
Abstract
Cardiac echinococcus is a rare affliction of the heart caused by the tapeworm Echinococcus granulosus. Primary echinococcosis of the heart represents 0.5–2% of all hydatid disease cases in endemic regions. It evolves slowly, explaining its rarity in children. We report the case of a 11-year-old child affected by a giant cardiac cyst of the left ventricle (LV). The patient underwent cardiac surgery and medical treatment. A retrospective review of the current literature was realized. We found 18 cases: the mean age was 11-years old. Nine cysts were localized in the LV, four in the interventricular septum, three in the right ventricle, and two in the right atrium. All underwent surgery except six patients. Routine echocardiographic screening may be useful in endemic regions where infestation is common. Cardiac echinococcus should be diagnosed in the early and uncomplicated stages and be removed surgically even in asymptomatic patients.
Introduction
Hydatid disease (HD) is mostly caused in humans by Echinococcus granulosus. It has a worldwide distribution with higher prevalence in South Europe, South America, Africa, Turkey, Australia, New Zealand, and India, affecting more childhood than adulthood. 1
Hydatid cyst (HC) was first seen in the intestine of sacrificed animals in the Talmud of Babylonia. Cardiac HC was described by May in 1639. 2 In 1921, Martin and De Crespign performed the first surgical treatment. The utilization of extracorporeal circulation for this purpose took place in 1961. 3 Cardiac echinococcosis (CE) are extremely rare, especially in children, representing 0.5–2% of all human cases. 4 The most commonly affected cardiac chamber is the left ventricle (LV) (55–60%). 5 CE is often asymptomatic until the cyst has grown to large dimensions, which often occurs in 1–5 years. Presentation in pediatric patients is uncommon because of the slow growth of the cyst by approximately 1 cm per year. 6 An epidemiologic study from Benghazi 7 showed that only 11.7% of patients were under 10 years old. Most of the reports in the recent literature concern adult patients. 8 The authors will describe the case of a 11-year-old female affected with echinococcus of the LV and review the literature of CE affecting young children.
Case Report
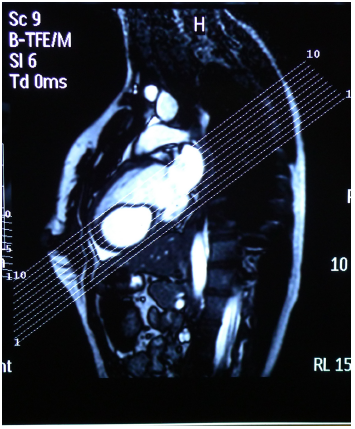
A 11-year-old female living in a rural area in Turkey presented to the Emergency Department with a history of left-sided chest pain and palpitation. Her pulse was regular, with a heart rate of 79 bpm and her blood pressure was 120/80 mmHg. Heart sounds were normal with no murmur. Results of hematologic and biochemical laboratory exams were normal. Chest X-ray showed a localized bulge at the apex of the heart and electrocardiography (ECG) revealed T-wave inversion in leads I, II, aVL, and V4-V6. Transthoracic echocardiography (TTE) demonstrated a subepicardial echolucent cyst measuring 9 × 6 cm on the left ventricular free wall. Cardiac magnetic resonance imaging (MRI) revealed a large lesion from the myocardium of left ventricular free wall (Fig. 1). Thoracic computed tomography (CT) of the lungs identified no additional organ involvement and abdominal ultrasounds were negative. Diagnosis of CE was made and the patient was referred for cardiac operation. Cyst liquid was evacuated and hypertonic serum was injected in the cyst several times and the pseudomembrane was removed (Fig. 2). Once systemic contamination was prevented, the cyst was widely opened and thoroughly excised under cardiopulmonary bypass (CPB). Histologic examination confirmed the diagnosis of HC and ELISA test was positive for echinococcosis. Patient started medical treatment with albendazole (400 mg twice daily for 12 weeks) and was discharged on seventh postoperative day. Patient was symptom free with no complications 18 months after surgery and no cyst recurrence was seen during this period.

Cardiac MRI confirming the hydatid cyst.

Cyst membrane.
Lateral view cardiac cyst.
Review
We retrospectively reviewed the medical records of cardiac HCs in children before May 2012 using Pubmed and OVID searching the terms: “cardiac cyst in children,” “hydatid cyst,” “Echinococcus granulosus,” and “surgical approach.” All papers not in English were excluded. Only patients ≤16 years of age were included. Eighteen patients were included in the review9–23 with a mean age of 11. Five were females and 13 were males. Eleven patients lived eastern and southeastern parts of Turkey and dealt with animal husbandry. The others were from India (three cases), Spain (two cases), Libya (one case), and Greece (one case) (Table 1). Common symptoms were dyspnea, cough, weight loss, and fever. Two patients had cerebral events with right hemiparesis and cerebral confusion and one patient also had lower extremity ischemia. Nine cysts were in the LV, three in the right ventricle (RV), four in the interventricular septum (IVS), two in the right atrium (RA), and seven had multiorgan involvement. All laboratory tests were positive except for two. One patient underwent emergency surgery, and six were operated in elective surgery. All patients except one underwent CPB with cystectomy by deroofing the cyst and removing the parasite and capitonnage by reducing the size of the cyst cavity coapting the cyst wall by enrolling the edges of the parenchyma into the cavity.
Cases of cardiac cyst in children worldwide.

Five patients did not undergo surgery. One was waiting for surgery at the time. There was one immediate death and one patient died due to complication with pulmonary emboli (PE). Albendazole was used in seven patients post-operatively and mebendazole was used in five patients. At follow-up all survived patient were doing well, and the patients under medical treatment had no reduction in the size of the cyst.
Discussion
The term HC (“watery vesicle”) was coined by Rudolti in 1800 and derives from Greek word “hudatis” which means “drop of water.” 24 The life of the cyst in humans averages from 10 to 20 years. Karl von Siebold in 1853 demonstrated that the cycle of the human tenia is caused by the larval stages of cestodes (tapeworms) of the genus Echinococcus. 25 Dέvέ in 1928 stated that HC of the heart is primary and single even in those cases with other localization. 5 LV free wall is involved most frequently (55–60%), due to embolization through the left anterior descending artery followed by IVS (5–9%), RA wall (3–4%), RV myocardium (15%), LA (8%), pulmonary atrial (7%), and pericardial (8%). 5 The cyst may either localize in the ventricular wall, apex, outflow tract or spread from the left ventricular wall to the ventricle septum. 26 HCs of LV are usually subepicardial and rarely rupture in the pericardial space. Cyst in the septum can cause disturbance of conduction and atrioventricular (AV) block. Intracardiac HC may also lead to valve destruction, necessitating valve replacement. RV localization is subendocardial and intracavitary rupture is more frequent causing PE. In some cases, the differentiation between a myxoma and HC is made only after surgical removal. The pericardial space is another possible site of invasion. While the pericardium invaded by the HC has an inflammatory reaction leading to constrictive pericarditis over time, endocardium does not react and is therefore easily invaded by the cyst. 27 Symptoms are not always present and depend on the location of the cyst. Patient's symptoms can include allergic reactions, heart failure, arrhythmia's, heart block, and dyspnea. It may also present with non-specific features like weight loss, dyspnea, fever, and chest pain.4,5,8,27 Symptoms such as hemiparesis, lower ischemia, and vomiting can manifest because of complications.18,19 Diagnosis of HD of the heart should be made in the early and uncomplicated stages of the disease prior to the occurrence of any one of its common and dreaded complications. 28 Diagnosis can be done with Chest X-ray showing deformity in cardiac silhouette and calcifications in all projections. 29 Intramural fibromas, even if extremely rare, should be excluded. Because of compression of myocardial fibers, ECG can show abnormalities such as changes in the QRS complex, AV blocks, or S-T segment elevation.29,30 Echocardiography can demonstrate multiloculated cystic nature of the lesion as well as the presence of daughter cysts. It is a reliable technique for diagnosing intracardiac masses, but in some cases the echo-lucent and multiseptate nature of echinococcal lesions may be absent. Thus, in the appropriate clinical settings, echinococcal infections should be included in the differential diagnosis of tumor-like lesions of the heart. 31 The non-invasive nature of the modality and lack of cardiac motion artifacts, which occurs with multidetector cardiac computed tomography and MRI, makes the echocardiography the modality of choice in imaging cardiac HD.32,33 Non-contrast CT should be done to detect localized or segmental calcification.34,35 MRI HC is mostly a hypotense lesion on T1-weighted images and hypertense on T2. After contrast, ring enhancement, which represents the pericyst, can be detected. CT scan and MRI should be reserved especially for extracardial involvement.33,35
TTE is helpful for both diagnosis and surgical treatment of the cyst, and to establish the cardiac cyst characteristics. Atilgan et al removed two cyst under trans-esophageal echocardiography (TEE) guidance successfully in an adult. 4 Tufekcioglu et al performed TEE and TTE on all the 16 patients and proposed a scheme for echocardiographic classification of CE lesions based on the World Health Organization (WHO) classification.36,37 To evaluate outflow tract obstruction and the status of coronary arteries, cardiac catheterization and angiography may be useful,38,39 but can cause the rupture of the cyst. Angiography and scintigraphy are useful for pulmonary hydatid embolism diagnosis. 39
Serologic tests like the Casoni test are not very reliable with frequent false-positive and false-negative results up to 30%. ELISA test has a sensitivity of 91% and specificity of 82%. 40
Immunodiagnostic tests should be used before invasive methods. False-positive reactions may occur in persons with other helminthic infections, cancer, and chronic immune disorders. Indirect hemagglutination (IHA), indirect fluorescent antibody tests, and enzyme immunoassays (EIA) are sensitive tests for detecting antibodies in serum of these patients; sensitivity rates vary from 60% to 90%, depending on the characteristics of the cases. Crude HC fluid is generally employed as antigen. At present, the best available serologic diagnosis is obtained by using combinations of tests. EIA or IHA are used to screen all specimens; a positive reaction is confirmed by immunoblot assay or any gel diffusion assay that demonstrates the echinococcal “Arc 5.” 41
Acute rupture of the cyst may cause massive PE, hemispheric stroke8,26 especially when the cyst is located in the left side, acute abdominal aortic embolism or embolization of femoral artery 42 but also IVS dissection, secondary localization in the pericardium, chronic pericarditis (hydatopericardium) with signs of compression or be even invasive with pseudoaneurysmatic form,29,43 obstruction of cardiac orifice, metastatic visceral echinococcosis, hydatid allergy with anaphylactic reaction, sudden death. 8
Late complications are metastatic echinococcosis of the lesser or systemic circulation due to the dissemination and colonization of the scolex, or embolization of the fragmentation of the cyst membrane leading eventually to death. 29
Albendazole is preferred for its greater absorption in the gastrointestinal tract and higher plasma levels although reversible abnormalities of liver function, neutropenia, alopecia, rash, fever, gastrointestinal adverse effects have been reported for albendazole and mebendazole. As it is teratogenic, it should not be used in pregnant woman. The WHO guidelines 37 recommend that patients with operable disease should undergo surgical excision of the cyst followed by a medical therapy for a minimum of 2 years. Long-term therapy should be provided for inoperable cases. If surgery is refused by the patient, then medical therapy could be an alternative. In fact some authors, like Ben-Musa, 9 report successful medical treatment of cyst 44 with no changes of cyst size.
Surgery is the most common form of treatment, curing up to 90% if the cyst is not in a risky location or if the disease is not too far advanced. It has a peri-mortality of 20%. 45 The operation starts with a median sternotomy or right side thoracotomy with the use of CBP, moderate hypothermia, and cross-clamping of the aorta. Pulmonary artery should be clamped to prevent PE. Before removing each lesion, the cyst is aspirated for macroscopic and microscopic examination. When the liquid is a clear colorless liquid and reveals at least one protoscolex, then the lesion is sterile. An inactive lesion can only be aspirated with suction. 46 After aspiration, cystectomy is performed. Surgical removal usually includes sterilization of the cyst before enucleation by injection or instillation of 2% formalin, 0.5% silver nitrate solution, 30% hypertonic saline solution, 1% iodine solution, or 5% cetimide solution. This precautionary measure is performed to prevent dissemination of the infection in case of rupture of the cyst. During surgery, anaphylactic reactions and infection can occur. Location of the cyst is very important for the decision of the operative technique as most cysts in the ventricular myocardium can be resected off-pump and isolated septal cyst is best resected under CPB. 47 Some authors 48 have reported the removal of a HC of the IVS via the IVS with no entry of cardiac chambers in an adult. 48 Therefore, they recommend the excision of the germinative membrane without capitonnage to avoid impairment of the AV conduction pathway or of myocardial contraction. Serologic and echocardiographic controls are recommended for 5 years after extirpation to detect recurrences after surgical manipulation or cysts that were not yet discovered at operation. 49
Conclusions
The cysts are formed in a period of time from 1 to 5 years, and usually present in individuals over 20 years of age. HCs are very rare in children; however, hydatidosis must always be kept in mind in endemic zones. The groups more at risk are usually underserved by medical services. 44 However, the increasing use of mass screenings with ultrasonography in endemic countries is generating important epidemiological data. Cyst echinococcus can have large social impact in endemic area. Research is being conducted to evaluate the burden of disease, including non-monetary costs. Routine echocardiographic screening may be useful in endemic regions when infestation is likely. HC of the heart should be diagnosed in the early and uncomplicated stages when possible 47 and should be removed surgically even in asymptomatic patients. The treatment of choice is surgical excision under CPB. The size of the cardiac cyst in our patient is the biggest yet reported.
Author Contributions
Conceived and designed the experiments: DSK, DG. Wrote the first draft of the manuscript: LF, FB. Contributed to the writing of the manuscript: FB. Agree with manuscript results and conclusions: AR. Jointly developed the structure and arguments for the paper: GP. Made critical revisions and approved final version: AR. All authors reviewed and approved of the final manuscript.