
Abstract
A 67-year-old man with elevated serum immunoglobulin G4 (IgG4) levels, systemic lymphadenopathy infiltrated by IgG4-positive plasma cells, and Coombs-positive autoimmune hemolytic anemia (AIHA) showed marked hypercalcemia. Although the intact parathyroid hormone (PTH) level was elevated, 99mTc-MIBI scintigraphy and thyroid ultrasonography revealed no evidence of primary hyperparathyroidism. Liver biopsy showed marked infiltration of IgG4-positive plasma cells, which confirmed the diagnosis of IgG4-related disease (IgG4-RD). Corticosteroid therapy was initiated, and subsequently, intact PTH and serum calcium levels gradually normalized. Transient hypercalcemia in a patient with AIHA may therefore be associated with IgG4-RD.
Introduction
IgG4-related disease (IgG4-RD) is a systemic condition characterized by elevated serum levels of IgG4 and tissue infiltration by IgG4-positive plasma cells that affects multiple organs.1–6 Several reports of IgG4-RD combined with autoimmune hemolytic anemia (AIHA) have been published7,8; however, parathyroid gland involvement has not been previously reported. Here, we present a rare case of IgG4-RD associated with AIHA and high serum levels of intact parathyroid hormone (PTH) and calcium, which were reversed with intravenous (IV) corticosteroid therapy.
Case
A 67-year-old man presented with shortness of breath and fatigue for one month. In 2012, he was admitted to our hospital with worsening anemia (hemoglobin, 5.1 g/dL; hematocrit, 14.9%). Laboratory data revealed Coombs-positive AIHA. He had a history of gastric and esophageal cancer, and we initially suspected cancer recurrence. Contrast-enhanced computed tomographic (CT) imaging of the chest and abdomen showed systemic lymphadenopathy (cervical, axillary, perigastric, portal, paraaortic, and inguinal lymph nodes), but no solid mass in any of the organs or lymph nodes. Positron-emission tomography/computed tomography (PET/CT) (Fig. 1) showed fluorodeoxyglucose (FDG) accumulation in the same lymph nodes as well as in the salivary glands. Sjögren's syndrome was ruled out based on the normal levels of anti-SSA/Ro and anti-SSB/La. Based on the elevated serum IgG of 3,421 mg/dL and IgG4 of 391 mg/dL, we suspected a diagnosis of IgG4-RD.

(
The biopsy of an inguinal lymph node from the right side revealed lymph node enlargement with an expanded paracortical region and marked infiltration of plasma cells (focally up to 100 cells/high power field). Further, follicular hyperplasia and fibrosis were observed. The plasma cells were not atypical or blastic, and no restriction of the immunoglobulin light chain was present (kappa/lambda ratio = 2). Almost all plasma cells were IgG-positive, and the IgG4/IgG ratio was 0.3 (Fig. 2). There was no evidence of malignancy or acute inflammation. As the patient's hemolysis had resolved, he was discharged from the hospital after receiving a blood transfusion.
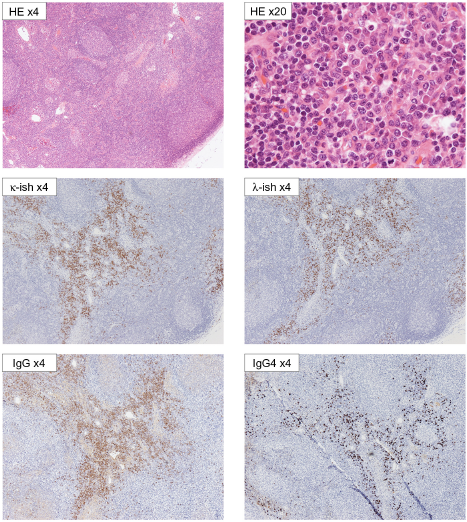
Biopsy of an inguinal lymph node in the right side. The plasma cells were not atypical or blastic. No immunoglobulin light chain restriction was seen (kappa/lambda ratio = +2). Almost all plasma cells were IgG-positive, and the ratio of IgG4/IgG was 0.3.
At 40 days after discharge, he visited the emergency department after hypercalcemia and renal dysfunction were detected during a routine visit to his family physician. On readmission, laboratory findings (Table 1) showed serum calcium of 14.4 mg/dL (adjusted for albumin), blood urea nitrogen (BUN) of 51.5 mg/dL, creatinine of 5.37 mg/dL, alkaline phosphatase (ALP) of 1,422 U/L, and gamma-glutamyl transferase (γGTP) of 364 U/L. He had no symptoms other than malaise. The 12-lead electrocardiogram was normal. We suspected that the renal abnormalities had been preceded and caused by hypercalcemia, since his renal function was normal 2 weeks before readmission. While the results for serum levels of intact PTH, parathyroid hormone-related protein (PTHrP), and 1–25(OH)2 vitamin D were awaited, treatment for hypercalcemia was initiated with IV fluids, bisphosphonate (pamidronate disodium hydrate 30 mg), calcitonin (elcatonin 80 U/day for three days), and IV corticosteroids (prednisolone sodium succinate 120 mg/day for three days, 20 mg/day for two days, and 10 mg/day for two days) (Fig. 3).

Clinical course at the second admission.
Laboratory data at second admission.

During the second admission, the serum level of intact PTH was 95 pg/mL (normal, 10-65 pg/mL) and PTHrP was <1.1 pmol/L (normal, ≤1.1 pmol/L). 99mTc-MIBI parathyroid scintigraphy (Fig. 4) and parathyroid ultrasonography showed no abnormal findings, ruling out primary hyperparathyroidism. Gastroscopy and colonoscopy revealed no abnormalities, and upper gastrointestinal endoscopy showed no evidence of Helicobacter pylori infection. No M protein was detected in blood or urine. Bone marrow biopsy revealed no evidence of malignancy, and screening for human T-lymphotropic virus type 1 (HTLV-1) was negative.
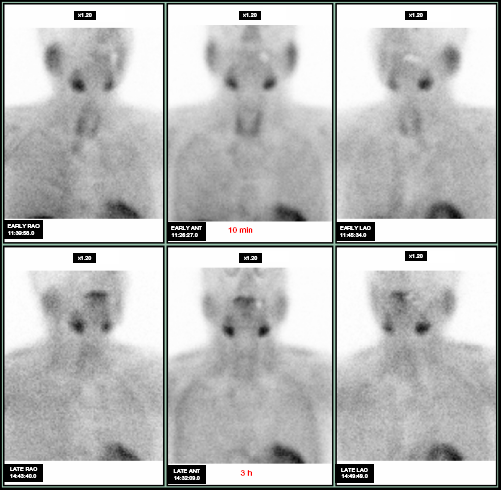
99mTc-MIBI parathyroid scintigraphy was negative, and no ectopic parathyroid glands were found.
Because ALP and γGTP levels continued to increase even after the administration of prednisolone, we performed a percutaneous needle liver biopsy on day 26 of the second admission. Histopathological examination showed plasma cell infiltration in Gleason's area but no active hepatitis or fibrosis. The ratio of IgG4-positive and IgG-positive plasma cells was 0.4 (Fig. 5). This finding was compatible with the diagnosis of IgG4-RD. 9
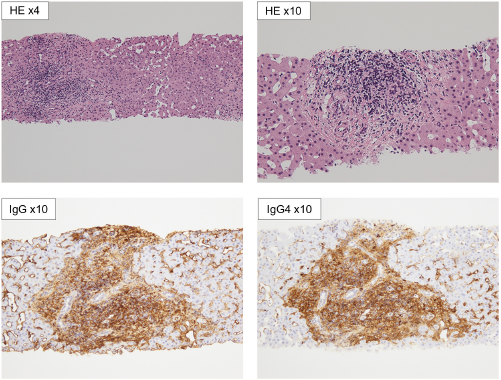
Liver biopsy. Plasma cells infiltration was noted in Gleason's area; however, no active hepatitis or fibrosis was seen. The ratio of IgG4-positive/IgG-positive plasma cells was 0.4.
The patient's serum calcium, kidney function, and intact PTH gradually returned to normal by 15 days after the first dose of prednisolone. ALP and γGTP levels also slowly normalized and were within normal limits three months after corticosteroid therapy was initiated. A repeat PET/CT scan showed resolution of abnormal FDG uptake in the lymph nodes and salivary glands. Follow-up for more than two years has shown no recurrence of AIHA, hypercalcemia, renal dysfunction, or ALP and γGTP elevation.
Discussion
IgG4-RD is a systemic disease characterized by tumefactive lesions, a dense lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells, and elevated serum IgG4 concentrations. 10 IgG4-RD has been described in many tissues/organs, including the biliary tree, salivary glands, periorbital tissues, kidneys, lungs, lymph nodes, meninges, aorta, breast, prostate, thyroid, pericardium, and skin. Several reports have described IgG4-related autoimmune pancreatitis combined with AIHA,7,8 which permanently resolved after steroid therapy.
Here, we diagnosed a patient with IgG4-RD involving the liver, systemic lymph nodes, and salivary glands combined with AIHA. The elevated serum levels of intact PTH and calcium suggested hyperparathyroidism, although these glands were normal on 99mTc-MIBI scintigraphy. The intact PTH level returned to within normal range after treatment with corticosteroids. IgG4-RD involving the parathyroid glands has not been reported previously. However, it has been previously reported that some patients have antibodies that inactivate the calcium-sensing receptor, resulting in acquired hypocalciuric hypercalcemia. This is associated with hypercalcemia and elevated PTH levels, and some of these patients have a history of multiple autoimmune disorders.11–13 Although the diagnosis was not proven in this case, the clinical findings suggest that IgG4-RD may have affected the calcium-sensing receptor of the parathyroid glands.
Author Contributions
Conceived and designed the experiments: SHasegawa. Analyzed the data: SHasegawa. Wrote the first draft of the manuscript: SHasegawa. Contributed to the writing of the manuscript: SHasegawa, SM, SHagiwara. Agree with manuscript results and conclusions: SHasegawa, SM, SHagiwara. Jointly developed the structure and arguments for the paper: SHasegawa, SM, SHagiwara. Made critical revisions and approved final version: SHagiwara. All authors reviewed and approved of the final manuscript.