
Abstract
Superior mesenteric artery (SMA) syndrome is a mechanical duodenal obstruction by the SMA. The traditional approach to SM A syndrome was open bypass surgery. Nowadays, a conventional approach has been replaced by laparoscopic surgery. But single incision laparoscopic approach for SMA syndrome is rare. Herein, we report the first case of SMA syndrome patient who was treated by single incision laparoscopic duodenojejunostomy.
Introduction
Superior mesenteric artery (SMA) syndrome is defined as a compression of the third portion of the duodenum in between the SMA and the aorta. It is a rare disease that causes many symptoms including postprandial abdominal pain, anorexia, nausea, vomiting, and subsequent weight loss.1–3 Bypass surgery is indicated in patients, when the conservative treatment is failed. The most common surgical procedure for SMA syndrome was laparoscopic duodenojejunstomy. 4
Herein, the authors report the successful single incision laparoscopic duodenojejunostomy for a patient with an SMA syndrome.
Case Report
A 75-year-old male, 170 cm, 60 kg, presented to our hospital with vomiting for 1 week and 7 kg weight loss for 2 months. Two years ago, he found duodenal ulcer and took medicine for 2 months. He was a smoker and a social drinker.
On admission, plain abdominal film showed a distended stomach. Laboratory studies were within normal limits. An abdomen computed tomography (CT) revealed a severely distended stomach and distal duodenum with obstruction at the level of the SMA (Fig. 1A). On CT examination, an aorto-mesenteric angle was narrow to 15° and an aorto-mesenteric distance was short 8 mm (Fig. 1B).
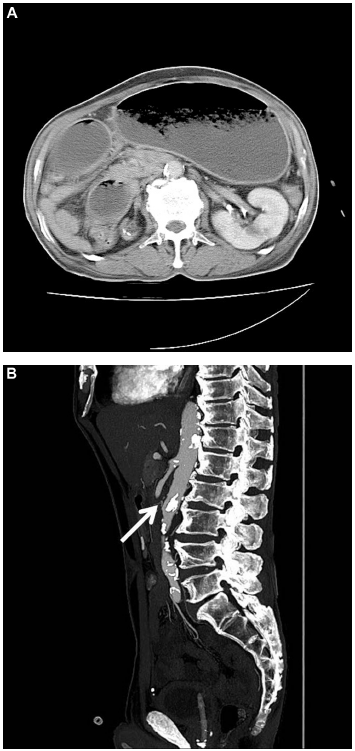
Abdomen Computerized Tomography. (
After insertion of nasogastric tube, the amount of drainage was more than 2000 cc a day. Because of much food in his stomach, esophagogastroduodenoscopy was failed. For 1 week, the patient was treated conservatively by providing parenteral high caloric nutrition. But the amount of drainage from a nasogastric tube was not decreased (>2000 cc/day). He refused a conservative treatment and wanted to have surgery.
The patient under general anesthesia was placed in the dorsal lithotomy position. The operator stood between patient's legs. On the patient's left side, the first assistant handled the scope.
First, the trans-umbilical 1.5 cm incision was made with the Hasson technique. After making incision, we used a four channel Octo-Port (DalimSurgNet, Seoul, Korea). After upward traction of a transverse colon, a dilated duodenum was easily identified. We made two small incisions at proximal jejunum (20 cm from a treitz ligament) and duodenum (anterior wall at second portion). And we inserted a 45-mm Endo-GIA™ (Covidien, New Haven, CT) in order to create a side-to-side duodenojejunostomy. The common entry hole was closed by hand-sewn continuous running suture.
A drain was placed to the duodenojejonostomy site via port incision. The operation time was 180 minutes.
His postoperative course was unremarkable. An upper gastrointestinal study on postoperative day 4 showed good patency of the anastomosis. The patient was discharge uneventfully on the fifth postoperative day.
One month later, when he visited our clinic, he had gained 6 kg.
Discussion
SMA syndrome was first described in 1861. 5 This syndrome is characterized by typical symptoms (vomiting, nausea, weight loss, and knee-chest position).1–3 The actual incidence is unknown since the diagnosis is not frequently pursued.4,6 SMA syndrome has been associated with prolonged confinement in the supine position, loss of weight, loss of abdominal wall muscle tone, application of a body cast, and severe burns.7–9 Females and young adults are more likely to be affected by the condtion.4,10
Our case was a 75-year-old male. He did not have a past medical history associated SMA syndrome (eg, immobilization, burn, or hidden malignancy). And we could not find any abnormality except a distended stomach and duodenum from his CT scans.
Radiologic studies (upper gastrointestinal barium study, angiography, or abdomen CT) have been established as definitive diagnostic tools for SMA syndrome. Recently, abdomen CT has been replaced with an angiography. It can show the dilated 1st and 2nd portion of duodenum and the 3-dimensional image of the aorta, SMA, and spine. In SMA syndrome, the angle between the aorta and SMA is decreased to 6–25° and a shortened aroto-mesenteric distance of 2–8 mm.11,12
Non-operative treatment is recommended as initial therapy of the SMA syndrome. But, when the conservative treatment has failed, surgery is often required as a curative treatment for SMA syndrome.
After the first successful operative treatment, a duodenojejunostomy in 1908, 13 SMA syndrome has been treated by a laparotomy with duodenojejunostomy.
Postoperative sequelae, such as pain and complications, affect not only the patient's general wellbeing but also increase perioperative morbidity and the length of hospital stays. Because of these reasons, laparoscopic surgery, which has the benefits of a small wound, diminished postoperative pain, and decreased hospital stay has been widely accepted and is used for treatment of many diseases. Advances in laparoscopic skills and instruments have enabled surgeons to perform a laparoscopic surgery.
In 1998, Gersin performed the first laparoscopic duodenojejunostomy for treatment of SMA syndrome. 14 Nowadays, the most common surgery for SMA syndrome is a laparoscopic duodenojejunostomy. 4 Furthermore, a reduced port or single incision laparoscopic surgery (SILS) has been adapted for benign disease.15–17 However, the introduction of SILS, SILS is not widely performed except a cholecystectomy, appendectomy, or gynecologic surgery.15–17 SILS has longer operative time and more difficulties than conventional laparoscopic surgery.16–19
There were several case reports about “laparoscopic duodenojejunostomy for SMA syndrome.”4,10,20,21 Most of them reported a good surgical outcome or success.4,10,20,21 A conventional laparoscopic duodenojejunostomy (three to four ports) took 1 hour and 35 minutes to 3 hours. 20 In this regard, our operation time (3 hours) was not longer than these.
A duodenojejunostomy is a simple procedure that makes an anastomosis for bypass and the loss of his visceral fat made us easily identify a dilated duodenum and a proper surgical plane. So we decided to perform a SILS approach instead of a conventional laparoscopic approach.16–19 It is true that SILS is ergonomically more stressful for the surgeon than the standard laparoscopic approach.
There are still debates on SILS. Some reports about SILS have failed to demonstrate the superiority to conventional laparoscopic approach (eg, cosmesis, wound pain, and surgical site infection). 22,23 But there were several reports that favored SILS.15,16,24,25
The surgical instrumentation and techniques have been improved. Thereby, the SILS approach will be more convenient for surgeons, and this approach may be beneficial for selected cases.
In this report, we describe the first known case, to our knowledge, of single incision laparoscopic duodenojejunostomy for SMA syndrome.
Author Contributions
Conceived and designed the experiments: SK, YSK. Analyzed the data: SK, YDM. Wrote the first draft of the manuscript: SK. Contributed to the writing of the manuscript: SK, YSK. Agree with manuscript results and conclusions: SK, YSK, YDM. Jointly developed the structure and arguments for the paper: SK, YSK, YDM. Made critical revisions and approved final version: SK, YSK, YDM. All authors reviewed and approved of the final manuscript.