
Abstract
Disease severity in asthma can be classified as mild, moderate or severe based upon the frequency of symptoms or the severity of airflow obstruction. This review will focus on the treatment of youths greater than 12 years of age and adults with moderate persistent asthma. Moderate asthmatics may have daily symptoms that cause some limitation with normal daily activities and require use of a rescue inhaled short-acting beta2-agonist inhaler or experience nocturnal awakenings secondary to asthma that occur more than once per week. Furthermore, spirometry may reveal airflow obstruction with a reduction in FEV1 to between 60% and 80% of predicted. Although inhaled corticosteroids (ICS) are the primary controller medication used to modify symptoms in moderate asthmatics, additional controller medications, such as inhaled long-acting beta2-agonists (LABA), leukotriene receptor antagonists (LTRA) or theophylline, are often needed to obtain optimal disease control. While the addition of an inhaled LABA to an ICS is very effective at improving disease control in moderate asthma, concerns have arisen over the safety of LABAs, in particular the risk of asthma-related death. Therefore, consideration may be given to initially adding a LTRA, rather than a LABA, to ICS when asthma symptoms are not adequately controlled by ICS alone. Furthermore, individualization of medication regimens, treatment of co-morbid conditions, and patient education are crucial to optimizing compliance with therapy, improving disease control, and reducing the risk of exacerbations. Lastly, the development of new asthma treatments, perhaps based upon personalized medicine, may revolutionize the future treatment of moderate asthma.
Keywords
Asthma is a chronic inflammatory disease of the airway that is highly prevalent in both children and adults. The World Health Organization estimates that approximately 245 million individuals suffer from asthma worldwide, while the Centers for Disease Control reported that asthma prevalence in the United States was 8.2% in 2009, which represents approximately 24.6 million individuals.1,2 The Expert Panel 3 Report (EPR-3) from the National Asthma Education and Prevention Program (NAEPP) of the National Heart, Lung, and Blood Institute (NHLBI) defines asthma as the presence of “variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation,” which are commonly triggered by exposure to allergens, irritants or cold air, as well as by viral infections or exercise. 3 The clinical manifestations of asthma are typified by intermittent symptoms of cough, wheeze, chest tightness or dyspnea, that often occur in individuals with a personal or family history of allergy and/or other common diseases, such as gastroesophageal reflux or chronic rhinosinusitis. Asthma symptoms and physiologic evidence of airflow obstruction are caused by underlying airway inflammation (cellular infiltration by activated T helper lymphocytes, eosinophils, neutrophils and mast cells with associated edema), airway remodeling (increased airway secretions, airway epithelial cell and smooth muscle hyperplasia, epithelial cell desquamation, goblet cell hyperplasia and collagen deposition), and smooth muscle constriction. 4
Characterization of a patient's asthma severity is a critical guide for the initiation of asthma treatment and the determination of future risk of deterioration. Disease severity can be classified as mild, moderate or severe based upon the frequency of asthma symptoms or the severity of airflow obstruction (Fig. 1).
3
While the majority of asthmatics have mild disease, those with moderate or severe asthma have more frequent symptoms that are difficult to control.5,6 This review will focus on the treatment of youths greater than 12 years of age and adult patients with moderate persistent asthma. Moderate asthmatics have daily symptoms or nocturnal awakenings secondary to asthma that occur more than once per week, but not nightly. On spirometry, moderate asthmatics have an FEV1 between 60% and 80% of predicted, and their FEV1/FVC ratios are generally reduced by 5% or less when compared with predicted values. In addition, they may require daily use of an inhaled short-acting beta2-agonist (SABA) for control of their asthma symptoms and also experience some limitation with normal daily activities.
NHLBI National Asthma and Education and Prevention Program Expert Panel 3 Report classification of asthma severity in youths ≥ 12 years of age and adults.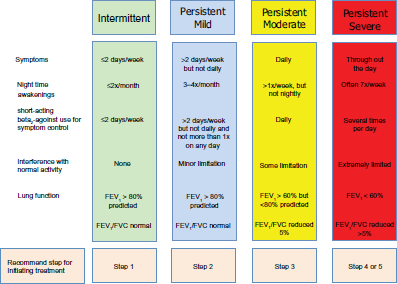
The EPR-3 recommends a step care approach that matches the intensity of treatment to disease severity and adequacy of control of asthma symptoms. As shown in Figures 1 and 2, the EPR-3 proposes that moderate asthmatics initiate treatment at Step 3 or 4.
3
The objective of treatment is to decrease disease severity and improve control while providing optimally dosed medications with the fewest possible side effects. Furthermore, treatment is directed at decreasing the risk of future exacerbations, as well as reducing the loss of lung function over time. The specific benchmarks for improvement of symptoms are defined as a decrease in the use of short-acting beta
2
-agonists (SABA), a reduction in daytime and nocturnal asthma symptoms, an improvement in ability to conduct normal activities, and personal satisfaction with the level of asthma control (Fig. 3). By periodically monitoring disease severity through patient visits and spirometry, the health care provider can determine the level of control and risk of future exacerbations within each patient and adjust therapy accordingly.
Stepwise approach for managing asthma in youths ≥ 12 years of age and adults as recommended by the NHLBI National Asthma and Education and Prevention Program Expert Panel 3 Report. Assessing asthma control and adjustment of therapy in youths ≥ 12 years of age and adults as recommended by the NHLBI National Asthma and Education and Prevention Program Expert Panel 3 Report.

Controller Medications for Moderate Persistent Asthma
The mainstay of therapy for moderate asthma is the chronic administration of controller medications that modify disease severity by reducing airway inflammation and bronchoconstriction in patients with persistent disease. The EPR-3 recommends that inhaled corticosteroids (ICS) be utilized as the main controller medication to which adjunctive controller medications can be added. These include inhaled long-acting beta2-agonists (LABAs), leukotriene modifiers, or theophylline. 3 The addition of allergen immunotherapy can also be considered for patients who have allergic asthma. In addition, patients are provided with short-acting beta-agonists (SABA) to be used as needed to provide bronchodilation for symptomatic relief.
Inhaled Corticosteroids
The mainstay of treatment for moderate persistent asthma among youths over the age of twelve and adults are inhaled corticosteroids (ICS). 3 Corticosteroids, via interactions with glucocorticoid receptors, are highly effective for the treatment of asthma based upon their broad anti-inflammatory effects, which are mediated via the suppressed transcription of pro-inflammatory genes, termed trans-repression, as well as the activation of many anti-inflammatory genes, termed trans-activation. 7 The clinical benefits of ICS therapy in asthma include improvements in disease severity, asthma control, quality of life, pulmonary function, airway hyperresponsiveness, disease exacerbations, hospitalizations and death. 3 Furthermore, ICS reduce the number of airway inflammatory cells (eosinophils, mast cells and T cells), as well as mucus production and hypersecretion, airway edema, and vascularization.4,8 Therefore, all patients with moderate asthma should receive treatment with ICS.
Suggested dosing of inhaled corticosteroids for asthma therapy in adults and adolescents (≥ 12 years).

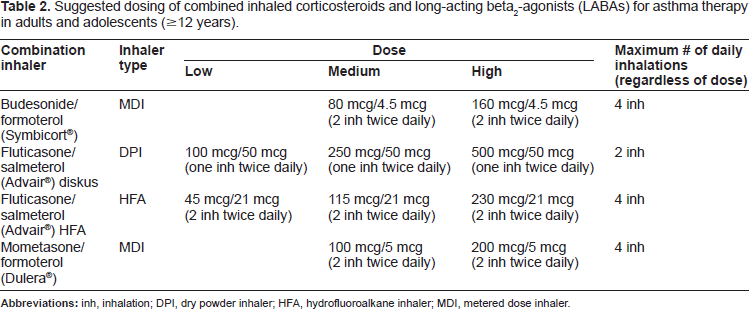
Suggested dosing of combined inhaled corticosteroids and long-acting beta2-agonists (LABAs) for asthma therapy in adults and adolescents (≥ 12 years).
Long-Acting Beta2-Agonists
β2-agonists induce bronchodilation via interacting with β2 adrenergic receptors to increase cAMP with resultant airway smooth muscle relaxation. 3 β2-agonist medications can be classified by their duration of action. The effects of short-acting β2-agonists (SABAs), such as albuterol, persist for 4 to 6 hours, whereas the effects of long-acting β2-agonists (LABAs), such as salmeterol and formoterol, last for 10 to 12 hours. 14 Therefore, SABAs are recommended as a quick relief medication for asthma symptoms, whereas LABAs are considered a controller medication that attenuate bronchoconstriction, but do not modify underlying airway inflammation. Consistent with this concept, the addition of an inhaled LABA to an ICS has been shown to improve lung function, decrease symptoms and reduce exacerbations in asthmatics who are not well controlled on low or medium doses of ICS. 3 The EPR-3 recommends that patients with moderate persistent asthma may be treated with a combination of low-dose (Step 3) or medium dose (Step 4) ICS plus a LABA. Combination inhalers facilitate delivery of the maximal recommended daily dose of LABA with varying doses of ICS (Table 2). The pharmacodynamics of inhaled salmeterol and formoterol differ. Inhaled salmeterol has an onset of action of between 30 and 48 minutes with a peak effect at 3 hours. 15 It has a half-life of 5.5 hours and undergoes hepatic metabolism by CYP3A4. In contrast, inhaled formoterol has a rapid onset of action within 3 minutes of administration, with 80% of its peak effect evident within 15 minutes. 16 The half-life of formoterol in powder form is approximately 10 to 14 hours, while nebulized formoterol has a half-life of approximately 7 hours. It undergoes hepatic metabolism via direct glucuronidation and O-demethylation by multiple cytochrome P450 enzymes. Arformoterol and indacaterol are new LABAs that have been approved by the US. Food and Drug Administration (FDA) for use in COPD, but not for the treatment of asthma.
Although the addition of an inhaled LABA to an ICS is very effective at improving disease control, concerns have arisen over the safety of LABAs. Prior to its approval by the FDA, the Serevent® Nationwide Surveillance Study noted an increase in risk of asthma-related death in patients treated with salmeterol as compared with albuterol. 17 Based upon this study, as well as reports to the FDA of serious asthma exacerbations and deaths in patients treated with salmeterol, the manufacturer conducted the Salmeterol Multicenter Asthma Research Trial (SMART), which showed a small but significant increase in asthma-related deaths (1 in 700 patient-years) in individuals receiving salmeterol without concurrent ICS over 28 weeks.18,19 The safety concern of increased risk of asthma-related deaths associated with the use of LABAs prompted the FDA to conduct a comprehensive review of the benefits and risks of LABAs for the treatment of asthma, which resulted in a black box warning that contraindicates LABA monotherapy for the treatment of asthma. 17 The FDA also recommended against LABA use in patients whose asthma is well-controlled with low-dose or medium-dose ICS alone. In addition, adjunctive LABA therapy use should be discontinued, if possible, once asthma control is achieved and maintained by an asthma controller medication, such as ICS. If LABA therapy is utilized, it should be provided as a combination inhaler with ICS, never as a separate LABA inhaler, in order to minimize the potential of overuse. More recently, in April of 2011, the FDA updated their recommendation stating that five prospective clinical trials will be conducted among all age groups to determine whether LABAs, when used concurrently with ICS, are safe for the treatment of asthma. 20 These studies are expected to conclude in 2017 and hopefully will provide definitive data regarding the safety of LABAs. In the interim, it has been suggested that LABA use be restricted to patients in whom other adjunctive controller medications, such as leukotriene modifiers, do not provide adequate asthma control. 19
Leukotriene Modifiers
Leukotriene modifiers are another class of adjunctive controller medication that can be combined with ICS for the management of moderate persistent asthma. Cysteinyl leukotrienes (leukotriene C4, D4 and E4) are pro-inflammatory lipid mediators that are released by mast cells, eosinophils and basophils to induce airway smooth muscle contraction, tissue edema, eosinophil migration and increased airway secretions.3,4,21 The pathway that generates cysteinyl leukotrienes requires the conversion of the precursor fatty acid, arachidonic acid, to leukotriene A4 by 5-lipoxygenase (5-LO), which is then converted to leukotriene C4 or leukotriene B4. 21 Leukotriene C4 can then be metabolized further to generate leukotriene D4 and leukotriene E4, which play important roles in allergen-mediated airway inflammation. Leukotriene modifiers either antagonize the ability of cysteinyl leukotrienes to interact with the cysteinyl leukotriene receptor, CystLT1, or inhibit the enzymatic activity of 5-LO.

Zileuton is the only 5-lipoxygenase inhibitor currently approved for treatment of asthma in the United States. It is orally administered and requires dosing either 4 times daily for the regular formulation or twice daily for the controlled release formulation. 22 Zileuton undergoes gastrointestinal and hepatic metabolism via CYP1A2, 2C9, and 3A4. 29 The safety profile of zileuton is similar to LTRAs with the exception of transaminitis, which occurs in 4.4% of cases, but is typically not associated with jaundice or liver failure. 30 Therefore, liver function tests should be monitored monthly during the first three months of treatment and every 2 to 3 months during the first year, as well as periodically in subsequent years.22,30 Other side effects that have been associated with zileuton include headache, gastrointestinal symptoms, myalgias, leukopenias, sleep disorders and behavior changes. 22
The EPR-3 recommends the addition of a LTRA to low-dose ICS as Step 3 therapy or medium-dose ICS as Step 4 therapy (Fig. 2). Results of randomized clinical trials have suggested that LABAs are superior to LTRAs as add-on therapy based upon their ability to decrease symptoms and exacerbations when asthma symptoms are not adequately controlled with ICS alone.22,31,32 Recently, a community-based, multicenter trial compared the addition of a LTRA or LABA when patients were inadequately controlled by ICS. 32 This “real world” study followed patients for 2 years and showed that LTRAs were equivalent to LABAs as add-on therapy for a diverse group of primary care patients who were not adequately controlled with ICS alone, using the miniAQLQ as the primary outcome measure. Furthermore, treatment with a LTRA was equivalent to an ICS as first-line controller medication. When these results are considered in the context of the uncertainty regarding the safety of LABAs for the treatment of asthma, clinicians may favor the addition of a LTRA, rather than a LABA, as initial step-up therapy when patients are persistently symptomatic on ICS alone. 33 The ease of daily oral administration of LTRAs (montelukast), as well as their favorable safety profile and effectiveness for treatment of allergic rhinitis are additional reasons for clinicians to consider initial step-up therapy with LTRA in patients who are persistently symptomatic despite ICS. Furthermore, patients with aspirin-sensitive asthma, exercise-induced asthma and those with asthma exacerbations secondary to viral upper respiratory tract infections may be more likely to benefit from leukotriene modifier therapies. 22
Theophylline
The xanthine derivative, theophylline, is an orally administered, non-selective phosphodiesterase inhibitor that mediates airway smooth muscle relaxation by increasing cAMP levels, and may also possess mild anti-inflammatory activities.3,34 EPR-3 recommends sustained release theophylline as an alternative, but not preferred, controller medication that can be added when asthma symptoms are not adequately controlled by ICS. 3 Consistent with this recommendation, addition of theophylline to low-dose ICS has been shown to be as effective as increasing the dose of ICS for improving control of asthma symptoms.35,36 However, comparison of step-up therapy with theophylline to LABAs has shown that LABAs (ie, salmeterol) are superior in improving morning and evening peak expiratory flow rates, as well as in reducing the use of rescue medication, while no differences were noted in improving FEV1.36,37 Step-up therapy with the addition of theophylline, however, is associated with a higher incidence of central nervous system and gastrointestinal side effects. Few studies have directly compared step-up therapy with theophylline to LTRAs.36,38,39
Examples of common medications that can modify serum theophylline levels. 40

Allergen Immunotherapy
The EPR-3 recommends that subcutaneous allergen immunotherapy (AIT) also be considered for patients who have persistent asthma if there exists a clear relationship between asthma symptoms and exposure to the offending allergen. 3 AIT is typically utilized when patients have symptoms during at least a major portion of the year and are persistently symptomatic despite use of multiple controller medications. There is evidence that immunotherapy needs to be administered for prolonged periods, typically three to five years, to be effective.3,42,43 A recent update of a Cochrane review of 88 trials of injection allergen immunotherapy for asthma concluded that AIT reduces asthma symptoms and the use of asthma medications, as well as improves allergen-specific bronchial hyperreactivity, but does not have a consistent effect on lung function. 43 Systemic reactions to AIT were frequent, occurring in one out of nine patients. Since subcutaneous AIT can be associated with severe and sometimes fatal allergic reactions, especially severe bronchoconstriction, therapy should only be administered in a health care provider's office. 3 Similarly, a Cochrane style meta-analysis of 25 trials of sublingual immunotherapy for asthma concluded that there was a significant reduction in asthma severity, but not asthma symptoms, which suggests that the magnitude of the effect is not very large. 44 No severe reactions were noted in these studies, which represents an advantage of sublingual over subcutaneous immunotherapy. Potential mechanisms that mediate the effectiveness of AIT include induction of tolerance by allergen-specific regulatory T cells with resultant increases in allergen-specific IgG4 and decreases in Th2 cells, IgE and eosinophilia.45,46 Sublingual AIT may also decrease allergic responses via stimulating oral Langerhans cells. 46 New forms of immunotherapy are currently under development which may advance further the role of AIT for the treatment of allergic disease. 45
Putting it All Together: Management of Moderate Asthma
The EPR-3 recommends that patients with moderate persistent asthma initiate therapy at Step 3, which includes an ICS alone or in combination with an adjunctive controller medication. 3 This recommendation is based upon the potent anti-inflammatory properties of ICS that attenuate the airway inflammation that underlies the pathogenesis of asthma. Thus, therapy for moderate persistent asthma may be initiated with either a medium dose ICS or a low-dose ICS in combination with either a LABA, LTRA or theophylline. Although combination therapy with an ICS plus a LABA had frequently been utilized as the medication of choice for this patient population, safety concerns regarding LABAs have supported the concept that LABAs be utilized with caution until definitive data are available regarding their effect on asthma-associated mortality. 19 Therefore, clinicians and patients may opt to initiate therapy with either a medium dose ICS alone or a low-dose ICS in combination with a LTRA instead of an ICS in combination with a LABA. Furthermore, monotherapy with a LABA should never be utilized as a treatment for asthma. The addition of theophylline to a low-dose ICS is a non-preferred option due to the potential for toxicity and the need for monitoring of serum levels. Similarly, 5-LO inhibition with zileuton is a less desirable option due to more limited efficacy data and the need to monitor liver function tests. 3
Patient preference also needs to be considered when devising an asthma treatment plan, as a significant proportion of asthmatics with sub-optimally controlled asthma are non-adherent with prescribed treatments. 47 In particular, non-adherence rates with controller medications range from 30% to 70%, while approximately 20% may not acquire any controller medication at all. 48 Inclusion of patient preferences in the decision making process regarding asthma treatment may improve adherence to treatment. Factors that may improve compliance include use of a combination inhaler as opposed to two single inhalers, as well as the use of oral agents as compared with inhalers, as it is easier to swallow a pill than to properly use an inhaler.32,49 Furthermore, improper inhaler technique is common and is associated with poor disease control and increased risk of hospitalization or emergency department visits, especially in patients who are older, have less education and have not received proper instruction by health care providers.50,51 Compliance may be improved by education about the disease and proper inhaler technique.50,52
Frequency of administration may also impact compliance, as it is easier to adhere to a once daily medication than one that requires repeated dosing. 53 Similarly, compliance may be more difficult with medications that require periodic monitoring, such as zileuton or theophylline. Therefore, asthma management therapies need to be tailored to the preference of individual patients to increase adherence with prescribed treatments.
After therapy has been initiated, patients should be monitored at two to six week intervals to ensure that symptom control has been achieved. 3 Patients are not well-controlled if they have asthma symptoms more frequently than twice a week, utilize a rescue short-acting beta2-agonist inhaler more than twice a week, have nocturnal awakenings more than twice per month, ***FEV1 or a peak flow less than 80% of predicted, or have evidence of poor control on a validated asthma questionnaire (Fig. 3). If asthma symptoms are not well-controlled, then therapy should be “stepped up” by either increasing the ICS dose from low dose to medium-dose or by the addition of a LTRA, LABA or theophylline to medium dose ICS (Fig. 2). Allergen immunotherapy may also be considered as an adjunct therapy in individuals with atopic asthma who are chronically exposed to the offending allergen. Additionally, the patient's inhaler technique should be reviewed, as well as their compliance with therapy. Furthermore, an investigation to determine whether environmental factors, such as allergens, pollutants or irritants, or co-morbid conditions, such as gastrointestinal reflux or rhinosinusitis, are preventing adequate control of asthma symptoms. If these measures fail to improve asthma control, then therapy should be “stepped up” further to Steps 5 or 6 for severe asthma, as needed, which includes the options of anti-IgE therapy (omalizumab) and oral corticosteroids.
Once asthma symptoms are well-controlled for a period of 3 months, then consideration can be given to “stepping down” therapy, which is an equally important goal of asthma therapy in order to minimize side effects that can be associated with the long-term use of asthma controller medications. For example, although ICS have few side effects, systemic absorption occurs and can be associated with a reduction in bone growth in children.8,33 Furthermore, high dose ICS can be associated with an increased risk of cataracts and fractures in high-risk adults. 8 Consistent with this approach, a recent community-based study of supervised step-down therapy confirmed that a significant reduction in ICS dose could be achieved without deterioration of airway inflammation or function. 54 Given the recent safety concerns, consideration may be given to withdrawal of LABAs. However, stepping down to ICS monotherapy may be associated with poorer asthma control as compared to a reduction in dose of ICS with continuation of the LABA.55–57 Consideration might also be given to “stepping down” from other medications with potential side effects, such as theophylline or zileuton.
Conclusions
Moderate asthma is a common, but challenging, disease that is frequently managed by general practitioners, as well as specialists. Patients with moderate asthma can be difficult to manage and typically require more than one controller drug, as well as therapy for co-morbid conditions, such as environmental allergies, gastroesophageal reflux or rhinosinusitis. Involvement of health care providers in the individualization of medication regimens, as well as in patient education, are crucial to optimizing compliance with therapy and disease control. Health care providers also need to be continually aware of emerging data regarding the utilization and safety of controller medications that can significantly impact disease management. Lastly, the development of new asthma treatments, perhaps based upon personalized medicine, has the potential to revolutionize the future therapy of moderate asthma.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.