
Abstract
We encountered three adult patients with flu-like symptoms diagnosed with human parvovirus B19 (HPV-B19) infection. Blood serum analysis also revealed leukopenia, with white blood cell counts (WBCs) of 1,000–2,000/mL and low platelet counts of 89–150 × 109/L. Typical skin rash was absent in one patient. Bone marrow examination of another patient showed hypoplastic marrow with <5% blast cells. All patients recovered without administration of granulocyte colony-stimulating factor (G-CSF). Therefore, HPV-B19 infection with leukopenia should be considered in adult patients with leukopenia during erythema infectiosum epidemics, even if typical clinical findings (ie, skin rash) are absent. Further, the fact that three cases were observed over the stated time period at our hospital, which is located in Nagoya city, showed a transition to a slightly higher level of incidence than the annual average.
Introduction
Human parvovirus B19 (HPV-B19) infection is generally encountered in 4- to 10-year-old children. 1 Aside from asymptomatic mild flu-like symptoms, most children present with typical symptoms of erythema infectiosum (slapped-cheek rash) because the primary targets are erythroid progenitor cells. Because the temporary bone marrow infection causes transient erythropoiesis arrest, 2 this infection is particularly problematic for patients with hematological disorders, such as chronic hemolytic anemia, which includes sickle cell disease, hereditary spherocytosis, and infection with human immunodeficiency virus (HIV). 1 During HPV-B19 infection, these patients fail to increase erythroid progenitor cell formation to compensate for red blood cell lysis, leading to acute erythroblastopenia (aplastic crisis). Therefore, it is important to diagnose all cases of HPV-B19, even if the infection generally subsides without medication, in case the patient has an undiagnosed hematological disorder.
Immunity prevalence for HPV-B19 increases with age and exceeds 60% in adults. 3 However, cases of infection have been reported in adults, most of which present milder erythema infectiosum, arthralgia, and purpuric papular eruptions on hands and feet (gloves and socks syndrome). 1 We encountered three cases of HPV-B19 in adult patients presenting with unusual symptoms, such as leukopenia and low platelet counts. The patients have given consent for the publication of this report.
Case Report
Case 1
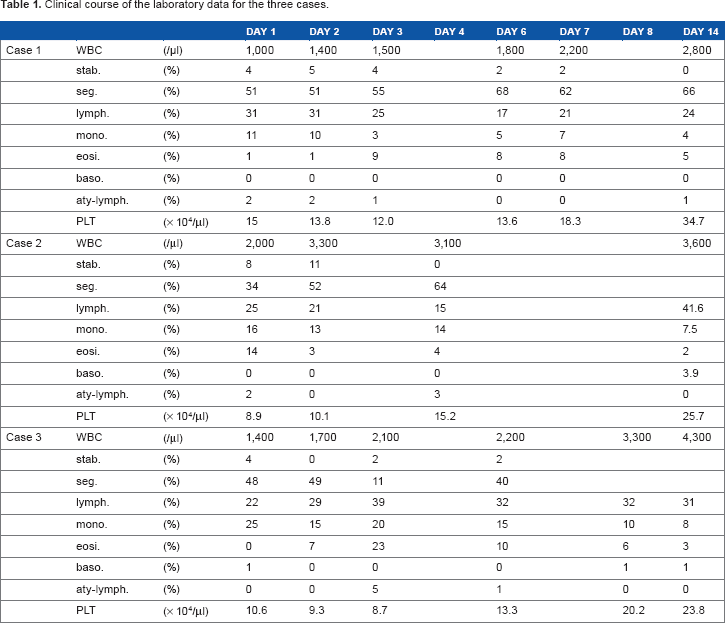
The patient was a 40-year-old female office worker with no children. There was no indication of cytopenia in past health examinations. On 16 January 2011, the patient developed a fever of 39 °C, systemic pain, fatigue, and loss of appetite. Therefore, she was transferred to our emergency outpatient department on 18 January 2011. However, she tested negative for influenza and was discharged. Because the symptoms persisted, the patient was readmitted to our hospital on 19 January 2011. Her body temperature was 38.7 °C, and neither lymphadenopathy nor rashes were present. Leukopenia (1,000/μL) and low platelet counts (15 × 104/μL) were observed (Table 1). The patient tested negative for HIV-1 and HIV-2 antibodies, and her HPV-B19 immunoglobulin M (IgM) antibody titer was 2.64. In all, 14 days later, the patient showed a leukocyte count of 2,800/μL and a platelet count of 34.74 × 104/μL, which were indicative of recovery.
Clinical course of the laboratory data for the three cases.
Case 2
The patient was a 36-year-old housewife, with children aged 2 and 7 years, who were not suffering from erythema infectiosum. There was no indication of cytopenia in past health examinations. Starting on 5 August 2010, the patient experienced general fatigue and a mild fever of 38 °C. On 9 August 2010, the fever progressed to 39 °C, and the patient noticed erythema on her extremities and trunk. Therefore, she was admitted after examination to our internal medicine outpatient department on 10 August 2010. She had no lymphadenopathy on admission but had lacy erythematous rashes on her trunk and bilateral upper extremities and thighs. Leukopenia (2,000/μL) and low platelet counts (8.9 × 104/μL) were observed (Table 1). The patient tested negative for HIV-1 and HIV-2 antibodies, and her HPV-B19 IgM antibody titer was 11.63. In all, 14 days later, the patient showed a leukocyte count of 3,600/μL and a platelet count of 25.7 × 104/μL, which were indicative of recovery.
Case 3
The patient was a 31-year-old female office worker (number of children not disclosed). There was no indication of cytopenia in past health examinations. Starting on 12 December 2010, the patient experienced flu-like symptoms of pharyngodynia and fatigue. The patient also observed rashes on the trunk and extremities the following day. Therefore, she was admitted following examination to our internal medicine outpatient department on 15 December 2010. Her body temperature was 38.2 °C, and there were rashes on her trunk and extremities. Leukopenia (1,400/μL) and low platelet counts (10.6 × 104/μL) were observed (Table 1). Bone marrow examination showed bone marrow hypoplasia, but blast cells were below 5%. The patient tested negative for HIV-1 and HIV-2 antibodies, and her HPV-B19 IgM antibody titer was 2.24. In all, 14 days later, the patient showed a leukocyte count of 4,300/μL and a platelet count of 23.8 × 104/μL, which were indicative of recovery.
The fact that three cases were observed over the stated time period at our hospital, which is located in Nagoya city, was indicative of a transition to a slightly higher level of incidence than the annual average (Fig. 1; according to documents from Port of Nagoya's public health center).
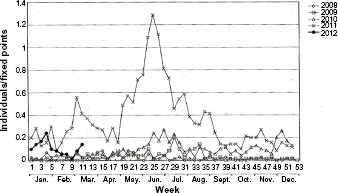
Erythema infectiosum. Trends in the weekly patient incidence rate for each fixed point in Nagoya City.
Discussion
We encountered three cases of acute HPV-B19 infection in adult females for which a definitive diagnosis is made by confirming the presence of HPV-B19 IgM antibodies or an increase in IgG antibody titer paired serum. In these cases, an increase in HPV-IgM antibodies was observed in blood tests upon admission. Hayakawa et al. 4 reported the clinical findings of 21 consecutive patients with adult HPV-B19 infection. In that report, the predominant signs and symptoms were fever exceeding 38.3 °C (81%), skin rash (47.6%), arthralgia/myalgia (61.9%), general fatigue (42.9%), lymph node swelling (38.1%), edema (38.1%), and petechiae (14.3%). In our cases, the predominant signs and symptoms were fever exceeding 38.2 °C (100%), general fatigue (100%), skin rash (66.6%), and arthralgia/myalgia (33.3%). They also exhibited concomitant leukopenia and low platelet counts. Because hematopoietic disease could not be excluded, bone marrow aspiration was conducted in one case, but no obvious hematopoietic dysfunction profile was observed.
Cases of acute HPV-B19 infection exhibiting leukopenia and low platelet counts have been reported sporadically over the past 15 years.5–11 Although there are various theories regarding the cause, nothing has been specified. There are reports of a connection with hemophagocytic syndrome accompanying infection,12–15 but bone marrow examinations did not reveal a hemophagocytic profile in any one of our three cases, and the involvement of hemophagocytic syndrome could be excluded based on their clinical courses.
Furthermore, B19 receptors are believed to be erythrocyte-like P antigens,16–18 which lead to anemia in patients with a background of accelerated erythropoiesis (eg, hemolytic diseases). Precursor cells outside the hematopoietic stem cell erythroid lines can also be infected, and some are of the opinion that this causes leukopenia. 19 However, bone marrow is not necessarily hypoplastic in cases with B19-induced neutropenia, and in bone marrow examinations in case 3, no hypoplasia was observed. Sakai et al. 20 suggested that neutropenia caused by B19 is not because of the direct effect of the virus but rather because of secondary leukocyte elimination and consumption. In addition, there are reports that anti-neutrophil antibodies are commonly detected in chronic neutropenia in infant B19 infections. 21 It is also suggested that the mechanism of B19-induced leukopenia and low platelet counts may be different from that of anemia.
Furthermore, although it is unknown whether there was a decrease in serum granulocyte colony-stimulating factor (G-CSF) as quantification of serum G-CSF was not conducted in any of our three cases, none of the cases required G-CSF administration. There are reports of G-CSF administration, 5 but administration is considered unnecessary in the absence of serious life-threatening complications such as septicemia.
As the other complications, HPV-B19 has been reported in association with a wide range of diseases and clinical manifestations, including arthritis, vasculitis, myocarditis, nephritis, lymphadenitis, immune thrombocytopenia (ITP), meningitis and encephalitis, hemophagocytic syndrome, fulminant liver disease, and generalized edema, as well as many other conditions. 22 Also, the observation that many cases of chronic fatigue syndrome (CFS) begin with a flu-like illness prompted the hypothesis that viral infections were implicated in the disease, and several viruses were suggested as etiological agents for CFS. HPV-B19 has been reported to be one of these viruses.23,24
In conclusion, we encountered three adults who were diagnosed with acute HPV-B19 infection after the simultaneous observation of acute flu-like symptoms, leukopenia, and low platelet counts. This case series emphasizes that the epidemic period should also be considered and HPV-B19 infection should be actively suspected in adult patients with hematocytopenia even if typical clinical findings (ie, skin rash) are absent.
Author Contributions
Conceived and designed the experiments: DY. Analyzed the data: DY. Wrote the first draft of the manuscript: DY. Contributed to the writing of the manuscript: DY, NM, MM. Agree with manuscript results and conclusions: DY, NM, MM. Jointly developed the structure and arguments for the paper: DY, NM, MM. Made critical revisions and approved final version: DY, NM, MM. All authors reviewed and approved of the final manuscript.