
Abstract
Interpreting an abnormal serum calcium level in subjects with chronic kidney disease (CKD) requires the simultaneous evaluation of various clinical and laboratory parameters. An excessive intake of calcium salts and vitamin D overdosing may be the most common etiologies of hypercalcemia in individuals with advanced CKD. Nevertheless, it should be noted that such patients are susceptible to all diseases that may cause hypercalcemia in subjects without renal disease. In this report, we describe the case of a male chronic hemodialysis patient who developed asymptomatic hypercalcemia associated with polyarticular swelling. On the basis of the findings of systemic workup, he was finally diagnosed as having multiple myeloma. The so-called shoulder pad sign, which is pathognomonic for light chain amyloidosis, although its detection remains a challenge for physicians, was a clue leading to the prompt diagnosis of the disease in the current case. The impact of articular manifestations on the diagnostic strategy for assessing multiple myeloma is also discussed.
Introduction
Multiple myeloma (MM) is a neoplastic disorder characterized by the clonal expansion of plasma cells derived from B cells. 1 MM has a propensity to cause a state of bone-remodeling turbulence that is associated with increased overall osteoclastic activity, resulting in hypercalcemia, which can range in presentation from asymptomatic to severe and lethal, one of the most common metabolic complications of the disease.2,3 In this report, we describe a male chronic hemodialysis (HD) patient who developed asymptomatic hypercalcemia associated with polyarticular swelling and was finally diagnosed with MM. Establishing the diagnosis of MM can be complex,4,5 although certain physical manifestations may occasionally help physicians to diagnose the disease promptly. The so-called shoulder pad sign, which is pathognomonic for light chain (AL) amyloidosis,6–8 although its detection remains a challenge for physicians, played such a role in the current case.
Case Report
A 76-year-old male was revealed to have hypertensive nephrosclerosis on a renal biopsy in the beginning of November 2011, at which time his serum creatinine (sCr) level was 4.84 mg/dL and his protein-to-Cr ratio (P/Cr) in a random urine sample was 1.27 g/g Cr. Two months later, he was enrolled in the chronic HD program due to a progressive decline in his renal function, with an sCr level of 10.0 mg/dL and spot urine P/Cr of 1.18g/g·Cr. He began to complain of symmetrical polyarthralgia at the beginning of February 2012. Thereafter, such symptoms worsened and swelling of multiple joints progressively developed around the end of June 2012, along with gradual elevation of the serum calcium level, although neither calcium-containing phosphate binder nor active vitamin D sterols were administered. The patient denied a history of inflammatory joint diseases, such as rheumatoid arthritis, as well as skin rashes and gastrointestinal symptoms. He was thus presumptively diagnosed as having idiopathic bursitis by a local orthopedic service, and symptomatic treatments – including rest, avoiding activities, and topical nonsteroidal anti-inflammatory therapy – were continued. Nevertheless, the range of motion in his shoulders, elbows, and hips remarkably decreased in the beginning of August 2012, at which time the serum calcium level further increased up to 11.7 mg/dL, despite combined management with HD using a low-calcium dialysate (Fig. 1). Remarkable distinctive swelling in the shoulders with a rubbery hard consistency associated with gross muscle hypertrophy was also detected at the end of August 2012 (Fig. 2A and B). Arthrograms revealed no skeletal deformities within the joints, while technetium-99m (99mTc)-pyrophosphate scanning showed a marginal uptake in the corresponding joints, including the shoulder, elbows, hips, knees, and ankles (Fig. 2C). Meanwhile, the white blood cell and platelet counts were maintained at almost constant levels, ranging from 4,000 to 5,000/μL and 14.6- to 16.0 × 104/mm3, respectively, while anemia gradually progressed despite the administration of human recombinant erythropoietin, ultimately requiring occasional transfusions of packed red blood cells. A further workup revealed the following data: immunoglobulin (Ig) G: 1,099 mg/dL; IgA: 22 mg/dL; IgM: 8 mg/dL; serum intact parathyroid hormone (PTH): 6 pg/mL; PTH-related protein (PTH-rP): 2.1 pmol/L; angiotensin-converting enzyme: 2.1 mU/mL; and beta-2-microglobulin, 31.6 mg/L. Rheumatoid factor was negative, as was an assay for antibodies to cyclic citrullinated peptides. A peripheral blood smear was unremarkable, and no atypical plasma cells were noted; however, analyses of urine immunoelectrophoresis showed an IgG kappa (K) monoclonal component and Bence Jones proteins (K type), despite the absence of a distinct serum electrophoretic spike (Fig. 3). In addition, a bone marrow biopsy performed in the middle of September 2012 revealed 50% plasma cells with K light chain restriction. Therefore, the patient was diagnosed as having stage IIB MM according to the Durie–Salmon criteria and stage III disease based on the international staging system for MM9–11 and was scheduled to receive chemotherapy for MM. Four months later, however, he died of fatal gastrointestinal bleeding despite the application of bortezomib-based therapeutic regimens.
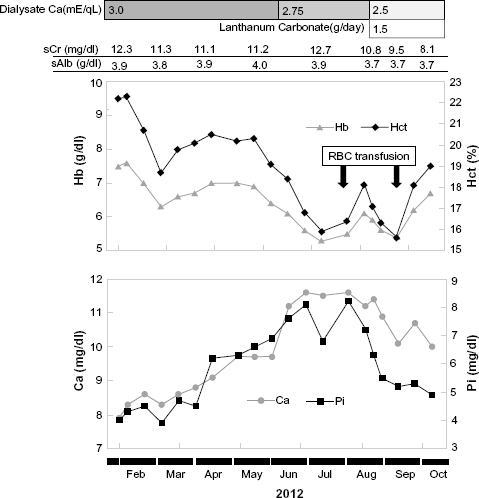
Serial changes in the hemoglobin, hematocrit, serum creatinine (sCr), serum levels of albumin (sAlb), calcium (Ca), and phosphorus (Pi) during the observation period. The level of sCa increased up to 11.7 mg/dL in August 2012 despite combined management with hemodialysis using a low-calcium dialysate. Thereafter, the patient received occasional red blood cell (RBC) transfusions for anemia.

Musculoskeletal findings. The shoulder masses, which appeared similar to shoulder pads worn by American football players, were firm and immobile. The masses were more prominent on the right than on the left (

Electrophoretic pattern of serum proteins (
Discussion
Hypercalcemia is not a rare concern in the ordinary clinical setting due to the widespread use of routine biochemical screening, 12 requiring the simultaneous evaluation of several parameters to define the disease status.3,13 Numerous causes for the development of hypercalcemia have been proposed, with primary hyperparathyroidism being the most common in ordinary ambulatory subjects, whereas hypercalcemia related to malignancy – including carcinoma of the bronchus, breast, head and neck, urogenital tract, as well as MM – is more common in some hospital-based populations.12,14 The precise incidence of hypercalcemia among patients with advanced chronic kidney disease (CKD) remains to be delineated, in part because transient elevation of serum calcium due to an excessive intake of calcium salts and vitamin D overdosing is very common15,16; however, it is necessary to stress that such patients are also susceptible to all diseases that may cause hypercalcemia in subjects without renal disease. 16
MM is a common hematological malignancy, with an overall worldwide incidence of 4.3 per 100,000 persons per year. 17 Hypercalcemia is most common in patients with MM having the greatest neoplasm volume, regardless of the serum PTH-rP status. The reasons for this phenomenon remain to be clarified, although it may depend on both the degree of bone-resorbing activity induced by myeloma cells and the glomerular filtration status. 2 The associatin between MM and renal insufficiency, as noted in the current case, is also not exceptional. Renal damage is usually moderate and reversible in approximately half of all cases, particularly related to precipitating factors such as hypercalcemia or volume depletion, although a small proportion of patients develop renal dysfunction severe enough to require renal replacement treatment. 18 On the other hand, several studies have demonstrated that the frequency of various neoplasms is higher in patients with end-stage renal disease than in the general population, especially in the kidneys and urinary tract.19–21 Although unsuccessful exclusion of end-stage renal disease subjects with prevalent MM from the cohort might result in the large excess of MM lesions soon after the commencement of renal replacement therapy, the risk of MM has been shown to be 5.2 times higher in subjects with end-stage renal disease than in the normal population. 20 Our failure to identify the precise time point of MM onset in the present case precludes us from evaluating the relative contribution of the disease to the development of end-stage kidney disease, while the electron microscopic analysis of the current patient's renal biopsy specimen did not detect the ultrastructural appearance of amyloid fibrils, thus leading us to conclude that the role of an amyloid-dependent pathology for the renal dysfunction at the time point of the procedure was marginal.
It should be noted that the initial manifestations of MM are sometime obscure and can include weight loss, malaise, fatigue, and bone pain. 22 Similarly, the symptoms of progressive CKD are nonspecific, and thus nephrologists, as well as primary care physicians and hematologists/oncologists, should consider the possibility of plasma cell dyscrasia as an underlying cause in patients with a wide variety of presenting complaints. 22 In the current case, the diagnosis of MM as the cause of the patient's sustained hypercalcemia was straightforward after confirming the presence of a monoclonal component in the serum and urine specimens. Hence, one may argue that a clinical picture including hypercalcemia, renal failure, and MM is too common to be described in the literature. Nevertheless, we believe that the clinical significance of our experience must be evaluated more carefully in that the characteristic musculoskeletal manifestations were clues to obtaining a prompt diagnosis of the disease in the current case.
Polyarticular swelling associated with stiffness and a diminished range of motion is recognized to be a characteristic symptom of rheumatoid arthritis.23,24 Although the prevalence of this physical sign may be minor, it can be a diagnostically significant manifestation in some subsets of patients with AL amyloidosis caused by MM.25–27 Indeed, previous reports contain several references to the occurrence of multiple-joint swelling in association with MM, drawing attention to the fact that such manifestations may be attributed to the onset of AL amyloidosis mediated by the infiltration of amyloid proteins to the dependent portion of the skeletal and periarticular structures.6–8 Alternatively, or in addition, gross skeletal muscle pseudohypertrophy has been described as a phenotype of amyloid myopathy in several previous cases.28–31 From a clinical point of view, musculoskeletal involvement is rare in patients with systemic amyloidosis,25,27 although its development may be a pivotal clue for making a prompt diagnosis of the disease. In the current patient, we believe that the polyarticular swelling and bodybuilderlike appearance of the upper torso muscles are linked to AL amyloidosis associated with MM and that this characteristic shoulder manifestation can be regarded as the shoulder pad sign, a feature pathognomonic for AL amyloidosis.6–8 Although not all cases of MM are necessarily complicated by this disease, AL amyloidosis is found in up to 30% of patients who present with MM. 17 Moreover, it is likely that the frequency of this condition would be higher if diligent assessments for amyloid aggregates were conducted in subjects with MM at autopsy. 25 Pathological evaluations are mandatory for obtaining a definitive diagnosis of tissue injury resulting from amyloidosis, 31 and it has been proposed that investigations of the synovial fluid may be an option for definitively diagnosing arthropathy mediated by AL amyloidosis. 25 Nevertheless, one may be exempt from performing such invasive techniques during the diagnostic process in particular subjects due to findings of a characteristic physical appearance and/or significant concerns regarding bleeding in cases of advanced myeloma-associated amyloidosis,29,32 as was the case in the current patient. We feel that such a heterogeneous stance for a pathological evaluation may mirror the lack of standardization of policies for the selection of patients eligible for tissue biopsies, presumably due to the rarity of the disease. Otherwise, imaging analyses using radiopharmaceutical agents may be used as an alternative diagnostic procedure. Indeed, myocardial accumulation of bone-seeking tracers has been demonstrated anecdotally in cases of cardiac amyloidosis, 33 and a positive99mTc-pyrophosphate uptake in the corresponding portions manifesting the shoulder pad sign in a patient with AL amyloidosis has been reported. 7 Considering the negative results obtained in the current case, however, the diagnostic impact of this modality in the overall patient population with amyloid arthropathy requires a careful evaluation. Finally, we believe that the optimal diagnostic strategy will be determined only when more experience with cases similar to ours has been accumulated.
We feel that obtaining an accurate and prompt diagnosis of musculoskeletal disorders resulting from AL amyloidosis associated with MM and identifying characteristic physical manifestations, such as the shoulder pad sign and grossly hypertrophied muscles with a pseudoathletic appearance, remains a challenge for physicians. Although we failed to confirm the clinical benefit of bortezomib-based regimens, as has been demonstrated in several studies of MM subjects with various degrees of renal failure,10,34 the current report emphasizes the pitfalls in evaluating patients with several musculoskeletal manifestations associated with paraproteinemia, a matter requiring continuous and careful attention,8,26,30 thus leading to a high index of suspicion with prompt recognition and immediate intervention for the disease.
Author Contributions
SI and TA drafted the manuscript. SI and HI made contributions to the acquisition of the clinical data. EK and DN provided a detailed review of the contents and structure of the manuscript, resulting in significant changes to the original document. All authors have read and approved the final manuscript.