
Abstract
We report the case of a middle-aged man admitted for five months of unexplained left lower quadrant pain. He had been hospitalized on two prior occasions and treated with broad spectrum antibiotics. His clinical presentation was suggestive peritoneal irritation with severe, focal pain on abdominal palpation. Computed tomography scans showed non-specific inflammation in the left lower abdomen with adjacent small bowel wall thickening. Upper endoscopy and colonoscopy were unremarkable on prior admission. Given the severity and focality of the patient's recurrent abdominal pain he underwent laparoscopy and was found to have a wooden toothpick perforation of the small bowel thirty centimeters from the ileocecal valve requiring partial small bowel resection. The patient did well post-operatively. On retrospective questioning he may have eaten a cabbage roll or bacon wrapped shrimp pierced with a toothpick weeks before the onset of symptoms. Toothpick perforation should be a consideration in edentulous persons with focal, severe abdominal pain and trans-abdominal ultrasound or MRI may be a better choice for detecting wooden foreign objects.
Introduction
The differential diagnosis of relapsing abdominal pain is broad with the correct diagnosis being dependent upon a careful history, physical examination, the results of diagnostic evaluations such as radiological and endoscopic assessments, and the clinical course. We present a case of relapsing abdominal pain for 3 months with radiographic evidence of small bowel and mesenteric inflammation. The diagnoses considered included diverticulitis, peptic ulcer disease, inflammatory bowel disease, mesenteric ischemia, intra-abdominal vasculitis, and mesenteric panniculitis. Toothpick perforation of the intestines was suspected and surgical exploration revealed a toothpick perforation of the ileum.
Case
A man in his 50s presented to hospital with a two week history of anorexia, malaise, and constant, sharp left-sided lower abdominal pain. Past history included two drug eluting coronary artery stents 8 months previously for which he received daily aspirin (81 mg) and clopidogrel (75 mg). Prior to the onset of abdominal pain, he was clinically well. The physical examination and vital signs were normal except for having complete upper dentures and the presence of focal tenderness in the mid and left lower quadrants without rebound or guarding. Routine blood tests were normal except for a white blood cell (WBC) count of 12,500/cmm with 82% neutrophils, hemoglobin of 11.2 g/dL with an MCV of 88, and a serum albumin of 3.4 g/dL. Contrast computed tomography (CT) of the abdomen and pelvis showed a small area of fat stranding in anterior midline of lower abdomen and adjacent small bowel wall thickening (Fig. 1). No colonic diverticula were seen. He received empiric oral antibiotic therapy with ciprofloxacin 500 mg every 12 hours and metronidazole 500 mg every 6 hours for 14 days. After one week his pain and symptoms completely resolved.

CT of abdomen and pelvis with contrast demonstrating a small area of fat stranding in anterior midline of lower abdomen and adjacent small bowel wall thickening.
Five weeks after symptoms initially started, he presented with recurrence of the lower abdominal pain, nausea, vomiting, and non-bloody diarrhea. He was afebrile. Physical examination was normal except for marked tenderness in the left lower abdomen lateral to the umbilicus with moderate rebound tenderness. The WBC was 7,400/cmm with 69% neutrophils, platelets 491,000/cmm, hemoglobin 9.7 g/dL and a serum albumin of 2.9 g/dL. Urinalysis was normal. Repeat abdominal CT showed a 5.5 cm extraluminal fluid collection in the mid abdomen adjacent to a loop of ileum with a radiopaque linear structure thought to be oral contrast crossing into the left pelvis with surrounding inflammatory changes (Fig. 2). He was admitted to hospital where upper gastrointestinal endoscopy showed a small linear ulcer in the duodenum. Colonoscopy including endoscopic assessment of the terminal ileal mucosa was normal (Fig. 3).

Repeat CT of the abdomen 5 weeks after initial presentation showing a radiopaque linear structure crossing to the left pelvis with surrounding inflammatory changes (yellow circle).

Images of terminal ileum during colonoscopic evaluation.
He was discharged after 3 days of intravenous piperacillin/tazobactam 3.375 g every 6 hours with improvement of the pain but was readmitted 3 days later with recurrence of the abdominal pain. Repeat CT showing improvement of the extraluminal fluid collections (Fig. 4). Antibiotics were continued and he was discharged after 2 days. On follow-up he continued to experience left sided abdominal pain. Laboratory examination 58 days after onset of the illness revealed a white count of 7,200/cmm, hemoglobin 9.6 g/dL, platelets 390,000 K/cmm and albumin of 3.4 g/dL. CT enterography showed fat stranding in the previously affected loop of small bowel but no discrete extraluminal abscess or fluid collection. He was also scheduled for outpatient video capsule endoscopy but because of recurrent nausea, left lower quadrant pain, subjective fever, and non-bloody diarrhea was readmitted to hospital. His vitals signs were normal. He had normal bowel sounds but was markedly tender to palpation in his left lower quadrant with voluntary guarding. Rectal examination was normal. His white count was 8,200/cmm, hemoglobin 9 g/dL, serum albumin of 3.1 g/dL, sedimentation rate of 58 mm and Saccaromyces IgG was elevated at 34.7 units (normal < 25 units).

Repeat CT of the abdomen and pelvis one and a half months after initial presentation with improvement in extraluminal inflammation.
Diagnostic laparoscopy revealed a segment of small intestine approximately 30 cm from the ileocecal value adherent to the sigmoid colon. A foreign body was palpated in the lumen of the small bowel and a wooden blue toothpick was seen protruding from the ileum. Fifteen cm of ileum was resected encompassing the area of toothpick perforation (Fig. 5). The patient made an uneventful postoperative recovery and was discharged after 9 days.
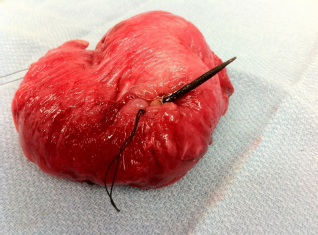
Resected small bowel with perforating blue toothpick (stitch marks the area of perforation).
On further discussion he recalled eating cabbage rolls and bacon wrapped shrimp pierced with toothpicks in the weeks preceding his initial presentation.
Discussion
The onset of acute abdominal pain in adults associated with evidence of intraperitoneal inflammation has a broad differential. In this case the acute onset, the presence of dentures, and radiological evidence of a contained perforation suggested the possibility of a toothpick perforation. Toothpicks have long history; anthropologists have reported striated grooves on fossilized teeth of ancient humans and La Quina Neanderthals that were caused by abrasive toothpicks. 1 Toothpick use in the United States blossomed in the late 1800's when Charles Foster imported manufactured toothpicks from South America and heavily promoted their use. 2 Toothpick use, while both ancient and widespread, is not without its medical complications. For example, the U.S. Consumer Product Safety Commission National Injury Information Clearinghouse from 1979 to 1982 estimated the incidence of all toothpick related injuries to be 3.6 per 100,000 persons. 3 Children age 5 to 14 have the highest rate of injuries. Overall toothpicks are implicated in 9% of foreign body ingestions. 4 In a systematic review of the literature from 1966 to 2000, 57 published cases of ingested toothpicks were found. 5 The average age was 52 and 88% were male. Interestingly, only 12% remembered swallowing a toothpick. Risk factors for toothpick ingestion include alcohol intoxication, dulled palatal sensation most commonly due to the presence of dentures, rapid ingestion of food, habitual chewing of toothpicks, and mental retardation.3,6,7 The most common sites of injury are the duodenum and sigmoid colon 5 although toothpicks have been reported to migrate and cause injury to the retroperitoneum causing upper urinary tract obstruction, 8 pericardium causing injury to the right coronary artery, 9 and cardiac tamponade. 10 Unusual presentations include liver abscess,11,12 subcutaneous emphysema of leg, 13 and arterial-enteric fistula. 14
In our case the toothpick was originally not recognized. While CT scan can identify wooden objects (e.g., it has been used to detect imperfections and determine authenticity of high quality stringed instruments such as those made by Stradivari), 15 given their small diameter, wooden toothpicks can easily be missed if a high index of suspicion is not present. On retrospective review, a small radiopaque density was detectable near the area of mesenteric and small bowel inflammation and could be retrospectively identified in each of the CT scans received during his 3 month course. Trans-abdominal ultrasound may be a better choice for detecting wooden foreign objects (sensitivity 52% to 82%)16,17 suggesting that it should be considered whenever foreign body ingestion is considered. In experimental studies, saline soaked wooden splinters of varying sizes placed within porcine muscle were easily detected via MRI, suggesting that MRI or possibly 64 slice CT may be useful.15,18 The definitive diagnosis of toothpick perforation has been made at laparotomy in about 50% of published cases, by endoscopy in 19%, by imaging studies in 14%, and at autopsy in 12%. 5
The nature of our patient's abdominal pain was likely caused by the wooden toothpick extending into the peritoneal cavity causing focal peritonitis. The relapsing course may have been a result of intermittent antibiotic administration. Surgical consultation was obtained early in the patient's clinical course; however rapid improvement with antibiotics led to a conservative approach. Toothpick perforation may mimic fistulizing Crohn's disease and serious consideration was given to initiating a course of biologic therapy such as infliximab. This approach has been previously described in a case of overlooked toothpick perforation and, as expected, was not successful. 19
Most ingested objects readily pass through the gastrointestinal tract and foreign body ingestion is not commonly considered on the differential diagnosis of acute onset abdominal pain. 20 Sharp objects such as toothpicks with two pointed ends, straightened paperclips, and animal bones are particularly likely to cause foreign body-associated gastrointestinal perforations. Most perforations are easily diagnosed if the objects are radiopaque or because peritoneal irritation prompts exploratory abdominal surgery. In our patient, the combination of dentures and acute onset of abdominal pain with evidence of periintestinal inflammation led to toothpick perforation being considered and the suspicion was subsequently confirmed at laparoscopy. Possibly, if abdominal ultrasound or MRI had been performed as part of the diagnostic evaluation, the correct diagnosis and therapy would have been instituted sooner.
Author Contributions
Wrote the first draft of the manuscript: RJS, SS. Contributed to the writing of the manuscript: RJS, SS, DYG. Agree with manuscript results and conclusions: RJS, SS, DYG. Jointly developed the structure and arguments for the paper: RJS, SS, DYG. Made critical revisions and approved final version: RJS, SS, DYG. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.