
Abstract
We report a patient with primary anti-phospholipid syndrome (APS) who developed pulmonary edema following sudden-onset pain in the left, lower back of the chest. Radiological examinations demonstrated fresh infarction of the left adrenal gland but no obvious thrombi in pulmonary arteries. The patient quickly recovered from pulmonary edema with anti-coagulation therapy alone. Primary APS may have caused adrenal infarction in the patient, leading to transient pulmonary edema via microthrombosis and/or excessive release of catecholamine.
Keywords
Introduction
Anti-phospholipid antibodies, including the anti-cardiolipin (CL)-dependent β2-glycoprotein (GP) I antibody, are well known as a frequent cause of thrombosis in both arteries and veins.1,2 The precise mechanisms of this thrombosis remain unclear, but several recent reports have demonstrated that interference with the coagulation-anticoagulation pathway and endothelial cell function plays a central role in the pathogenesis.3,4 In addition to the presence of the anti-phospholipid antibodies, a history of thrombosis, such as cerebral infarction and repeated fetal death, and a lack of clinical symptoms and laboratory data suggestive of other collagen vascular diseases, particularly systemic lupus erythematosus, lead to the diagnosis of primary anti-phospholipid syndrome (APS). 1
Here, we report a young female patient with primary APS who showed transient pulmonary edema following sudden-onset pain in the left, lower back of the chest. Computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated fresh infarction of the left adrenal gland, and we postulate that this pathology may have contributed to the development of pulmonary edema in the patient. In this report we review the literature, and focus upon the pathogenesis of pulmonary edema in APS.
Case Report
The present patient was a 20-year-old woman. At age 17 she suffered from brain infarction due to occlusion of the left middle cerebral artery. She was admitted to a neighboring hospital by ambulance, and was diagnosed as having primary APS. Mild hemiparesis in the right extremities remained as a neurological sequel after immediate treatment, but she could do everything necessary for daily living by herself without help. Her general status was good under oral administration of clopidogrel and warfarin, which was controlled to keep the prothrombin time- international normalized ratio (PT-INR) at approximately 2.0. At age 20 she suddenly developed severe spontaneous pain in the left lower back of the chest with no precipitating cause. The symptom persisted over the following 2 days, and she visited the emergency outpatient clinic, where chest CT demonstrated abnormal density lesions in the left lung. Laboratory data showed no abnormal findings in either hematology or blood chemistry except for a slightly increased level of PT-INR (1.86). Non-steroidal anti-inflammatory drugs could not fully relieve her clinical symptoms. She was referred to our hospital 5 days after onset of the back pain, and was admitted for treatment.
On admission, body temperature, radial pulse, and blood pressure were 36.8 °C, 92/min and 93/62 mmHg respectively. Percutaneous oxygen saturation was 97% under room air. No abnormal findings were detectable in either the chest or abdomen, but she complained of pain on the left lower back of the chest, particularly at the inspiration phase. Mild muscle weakness with hyperreflexia and positive pathological reflexes was seen in the right side, although there were no other neurological abnormalities. No abnormal findings were detected on routine laboratory data, including hematology and electrolytes, except for a slight increase in C-reactive protein (0.89 mg/dL, normal < 0.1 mg/dL) and elongation of activated partial thromboplastin time (57.7 sec, normal 23–38 sec). Rheumatoid factor, anti-nuclear antibody, anti-double-stranded DNA antibody and anti-neutrophil cytoplasmic antibody were all negative, but anti-CL β2-GPI antibody (125 U/mL, normal < 3.5 U/mL) and lupus anticoagulant (2.49, normal < 1.3) were positive. Chest X-ray revealed no cardiomegaly, and echocardiography showed no abnormal findings. Chest CT demonstrated multiple irregular-shaped ground-glass opacities in the left lung (Fig. 1A) without obvious thrombi in main pulmonary arteries, which were compatible with pulmonary edema rather than infarction according to a radiology review. Blood gas analysis showed no hypoxia (partial pressure of oxygen in arterial blood 81.1 Torr, normal 80–100 Torr) or hypercapnia (partial pressure of carbon dioxide in arterial blood 35.0 Torr, normal 35–45 Torr) under room air. To further investigate the cause of her back pain, we performed abdominal CT and MRI, which showed swelling of the left adrenal gland (Fig. 2A) suggestive of fresh infarction (Fig. 2B) with no obvious hemorrhage (Fig. 2C). The right adrenal gland was normal. Adreno-pituitary hormones in plasma taken in the early morning, such as catecholamine (epinephrine < 0.01 ng/mL, normal < 0.17 ng/mL; norepinephrine 0.05 ng/mL, normal 0.15–0.57 ng/mL; dopamine < 0.02 ng/mL, normal < 0.03 ng/mL), cortisol (9.8 ng/dL, normal 1.0–15.0 ng/dL) and the adrenocorticotropic hormone (29.1 pg/mL, normal 7.2–63.3 pg/mL), were normal.

Computed tomography demonstrated multiple irregular-shaped ground-glass opacities in the left lung (
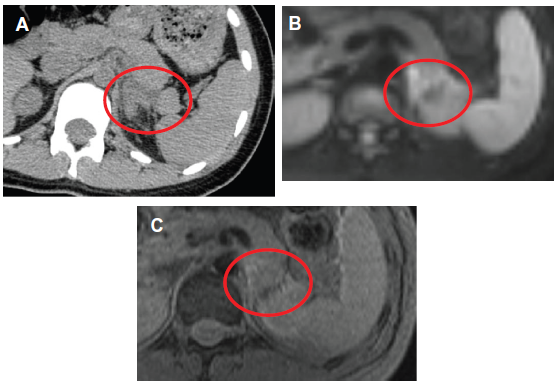
Abdominal computed tomography demonstrated marked swelling of the left adrenal gland (
Continuous intravenous infusion of dalteparin was started at 2000 U/day immediately after cessation of clopidogrel and warfarin. One day after admission the ground-glass opacities on chest CT had extended to the bilateral lungs (Fig. 1B). Nevertheless, her left back pain gradually ameliorated, and she did not complain of any respiratory symptoms, such as dyspnea and cough. On the following day chest CT revealed obvious improvement of the ground-glass opacities (Fig. 1C) and her back pain had almost disappeared. Thereafter, she showed no recurrence of back pain. Both clopidogrel and warfarin were restarted after cessation of dalteparin 7 days after admission, and she was discharged from our hospital 1 week later. Neurological sequelae due to the previous cerebral infarction did not worsen throughout the clinical course. She has since remained in good general health for 9 months, with PT-INR at 2.5 to 3.0.
Discussion
The present patient suddenly developed severe pain in the left lower back of the chest persisting for approximately 7 days, which was ascribable to adrenal infarction as shown by CT and MRI. Laboratory data on admission revealed well-preserved adrenal function. As an adrenal gland usually has a rich arterial blood supply, but only 1 central drainage vein, occlusion of the latter can easily cause infarction, frequently with hemorrhage. 5 Considering that the present patient had a previous episode of cerebral artery thrombosis in her teens, primary APS probably underlay the adrenal infarction also despite the anti-coagulation therapy. To prevent an increase in the size of infarction as well as recurrence, we used an intravenous anti-coagulant, dalteparin, in the acute phase, and thereafter restarted clopidogrel and warfarin.
The most notable point about the present case is the transient appearance of ground-glass opacities in the bilateral lungs. They were clinically diagnosed as pulmonary edema based on the predominant involvement of the lung parenchyma with an acute progressive course and a lack of evidence indicating infection. As the peak of lung opacities postdated that of the back pain, pulmonary edema was considered to occur as a complication secondary to adrenal infarction. The present patient did not fulfill the criteria of acute respiratory distress syndrome (ARDS) throughout the clinical course. 6 The precise cause of her pulmonary edema is unclear, but there are 2 possible factors worth consideration. One is micro-vascular thrombosis in the lungs. Chest CT in the present patient demonstrated no thrombi in the main pulmonary arteries, but those in small vessels may have been undetectable. A catastrophic type of APS is widely known to cause microvascular thrombosis in multiple organs and quickly produce functional failure.7,8 In the present patient primary APS may have caused thrombosis not only in the adrenal gland but also in small vessels of the lungs, leading to pulmonary edema via increases in hydrostatic pressure and endothelial cell injuries.
The other possible factor is excessive release of catecholamine from the adrenal gland damaged by infarction, although no obvious episode of sudden-onset hypertension was identifiable. Cardiomyopathy leading to pulmonary edema can occur in an excess of serum catecholamine, such as norepinephrine and epinephrine, as seen in pheochromocytoma, 9 but the present patient showed no abnormal findings in either electro- or echocardiography suggestive of myocardial damage. High blood concentrations of catecholamine have been reported to sometimes cause pulmonary edema even without cardiac involvement via direct damage to alveoli and capillaries with constriction of postcapillary venules.10–12 In the present patient excessive release of catecholamine from the adrenal gland damaged by infarction may have increased permeabilization of lung small vessels, resulting in pulmonary edema. The quick improvement of pulmonary edema in parallel with the disappearance of the back pain due to adrenal infarction also supports this hypothesis. The lack of increases in blood concentrations of catecholamine on admission may be due to the fact that 5 days had already passed since onset of the adrenal infarction.
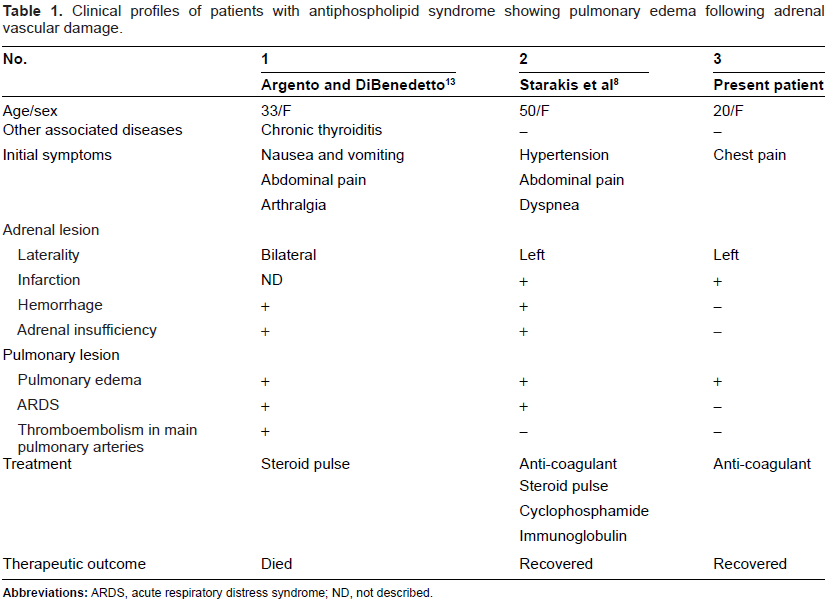
No reports have so far described asymptomatic pulmonary edema following adrenal infarction as seen in the present patient. Nevertheless, there are 2 case reports from other institutes that describe ARDS complicating adrenal infarction or hemorrhage in APS.8,13 Clinical profiles of the reported cases and the present patient are summarized in Table 1. All of the patients are young to middle-aged women. The present patient showed left back pain alone with no respiratory symptoms, while in the reported cases pulmonary edema quickly worsened and reached ARDS with adrenal insufficiency. Both reported patients received intensive treatment, such as steroid pulse therapy and immunosuppressants, in order to relieve their clinical symptoms, but case 1 died of heart failure. Adrenal hemorrhage was seen in both reported patients, and of these 1 (case 1) showed bilateral involvement. These findings suggest that the prognosis of pulmonary edema following adrenal vascular damage, including infarction, may depend on the size and/or severity of the latter.
Clinical profiles of patients with antiphospholipid syndrome showing pulmonary edema following adrenal vascular damage.
In conclusion, adrenal infarction is a rare manifestation of APS, but is important with regard to possible association of life-threatening pulmonary edema. When APS patients complain of sudden-onset back pain in the lower chest, adrenal infarction should be considered as a possible complication.
Author Contributions
KO wrote the first draft. KT, DK, KF and MM took part in analysis and interpretation of data, and MM and SI revised the manuscript for intellectual content. All authors reviewed and approved the final version.
Funding
This work was supported in part by the Health and Labor Sciences Research Grant on Intractable Diseases (Neuroimmunological Diseases) from the Ministry of Health, Labor and Welfare of Japan.
Competing Interests
Authors disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.