
Abstract
Metastatic disease to the heart is not uncommon. We describe a case of a man in his 60s with an unusual metastasis to the heart and detail its intracardiac location by means of cardiac computerized tomography (CCT) and transthoracic echocardiography. To our knowledge, this is the first report of a pancreatobiliary tumor metastasizing exclusively to the left ventricle (LV) of the heart.
Introduction
Metastatic disease to the heart is not uncommon. A study conducted on autopsies of patients with a known non-cardiac primary malignant neoplasm revealed cardiac metastasis in 9.7– 10.7% of cases. 1 Additional post-mortem studies have quoted the number of cardiac metastases in patients who had died of malignancies as high as 25%. 2 Despite these differing reports, cardiac infiltration is commonly found in metastatic carcinoma. Identification and characterization of metastatic cardiac disease necessitates differentiation of normal cardiac structures from the metastatic lesion. This is often difficult because of infiltration of the tumor and similar characteristics of normal and abnormal tissues. Examination with different imaging modalities can highlight distinct characteristics of an abnormal mass. Tissue echogenicity, tissue attenuation, and differential uptake of intravenous contrast enhance our ability to differentiate abnormal from adjacent normal structure as well as characterize the abnormal tissue itself. 3 Metastatic cardiac neoplasms are much more likely than a primary malignant cardiac neoplasm. Most cardiac metastases spread from the lungs (in men) and breasts (in women). In other instances, they can spread by direct extension from the esophagus and mediastinum. 3 We describe the echocardiographic and cardiac computerized tomography (CCT) findings of a man in his 60s with an undifferentiated pancreatobiliary carcinoma and a left ventricular mass.
Case Summary
A man in his 60s with a past medical history significant for hypertension presented to an outpatient urologist with microscopic hematuria, left flank pain, and a 10 pound weight loss over a month and a half. Investigation of his symptoms with CT scans of the abdomen and pelvis revealed an 8-cm lesion on the left upper pole of his kidney. A PET scan revealed activity in the left kidney. Pending further workup, the decision was made to admit this patient to our institution for left total nephrectomy and adjuvant immunotherapy for a presumed renal cell carcinoma.
Pre-operative risk stratification was undertaken. During this evaluation, the patient revealed progressive dyspnea on exertion over three months and denied chest pain, orthopnea, paroxysmal nocturnal dyspnea, or palpitations. The patient was afebrile, with a resting blood pressure of 136/83 mmHg, pulse of 91/minute, respiratory rate of 18 breaths/minute, and resting oxygen saturation of 96% in room air. On physical examination, the patient had an audible S1/S2 with a regular rate and rhythm and no murmurs, rubs, or gallops; there was no jugular venous distension. Rales were audible at both lung bases. The extremities showed no clubbing, cyanosis, or edema, and the remainder of the physical examination was unremarkable. Laboratory workup was significant for a white blood cell count of 20.9 mm3, hemoglobin of 10.9 g/dL, hematocrit of 34.8%, sodium of 131 mmol/L, creatinine of 1.3 mg/dL, and an international normalized ratio (INR) of 1.67. Electrocardiogram showed normal sinus rhythm at a rate of 90 bpm with a first degree atrioventricular block, right bundle branch block, and T-wave inversions in leads I, aVL, V5, and V6.
In consideration of the patient's history and symptoms, a transthoracic echocardiogram (TTE) was performed to evaluate for possible cardiac involvement via the inferior vena cava. Echocardiography revealed an irregular multilobulated mass (2.5 × 1.5 cm) infiltrating the apical lateral wall of the left ventricle (LV), with multiple highly mobile components attached to the main mass (Figs. 1 and 2). There was normal left ventricular function, internal dimensions, wall thickness, and no regional wall motion abnormalities. No masses were seen in the right heart, inferior vena cava (IVC), or pericardium, and the remainder of the TTE was unremarkable.
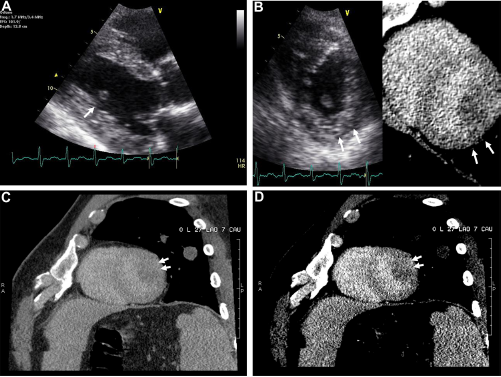
Transthoracic parasternal long-axis view (

Transthoracic apical four-chamber and the corresponding oblique CT image (
The patient then underwent further evaluation with 64-detector CCT. Three non-contrast enhancing low attenuation foci were present within the free wall and interventricular septum of the left ventricular myocardium (Figs. 1 and 2). There were also numerous nodules and masses present within both lungs, multiple heterogeneous lesions within the liver, and a large mass in the upper pole of the left kidney.
At this point, with these associated findings and the realized complexity of the case, tissue diagnosis was sought with ultrasound-guided needle core biopsy of a left lobe liver mass. Biopsy of this mass was immunoreactive for Ca19.9, CK7, CD10, and polyclonal CEA. The cells were nonreactive for Vimentin, CK20, and TTF1. The morphologic characteristics of abundant sclerotic stroma and immunohistochemical characteristics suggested a poorly differentiated carcinoma consistent with pancreatobiliary origin.
The patient subsequently began palliative radiation therapy and later developed a right-sided stroke, presumably from tumor emboli. He was later discharged from the hospital with the intent of undergoing palliative radiation treatment.
Discussion
Our case demonstrates a rare intracardiac left ventricular metastatic tumor of pancreatobiliary origin. Metastatic disease to the heart is much more common than primary cardiac tumors. In patients dying of a malignant disease, approximately 10% are found to have metastasis to the heart and pericardium. 4 This figure does not include liquid tumors, including leukemias, which frequently exhibit cardiac involvement. The most common tumors that metastasize to the heart include malignancies of the lung and breast as well as lymphomas, leukemias, and melanomas. Often times, these tumors will invade the right side of the heart or the pericardium; less commonly, we can see involvement of the left side of the heart. 4
Typically, extra-cardiac tumors reach the heart by one of four mechanisms: hematogenous, lymphatic, transvenous extension, or direct extension. 1 Depending on their origin, these tumors will preferentially metastasize to specific areas of the heart. For example, tumors of the breast are likely to travel to the heart via lymphatics and will therefore usually metastasize to the pericardium. Those tumors that travel hematogenously, such as melanomas, leukemias, and lymphomas, are usually seen in the myocardium. 1 Less commonly, metastatic disease may be found from infradiaphragmatic tumors, such as renal cell carcinomas, 5 hepatocellular carcinomas, 6 adrenal carcinomas, uterine leiomyomas, and cancers of the gallbladder. 7 These tumors reach the heart via transvenous extension and eventually reach the right atrium via the inferior vena cava. 2
Tumors of pancreatic origin that reach distant sites typically invade the liver, peritoneum, and omentum; vascular invasion via the superior mesenteric artery, inferior vena cava, celiac axis, and portal venous system is also commonly seen. 8 Metastatic implantation in other distant sites is exceedingly rare, with only isolated case reports.9,10 The tumor that we describe represents an infradiaphragmatic tumor of pancreatobiliary origin that has reached the left ventricular cavity, without leaving metastatic deposits in any other portion of the heart. Based on the tumor's location, one would expect that if cardiac metastasis occurred, it would be through trans-venous extension to the right side of the heart. Paradoxically, this tumor, which infrequently invades the heart in any capacity, has managed to implant, exclusively, in the left side of the heart, creating a very unusual mechanism of metastatic spread. One would have to assume that this tumor invaded the pulmonary veins by means of spread from the lung, and therefore, bypassed the right heart. Alternate mechanisms would include right to left spread by means of atrial septal defect, ventricular septal defect, or patent foramen ovale. However, we have no evidence to support this theory, given the absence of these abnormalities on either transthoracic echocardiography or CCT.
Conclusion
Metastastic pancreatobiliary tumors exclusive to the left heart have not been previously described. The mass we describe appears to infiltrate the endocardial border of the left ventricular myocardium. No intracardiac communication and no evidence of right heart involvement were found. The left ventricular masses were characterized by transthoracic echocardiography and CCT, but diagnosis was inferred by hepatic fine needle biopsy.
Author Contributions
Conceived and designed the experiments: ANM, LB. Analyzed the data: ANM, LB. Wrote the first draft of the manuscript: ANM, LB. Contributed to the writing of the manuscript: ANM, LB. Agree with manuscript results and conclusions: ANM, LB. Jointly developed the structure and arguments for the paper: ANM, LB. Made critical revisions and approved final version: ANM, LB. Both authors reviewed and approved of the final manuscript.