
Abstract
Schwannoma is a tumor that develops from nerve sheath. The authors report an unusual case of schwannoma of the median nerve (MN) that remained asymptomatic for four years. The diagnosis was based on MRI (magnetic resonance imaging) and histopathological examination. Surgical removal is usually curative. The asymptomatic character of the tumor and its slow evolution remain an essential factor in diagnosis delays. This tumor has a good prognosis with a low recurrence rate and potential for malignant transformation.
Introduction
Schwannoma is the most common benign tumor of the peripheral nerves. 1 It grows at the expense of Schwann cells of the nerve sheath. It is an encapsulated lesion rarely causing neurological deficit and is usually extirpable. 2 Although they commonly appear as solitary lesions, occasionally there can be multiple (schwannomatosis) lesions or a lesion associated with neurofibromatosis. 3 The median nerve (MN) is one of the most affected peripheral nerves. Schwannomas arising from Schwann cells are usually benign tumors and comprise 0.8–2% of all hand tumors. 4 The tumor is usually seen as a painless, asymptomatic mass, hence the risk of diagnostic delay. Pain, paresthesias, and motor weakness may occur when the tumor reaches sufficient size.4,5 EMG (electromyography), MRI (magnetic resonance imaging), and USG (ultrasonography) are helpful in the diagnosis. Surgical removal is usually curative. 6 We report an unusual case of schwannoma of the MN whose diagnosis was made four years after the appearance of swelling.
Case Report
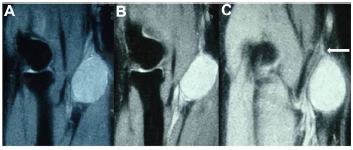
A 26-year-old man presented with a mass at the anterior side of his forearm. On clinical examination, there was a painless solid mass 4 cm in length, little sensitive to pressure, firmly attached to deeper tissues. Percussion over the mass produced a Tinel's-like sensation along the MN. The pain was not severe enough to disturb sleep or to hinder physical activities. The patient reported that he first palpated a nodule four years ago that grew up very slowly to the current size. There was no family history of neurofibromatosis and no associated clinical features. The ultrasound showed that the mass was subcutaneous although limited and homogeneous measuring 3 cm in diameter. An MRI examination revealed a 3-cm long, well-circumscribed mass in close proximity to the neurovascular bundle of the upper extremity of the forearm, which had hyperintense signal on T2-weighted images. The appearance was compatible with a tumor of nervous origin (Fig. 1A–C, arrow). A longitudinal incision centered over the tumor bulk was performed (Fig. 2). Surgical exploration brought to light an encapsulated tumor firmly attached to the MN, which was easily resected. Histological examination of the tumor showed the characteristic pattern of benign schwannoma: non-nucleated fibrillar areas lined by a palisade of Schwann cell nuclei (Fig. 3). At 10 months follow-up, the wound healed well with no pain or sensorimotor deficit.
(

Operative view: oval-shaped capsulated mass in eccentric position along the MN.

Histological examination of the tumor showing characteristic pattern of benign schwannoma: non-nucleated fibrillar areas lined by a palisade of Schwann cell nuclei (hematoxylin and eosin stain, original magnification × 200).
Discussion
Schwannomas are common, slowly growing, and encapsulated benign nerve sheath neoplasms separated from the surrounding tissues. Some forms may be localized within the nerve trunk or bundles of nerve fibers spreading over the surface of the tumor. 5 They most commonly occur in adults between 20 and 50 years of age, without distinction of gender, with an approximate one sex ratio. 7 They generally appear as solitary lesions. Occurrence of multiple schwannomas is rare and not necessarily correlate with neurofibromatosis, which demonstrates very precise chromosomal alterations. 8 Malignant transformation of benign schwannomas is unusual. 9 Schwannomas can be asymptomatic or can produce pain, a positive Tinel's sign or a Tinel's-like sensation, and sensory alterations. The slow growth pattern of benign nerve tumors allows for adaptation of the nerve function to the pressure effects.3,10 The slow growth and the nervous adaptation to the increased volume of the tumor is often the factor responsible for the diagnostic delay. In a study of 14 cases of schwannomas of the upper limb, Akambi Sanoussi and Dubert analyzed the time between the onset of clinical symptoms and surgery; this period was nine months on average (two months to seven years). 2 MRI can provide useful information about morphological data on the MN tumors; however, it cannot provide dynamic information. 5 Although low-intense signals on TI-weighted images and hyperintense signals on T2-weighted images are common findings of schwannomas, 6 MRI also give useful information regarding tumor extent, anatomical location, tumor size, and relationship of peripheral nerve, and for appropriate planning of surgical therapy and preoperative diagnosis. EMG studies may reveal prolonged sensory latency and diminished or absent sensory-evoked potentials.5,11 Malignant transformation in schwannomas is rare, the risk of malignant transformation being approximated at 18% in neurofibromatosis type 1 and 5% in schwannomas. In all, 14 patients with von Recklinghausen disease carry a worse outcome. In von Recklinghausen disease, neurofibromatosis associates multiple nerve sheath tumors. Patients may have simultaneous different histological types of nerve tumors, such as neurofibromas, and malignant nerve sheath tumors. 12
Surgical excision is the treatment of choice. Schwannomas are theoretically removable because they repulse fascicular groups without penetrating them, thus allowing their enucleation while preserving nerve continuity,13,14 as reported in our patient. Some authors recommend excision of only symptomatic tumors or those demonstrating enlargement during follow-up. 6 Other authors showed that the size of the tumor, longer history, or presence of preoperative neurological symptom correlated with the incidence of neurological deficit 15 ; hence, we recommended early surgical excision to have better clinical outcome and to avoid postoperative neurological deficits. This is the reason why early diagnosis is important for this type of tumor. Paresthesia is the most frequent postoperative complication. Nerve grafting may also be required in some malignant forms of these tumors.5,16
Conclusion
Schwannomas are benign nerve tumors. Their diagnosis is often delayed by the absence of clinical symptoms due to the nervous adaptation to the increased volume of the tumor. Hence, the need to think about this type of tumor before any mass in the path of peripheral nerve.
Author Contributions
MB conceived and designed the experiments. MA analyzed the data. AR wrote the first draft of the manuscript. MA contributed to the writing of the manuscript. MM and AE agreed with manuscript results and conclusions. MB jointly developed the structure and arguments for the paper. ME made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.