLL, peridural membrane, ligament of Hoffman, dural sac, epidural fat, and neural roots arrangement are accepted barricades to disk migration.
Posterior migration of a disk can be a diagnosed as a result of spinal mass effect not only in middle age but also in older patients.
Any compressive lesion causing cauda equina syndrome even in the elderly patients should be considered as a sequestrated disk herniation and decompressed as a matter of urgency.
Author Contributions
Conception and design: KH, HRGQ. Reviewed submitted version of manuscript, approved the final version of the manuscript on behalf of all authors, and study supervision: KH.