
Abstract
This is a rare case report of acute pancreatitis secondary to a massive incarcerated paraoesophageal hernia. The pathogenesis resulted from obstruction of the distal pancreatic duct after displacement of the pancreatic head and body into the thorax as part of a Type IV paraoesophageal hernia. Although this condition is rare, the patient made steady progress following laparotomy and open repair of hernia. She made a good recovery after prompt therapy, therefore, this report can be a guide to the diagnosis and treatment of similar conditions.
Introduction
The anatomic spectrum of diaphragmatic hernias is highly variable extending from sliding hiatus hernia, which is the commonest and predominantly asymptomatic type, to paraoesophageal hernia in which the stomach with other organs, such as the colon, spleen, and small bowel herniate into the chest. The tendency is for paraoesophageal herniae to enlarge with time. Because of this, elective surgical repair is recommended for patients who are symptomatic, as surgery becomes more difficult with increasing size of the hernia and age of the patient. In addition, emergency repair of paraoesophageal hernia is associated with a high mortality rate. 1
The two most frequent causes of pancreatitis are gallstones and alcohol, which combined account for over 80% of cases. Once gallstones or alcohol misuse have been excluded, the search for other aetiological factors begins (see Table 1). 2 Any condition that obstructs the pancreatic ducts can result in acute pancreatitis.
Aetiologies of pancreatititis. 2

A systematic search of the literature identified four other reported instances of acute pancreatitis secondary to incarcerated paraoesophageal hernia.3–6
Background
A 61-year-old female presented as an emergency with severe pain associated with vomiting and dyspnoea. The symptoms were progressive in the six weeks prior to presentation with the patient being otherwise fit and well. The only past medical history included a hiatus hernia seen on oesophagogastroduodenoscopy (OGD) a number of years ago. There were no gallstones seen on previous ultrasound scan nor was there a history of alcohol consumption. The only regular medication that the patient was taking was omeprazole 40 mg, the dose of which she had recently increased from once to twice daily. There was no family history of pancreatitis nor was there any history of recent systemic upset apart from the above.
On examination she was tender in the epigastrium and had reduced air entry on the left. Blood tests revealed a hyperamylasemia of 408 Somogyi units, a leukocytosis of 15,000 white blood cells/µL, and hypoxia with a pO2 of 8.63 kPa on room air. Serum calcium and lipid levels were within normal range. Chest radiograph showed considerable eventration of left hemidiaphragm with shift of heart and mediastinum to right (Fig. 1). This patient had nasogastric tube decompression of the stomach and supportive management for a putative diagnosis of acute pancreatitis. Subsequent computed tomogram (CT) scan of chest and abdomen confirmed a paraoesophageal hernia (diaphragmatic neck 6.5 cm) with stomach, large bowel, and small bowel with mesenteric vessels within the left hemithorax. There was no bowel obstruction. The neck and body of pancreas were positioned above the diaphragmatic defect and were not inflamed. There was inflammation and prominent ductal dilatation in the proximal body and tail of pancreas, which lay below the diaphragmatic defect. The tail of the pancreas was oedematous with surrounding inflammatory stranding. There was decreased enhancement of pancreatic tail, however, no definite necrosis was seen (Fig. 2). Complimentary magnetic resonance cholangiopancreatography (MRCP) revealed a pancreatic pseudocyst as well as confirming pancreatitis of tail with dilated duct. The driving pathological mechanism being obstruction of the distal pancreatic duct secondary to the mechanical displacement of the pancreatic head and body to the thorax as part of the Type IV paraoesophageal hernia. No structural abnormalities of the pancreas, such as, pancreas divisum were seen, nor was there any other obstructing ductal lesion. On resolution of her acute pancreatitis the patient was seen at the hepatobiliary clinic with a view to both repair of the hernia and potential distal pancreatectomy.

Chest radiograph.
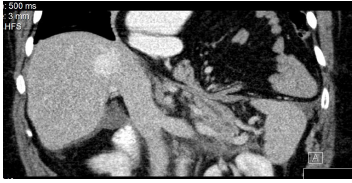
Computed tomography chest and abdomen.
At laparotomy the contents of the hernia were mobilized following division of the left diaphragmatic crus. Stomach, colon, spleen, pancreas, and small bowel were reduced and on inspection the pancreas appeared essentially normal, confirmed by intra-operative ultrasound. The diaphragmatic defect was repaired with a Teflon reinforced suture technique with a posterior wrap fundoplication. The patient made steady progress post-operatively and the recovery continued and she was eventually discharged after two weeks.
Discussion
From a practical perspective diaphragmatic hernias are described as sliding or paraoesophageal. However, traditionally hiatal hernias are classified into four types by the position of the gastro-oesophageal junction relative to the diaphragm. Type I hernia is a sliding hernia. This is the most common and least morbid type. The gastro-oesophageal junction (GOJ) ascends above the impression made by the diaphragmatic crura, the oesophagus and stomach ascending together with the GOJ. Types II–IV described as paraoesphageal hernias are rare. In Type II there is a separate orifice containing protruded fundus of stomach adjacent to a normally located GOJ. Type III is a combination of types I and II hernias with cranially displaced GOJ and stomach through the hiatus. 1 Type IV is characterized by displacement of the stomach with other organs into the chest and was the type encountered in this case. The most frequent herniated organs are the colon, small intestine, omentum, or spleen. This situation can strongly compromise the function and viability of these organs. Complications such as volvulus, occlusion, ischaemia, or even perforation can occur.7–8 Standard preoperative investigations include CT scan chest/abdomen, upper gastrointestinal contrast study, and upper gastrointestinal endoscopy.9,10 Previously published cases of pancreatic herniation through the diaphragm3–7 include four cases associated with pancreatitis,3–6 two of which were in cases of congenital diaphragmatic herniae.4,6 The causal elements of acute pancreatitis in such a herniation have been postulated as repetitive trauma associated with pancreatic movement across the hernia, ischemic compromise of the vascular pedicle, or intermittent folding of the main pancreatic duct.4–6 It is easy to envisage the sharp folding of the pancreatic body depicted in our patient with acute pancreatitis, resulting from folding and occlusion of the main pancreatic duct. Herniation of the pancreas through the diaphragm without complicating pancreatitis is described.7,11,12 The case presented here offers an evaluation of the inflamed pancreas with magnetic resonance imaging, including MRCP. Computed tomography and magnetic resonance imaging both offer evaluation of the pancreatic parenchyma and adjacent soft tissues; however, magnetic resonance imaging allows multiplanar imaging, and MRCP offers a unique non-invasive opportunity to investigate the pancreatic and biliary ducts in these rare patients. The use of manometry in the evaluation of paraoesophageal hernia is controversial. Similarly, ambulatory pH testing does not alter the planned operation.9,10
The approaches available for repair of paraoesophageal hernia include transthoracic, transabdominal, and laparoscopic. The components to a successful repair include complete tension free reduction of hernia contents into the subdiaphragmatic position, excision of hernia sac, closure of hiatal defect, and an antireflux procedure. 10 Roof top incision gives excellent access for repair of large hiatus hernia with associated pancreatitis where pancreatectomy is also being considered.
Owing to the progressive nature of paraoesophageal herniae early repair is recommended in symptomatic patients. Symptoms of obstruction or worsening reflux in someone with a history of hiatus hernia should raise the possibility of paraoesophageal hernia.
Author Contributions
Wrote the first draft of the manuscript: KMB. Contributed to the writing of the manuscript: WC, MT. Made critical revisions and approved final version: KMB. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.