
Abstract
We present a case of a 22-year-old female who presented with acute abdomen and amenorrhea. Emergency laprotomy was done with a clinical diagnosis of ectopic pregnancy. On laprotomy, twisted fimbrial cysts were found. Thus, although fimbrial cysts are rarely twisted, they should be considered as a cause of acute abdomen in a female of reproductive age group.
Introduction
Torsion of uterine adnexa is an important cause of acute abdominal pain reported in the literature. 1 However, isolated torsion of fimbrial cysts has rarely been described as a cause for acute abdomen.2–3 We report a rare case of isolated torsion of fimbrial cysts leading to acute abdomen.
Case Report
A 22-yr-old female presented to the hospital with acute abdomen, amenorrhea for a half month and a half, and spotting on and off. The patient provided written consent to reproduce information or photographs. On physical examination, the patient's vital signs were found to be normal. However, tenderness was found all over the lower abdomen. Laboratory investigations including hemoglobin, total leucocyte count, differential leucocyte count, and routine and microscopic examination of the urine were found to be normal. A urine pregnancy test was weakly positive. Therefore, a serum beta human chorionic gonadotropin (hCG) test was done to confirm pregnancy. However, serum beta hCG levels were within normal range. Therefore, to arrive at a provisional diagnosis, ultrasound examination was requested. The ultrasound report showed a tubo-ovarian mass in the right adnexa along with fluid in the pouch of Douglas, suggestive of fimbrial cysts or ectopic pregnancy (Fig. 1).
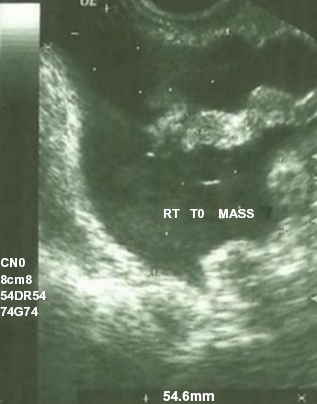
Ultrasound Film showing right tubo-ovarian mass suggestive of ectopic pregnancy.
To arrive at a definitive diagnosis, emergency laprotomy was planned. On laprotomy, multiple cystic structures attached to the fimbriae were seen, which were twisted at their pedicle. Many of them had ruptured leading to collection of about 200 mL of straw colored fluid. However, the fallopian tubes and ovaries were normal on both the sides, so a cystectomy was done. The fluid collected from laprotomy was normal on cytology and microbiology. Cystic structures were sent for histopathologic examination.
On gross examination, multiple cystic structures varying in size from 3 × 3 cm to 2 × 2 cm were seen. The cystic structures were filled with yellow colored fluid and were twisted at the pedicle (Fig. 2).

Gross appearance of fimbrial cysts.
Histopathology showed ciliated, columnar cells with underlying stroma and few chronic inflammatory cells, and a diagnosis of fimbrial cysts was made (Fig. 3).

Histopathology of fimbrial cyst (hematoxylin and eosin × 100).
Discussion
Paraovarian cysts represent approximately 10% of adnexal masses. 4 They are more common in childbearing women. 5 Paratubal cysts arise from Müllerian or Wolffian structures and are common in adult females. These are hormone sensitive and are generally asymptomatic. 6 Malignant neoplasms arising from paratubal cysts are very rare. 7 Rarely, they can be associated with torsion of fallopian tubes. 7 Other complications include hemorrhage, rupture, and infection. 3
Paratubal cysts are difficult to diagnose preoperatively, and even transvaginal ultrasound in older women has detected only about 44% of paratubal cysts preoperatively. 8 In only 1 of 15 patients is the diagnosis of fimbrial cyst suspected before surgery. 4 Thus, acute abodomen is a rare presentation of fimbrial cysts, which needs to be considered in a female of reproductive age group. Timely diagnosis and excision of these cysts may prevent the rare complications of torsion and rupture that are associated with them.
Author Contributions
Conceived and designed the experiments: MR, RN, SKB, SA, FA, AK, SD. Analyzed the data: MR, RN, SKB, SA, FA, AK, SD. Wrote the first draft of the manuscript: MR. Contributed to the writing of the manuscript: MR, RN, SKB, SA, FA, AK, SD. Agree with manuscript results and conclusions: MR, RN, SKB, SA, FA, AK, SD. Jointly developed the structure and arguments for the paper: MR, RN, SKB, SA, FA, AK, SD. Made critical revisions and approved final version: MR, RN, SKB, SA, FA, AK, SD. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.