
Abstract
Objectives
Timing to video-assisted thoracoscopic surgery (VATS) in hemothorax is based on preventing acute and long-term complications of retained blood products in the pleural space, including pleural space infection. We propose that the persistence of blood in the pleural space induces a proinflammatory state, independent of active infection.
Methods
We identified six patients with a hemothorax by clinical history, radiographic imaging, and pleural fluid analysis from a database of 1133 patients undergoing thoracentesis from 2002 to 2010 at the Medical University of South Carolina.
Results
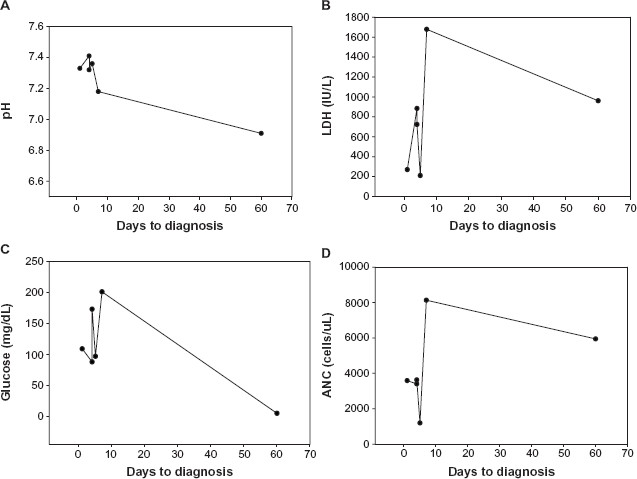
In four of the six patients identified, the time from injury to thoracentesis was one, four, four, and five days, respectively. The fluid pH range was 7.32–7.41. The lactate dehydrogenase (LDH) range was 210–884 IU/L (mean 547 IU/L), and the absolute neutrophil count (ANC) range was 1196–3631 cells/μL. In two patients, the time from injury to thoracentesis was 7 and 60 days. In these two patients, the pH was 7.18 and 6.91, LDH was 1679 and 961 IU/L, and the ANC was 8134 and 5943 cells/μL. Microbiology and pathology were negative in all patients.
Conclusions
The persistence of blood outside the vascular compartment, and within the pleural space, biochemically mirrors infection. We will explore the multiple mechanisms that account for development of pleural fluid acidosis, inflammation, and neutrophil recruitment.
Background
Hemothorax has traditionally been defined as pleural fluid to serum hematocrit ratio ≥50%; however, current consensus guidelines include hematocrits ranging from 25 to 50%, accounting for secondary dilution. 1 An acute hemothorax is commonly the result of blunt or penetrating trauma causing vascular injury. 2 Alternatively, spontaneous hemothorax can occur in the absence of trauma and is most commonly attributed to malignancy, anticoagulation, vascular rupture or malformation, and inherited coagulopathies. 1 Regardless of the cause, the consensus for hemothorax treatment when clinically suspected or proven mandates immediate and complete drainage to avoid late complications of infection and fibrothorax.
Based on expert opinion in the thoracic surgery literature, all patients with hemothorax should be evaluated for drainage using tube thoracostomy. 3 If there is incomplete drainage, reassessment and progression to video-assisted thoracoscopic surgery (VATS) should be considered. 3 The justification is based on the development of pleural fluid acidosis and pleural fibrosis, leading to a potentially unexpandable lung. 3 In addition, several studies suggest that delayed or incomplete drainage increases the risk of empyema, although in a majority of patients, the microbiology was ultimately negative.4–7 While tube thoracostomy and incomplete drainage appear to increase the risk of infection and empyema, the development of pleural fluid acidosis and inflammation may result in a complicated pleural space, which appears to be infected based on the biochemical parameters only. In a single study, 28 patients with blunt trauma were evaluated and treated for empyema with tube thoracostomy based on a functional definition of empyema: (1) an infected pleural effusion, (2) a pleural peel, (3) systemic signs of sepsis (fever or leukocytosis), and (4) no other obvious cause. However, of the 28 patients, only one-third had positive cultures at surgery. 6 In a review of a small case series from the Medical University of South Carolina (Table 1), we have been able to demonstrate the development of pleural fluid acidosis and inflammation consistent with infection, in the absence of a proven pathogen. We describe these findings in what we term a remote hemothorax, as the composition of the pleural fluid changes dramatically as the interval from injury to pleural fluid evaluation increases. We believe that the presence of pooled blood induces a proinflammatory state, resulting in a progressive recruitment of polymorphonuclear leukocytes. Several plausible mechanisms may account for these findings.
Pleural fluid analysis of the reported six cases of hemothorax.

Material and Methods
We identified six patients with a hemothorax by clinical history, radiographic imaging, and pleural fluid analysis from a database of 1133 patients undergoing thoracentesis from 2002 to 2010 at the Medical University of South Carolina. This case series was approved by the hospital's Institutional Review Board as a retrospective chart review.
In all patients, the inciting event was clearly identified, and the interval from the event to thoracentesis was recorded. Pleural fluid for each patient was sent for pH, total nucleated cell count and differential, total protein, lactate dehydrogenase (LDH), glucose, pleural fluid hematocrit, microbiology, and cytopathology. Concurrent serum protein, LDH, and hematocrit were also obtained (Table 1).
Case presentation
Patient 1 was a 38-year-old male admitted to the hospital with an upper gastrointestinal bleed and newly diagnosed hepatic cirrhosis with esophageal varices. Following a complicated hospital course, he was found to have deep vein thrombosis and was started on anticoagulation. After six days of intravenous (IV) heparin therapy without an event, the patient had a fall in his hospital room. Within 24 hours, he developed respiratory distress, and the chest radiograph (Fig. 2A) revealed a new unilateral pleural effusion. Anticoag-ulation was stopped, an inferior vena cava filter was placed, and the patient had tube thoracostomy to drain the hemothorax.
Patient 2 was a 77-year-old female admitted following a syncopal event at home. Upon initial evaluation, she was found to have a rib fracture as well as a non-ST elevation myocardial infarction. She was started on the acute coronary syndrome protocol, including high-dose clopidogrel and IV heparin infusion. Over the next four days, she developed a large, unilateral pleural effusion (Fig. 2B). Diagnostic thoracentesis revealed a hemothorax.
Patient 3 was a 36-year-old male transferred from an outside facility following a motorcycle accident. On admission, he had bilateral chest tubes placed for bilateral hemothoracies. His chest tubes were subsequently removed, and no effusion was noted on follow-up imaging. The patient subsequently noted shortness of breath, and radiographic imaging (Fig. 2C) showed an evolving left-sided pleural effusion. After four days, a CT-guided chest tube was placed by interventional radiology. Pleural fluid analysis revealed a hemothorax.
Patient 4 was an 84-year-old female who initially presented to the hospital in cardiac arrest. She received advanced cardiac life support, including cardiopulmonary resuscitation. After return of spontaneous circulation, she was admitted for further management. Initial chest radiograph (Fig. 2D) revealed rib fracture and small pneumothorax. A subsequent chest radiograph showed resolution of the pneumothorax with small, bilateral pleural effusions (Fig. 2D). The right-sided pleural effusion continued to increase, and on day 5, the patient underwent diagnostic thoracentesis revealing a hemothorax.
Patient 5 was a 49-year-old male with history of hepatitis C who was status post orthotopic liver transplant four years prior. He presented for an outpatient transjugular liver biopsy and was subsequently admitted, when he developed hypotension associated with an acute decline in hemoglobin. Pre-procedure chest radiograph was unremarkable. The admission chest radiograph (Fig. 2E) revealed unilateral pleural effusion. Following correction of his coagulopathy, the unilateral effusion persisted. The pleural fluid was consistent with a hemothorax and was drained by tube thoracostomy seven days following admission.
Patient 6 was a 56-year-old male with a history of chronic hemoptysis. Six years prior, he underwent a lung wedge resection, but his pathology did not reveal the cause of hemoptysis. Two months prior to presentation at our hospital, the patient was admitted to another facility with hemoptysis and was found to have a large amount of unilateral pleural effusion. The fluid was described as bloody, and the patient was treated with outpatient antibiotics. He was subsequently admitted to our institution with a large amount of unilateral pleural effusion noted on CT scan (Figs. 2F and 2G) and decrease in hemoglobin. He was taken to the operating room for tube thoracotomy and underwent a partial pleurectomy and decortication. Pleural fluid analysis performed in the operating room revealed a hemothorax. Figures 1A–D summarizes the pleural fluid pH, LDH, glucose, and ANC for each case from the time of diagnosis
Pleural fluid (
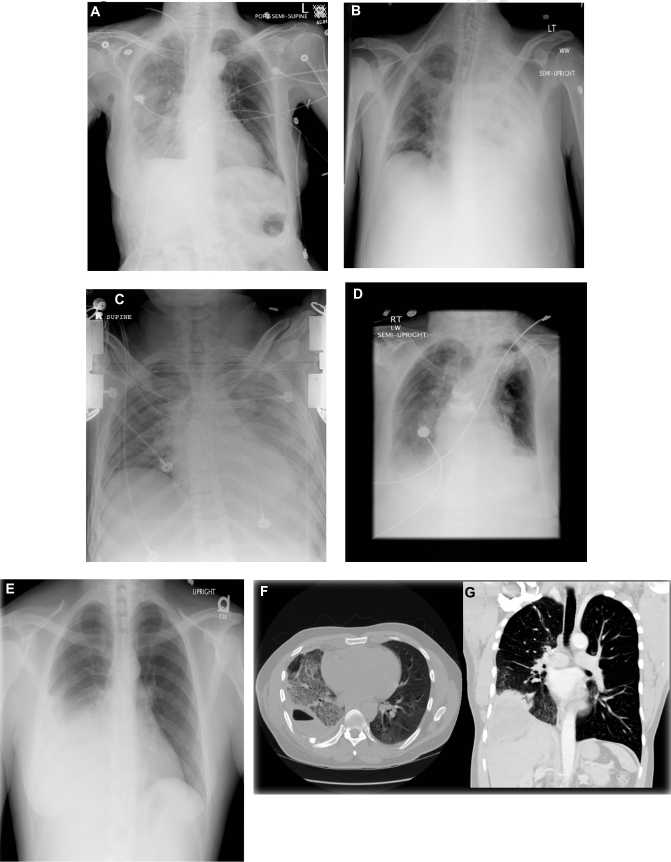
AP chest radiograph showing (
Discussion
Regardless of the cause, a hemothorax is an active, ongoing process within the pleural space that leads to a proinflammatory state, resulting in the formation of an abnormal pleural membrane. The persistence of inflammation and continued neutrophil recruitment results in increased glycolysis, inducing pleural fluid acidosis. 8 The eventual development of a fibrinous pleural membrane ultimately creates a complicated space, further impairing carbon dioxide and lactate clearance and glucose transport into the pleural space. 9 The mesothelial monolayer of the pleura is primarily responsible for both its integrity and its innate response to trauma, inflammation, or infection. 10 Injury of the pleural membrane causes the mesothelial cells to be reactive to the insult and launch a protective response that includes cytokine upregulation, changes in the permeability of the monolayer, and recruitment of inflammatory cells, such as neutrophils, mononuclear cells, and lymphocytes. 10 Once the normal homeostasis of the pleural membrane is disturbed, mesothelial cells release a vast array of chemokines, growth factors, and free radicals (Fig. 3). The result is the formation of a fibrinous pleural peel overlying the visceral and parietal pleural surfaces. With time and defective pleural space healing, the fibrinous pleural membrane matures into a fibroelastic membrane, leading to the development of a trapped lung, or fusion of both the parietal and visceral surfaces occurs, resulting in a fibrothorax (Fig. 3). 10
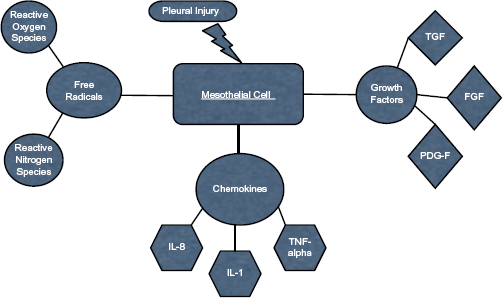
Proposed mechanisms of how remote hemothorax may lead to the developmed of pleural space injury and sterile empyema.
The role of IL-8 released by the mesothelial cells is similar to all other innate responses to inflammation and/or infection. IL-8 induces recruitment and influx of leukocytes from the circulation. The Duffy antigen receptor for chemokines (DARC) belongs to a family of chemokine receptors that have been proposed to mediate inflammation. DARC exists primarily on reticulocytes, mature erythrocytes, and to a lesser extent, venular endothelial cells. 11 It binds both CC and CXC inflammatory chemokines, and thus, acts as a scavenger. Multiple studies have suggested its role in leukocyte trafficking. 11 Because this receptor is not a G-coupled receptor, and therefore, has no signal transducing activity, it is believed to act simply as a sink, for excess free chemokines, preventing inappropriate activation of circulating leukocytes. 12 The DARC has been implicated in acute rejection of lung transplant, the pathophysiology of acute lung injury, and the adult respiratory distress syndrome. 13 Since the DARC receptor is primarily found on erythrocytes, we suspect that DARC expression is down-regulated simply by red blood cell lysis or the DARC receptor expression may be down-regulated by being in a pooled state once removed from the intravascular space. If this is true, the persistence of blood in the pleural space will lead to an inability to scavenge IL-8, and thus, an inability to downregulate the inflammatory response. In the absence of infection, the combination of these two ongoing processes leads to the formation of a thick, restrictive fibrous peel, and impaired chemokine scavenging creates the biochemical appearance of a sterile empyema, or as we have described, a mimicker of infection in patients with a retained hemothorax greater than seven days.
An interesting finding in our series was that the glucose trend did not initially follow the pH value. Traditionally, in diseases where the pathophysiology leads to pleural fluid acidosis, the glucose is typically low. In the setting of pleural space infection, there is increased glycolysis by bacteria and leukocyte phagocytosis. 14 In both rheumatoid pleurisy and malignancy, the development of an abnormally thickened pleural membrane leads to impaired glucose transport into the pleural space. With a hemothorax, the explanation appears to be multifactorial. The initial transport of glucose into the pleural space appears to be normal in a hemothorax but becomes progressively impaired as the degree of inflammation escalates. Maturation of the fibrous pleural membrane impairs CO2 and lactate clearance, resulting in pleural fluid acidosis. Eventually, sometime after seven days, glucose utilization appears to increase exponentially, with unopposed recruitment of inflammatory cells. This scenario leads to an elevated absolute neutrophil count (ANC) and progressive inflammation, causing a cyclical process that may eventually lead to the development of a fibrothorax.
Conclusions
As evidenced by out data, and the mechanisms detailed above, pleural fluid analysis of long-standing hemothorax may simulate pleural infection. For this reason, any clinical suspicion of bleeding into the pleural space should prompt immediate tube thoracostomy and thoracic surgery evaluation.
Compete drainage and/or VATS are measures to gain control of the inflammatory response and prevent evolution to a fibrothorax or a trapped lung. If this occurs, the morbidity from a hemothorax increases dramatically and decortication is often necessary. We recognize that the small sample size and retrospective nature of our study limit out ability to make broad clinical conclusions; however, understanding the natural progression and development of pleural space inflammation because of a remote hemothorax is an important observation and has provided, although speculative, compelling reasons to support a new concept that a remote hemothorax is a mimicker of pleural space infection.
Author Contributions
Conceived and designed the experiments: JTH, PD, SS. Analyzed data: MD, JTH. Wrote the first draft: MD. Contributed to the writing of the manuscript: LBA, CEK, MD, JTH, PD. Jointly developed the structure and arguments for the paper: MD, LBA, CEK, JEN, SS, PD, JTH. Made critical revisions and approved the final manuscript: JTH, LBA. All authors reviewed and approved the final manuscript.