
Abstract
Context
Syncope is a commonly encountered by primary care physicians and cardiologists. Etiology is frequently not apparent, and patients may undergo unnecessary tests. Treatment must be tailored to the likely etiology. Complexities of diagnosis and treatment often warrant referral to a specialist.
Objective
To highlight the evolving recommendations for managing syncope in a clinically and cost effective manner.
Evidence Acquisition
An electronic literature search was undertaken of the Medline database from January 1996 to April 2006, using the Medical Subject Heading syncope, defibrillators, pacemakers, echocardiogram, cardiomyopathy, long QT syndrome, Arrhythmogenic right ventricular dysplasia, and Brugada syndrome. Abstracts and titles were reviewed to identify English-language trials. Bibliographies from the references as well as scientific statements from the Heart Rhythm Society, American Heart Association, and American College of Cardiology were reviewed.
Evidence Synthesis
A methodical approach to syncope can improve diagnosis, limit testing, and identify patients at risk of fatal outcome. A thorough history, physical exam and electrocardiogram are critical to the initial diagnosis. Presence of heart disease determines the extent of work-up and treatment. A trans-thoracic echocardiogram should be performed in patients with an unclear diagnosis and a positive cardiac history or an abnormal ECG. Ventricular arrhythmias are the most common cause of syncope in patients with structural heart disease. Patients with an ejection fraction less than 30 percent should receive an implantable defibrillator with few exceptions. An electrophysiology study may assist risk stratification in syncopal patients with borderline ventricular function. In patients without structural heart disease, the presence of a well defined arrhythmia syndrome consistent with a genetically determined risk of sudden death must be sought. The 12-lead electrocardiogram, family history and clinical presentation will identify most high-risk patients. Patients without structural heart disease can often be managed conservatively with well defined strategies for preventing neurocardiogenic syncope.
Conclusions
Managing syncope requires a methodical approach. An understanding of the limitations of the diagnostic tools and treatments is important. Lethal causes of syncope make it imperative to recognize the appropriate timing of referring patients to specialists.
Evidence Acquisition
An electronic literature search was undertaken of the Medline database from January 1996 to April 2006, using the Medical Subject Heading syncope, defibrillators, pacemakers, diagnosis, treatment, echocardiogram, cardiomyopathy, long QT syndrome, Arrhythmogenic right ventricular dysplasia, and Brugada syndrome. Abstracts and titles were reviewed to identify English-language trials. Bibliographies from the references as well as scientific statements from professional organizations were reviewed.
Evidence Synthesis
Epidemiology
Syncope is the transient loss of consciousness with loss of postural tone due to cerebral cortical hypoperfusion. It is associated with absence of neurological sequelae and variable or limited recollection of peri-event details. 1 Although sometimes associated with sudden death, the causes of syncope can be difficult to diagnose. 2 Syncope results in 3% of emergency room visits, 1%-6% of hospital admissions and costs $750 million year to diagnose and treat.3,4 The overall incidence rate, a ratio of number of patients with syncope to number of person-years, of a first report of syncope is 6.2 per 1000 person years. 5 It is 2.6%-5.7% in the 20-69 years age group, increasing to 11.1% after 70 years. In octogenarians, it is 16.9% in men and 19.5% in women. Common known causes of syncope are neurocardiogenic (21.2%) and cardiac (9.5%). The cause is unknown in 36.6% of patients (Table 1), 5 necessitating further diagnostic testing and specific treatment. 6
Major Causes of Syncope.

The presence of heart disease as a predictor of a cardiac cause of syncope is 95% sensitive and 45% specific. 7 Absence of heart disease excludes a cardiac cause of syncope in 97% of patients. 7 In cardiac patients, the most specific predictors of a cardiac cause of syncope are syncope in the supine position or during effort, blurred vision and convulsive syncope. Predictors of a neurally mediated cause are time between the first and last syncopal episode >4 years, abdominal discomfort before syncope and nausea or diaphoresis during recovery. In patients without heart disease, palpitation is the only significant indicator of a cardiac cause. 7
This review highlights causes of syncope, as well as diagnostic and management options. It is important to note that the syndromes discussed touch on complexities and diagnostic features to help generalists recognize syndromes that might be present. Most patients with these syndromes or recurrent unexplained syncope should be referred to specialists such as cardiologists, electrophysiologists and neurologists.
Workup for Syncope
A thorough history, physical examination and electrocardiogram (ECG) are the core of the workup with a 50% diagnostic yield.8,9 Questions related to abruptness of onset, peri-syncope symptoms, and exacerbating or attenuating factors are helpful. The patient's history and presentation should guide testing (Fig. 1).

Suggested Algorithm for the Approach to Syncope in Patients.
Common tests in the syncope workup include head upright tilt test (HUT), various types of continuous electrogram monitoring such as 24-hour Holter and external loop recorders, as well as implantable loop recorders (ILR). Electrophysiology testing (EPS) is rarely indicated as initial workup of syncope. However, EPS can sometimes be helpful in specific situations where an arrhythmia related etiology is suspected. Expectant management is appropriate in patients with the first syncope episode, absent cardiac history, normal ECG and physical examination. For patients with recurrent syncope, HUT and an external 30-day loop recorder may be considered. Twenty four hour Holters are rarely useful in diagnosing the cause of syncope due to the limited monitoring window. The primary role of loop recorders and Holter monitors are for symptom-rhythm correlation. Hence, a significant index of suspicion for an arrhythmia must be present.
If cardiac disease is absent and clinical suspicion for vasovagal syncope is high, empiric management with medications and behavioral modifications is reasonable. If the HUT reproduces the clinical presentation, management with medications tailored to the specific mechanism (vasodepressive, cardioinhibitory, or mixed) and behavioral modifications is indicated. If tachyarrhythmia or bradyarrhythmia is diagnosed, or syncope is recurrent, referral to an electrophysiologist is recommended. An unrevealing initial workup but a positive cardiac history or an abnormal ECG (Table 2) should prompt an echocardiogram to identify structural heart disease. In one study, when limited to such patients, arrhythmia wasv subsequently diagnosed in 50% of patients with an EF ≤ 40% and in 19% of patients with a normal EF. However in patients with a negative cardiac history and a normal ECG, no arrhythmias were diagnosed and echocardiogram did not aid diagnosis. 10 In patients with significant valvular heart disease, syncope is often an indication for valve replacement. With few exceptions, patients with an EF <30%-35% require a defibrillator (ICD), regardless of symptoms.11,12 Patients with syncope and borderline LV function with inducible ventricular tachyarrhythmias (VT) on EPS also benefit from an ICD. EPS should be performed if the suspicion for arrhythmia is high based on history and the presence of structural heart disease. Catheter based ablation may play an important adjunctive role in reducing the risk of ICD shocks in patients with recurrent VT.
ECG Clues to Disorders Associated with Syncope.
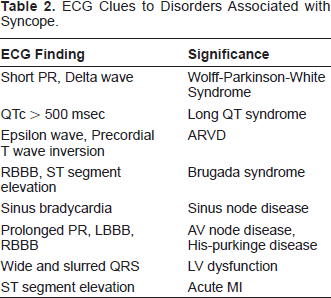
Patients with syncope and structurally normal heart but an abnormal ECG require evaluation to exclude an arrhythmia. If an inherited arrhythmia syndrome is identified, referral to a specialist is necessary since further risk stratification, implantation of a pacemaker or ICD, or possible catheter based ablation may be required. Common scenarios include elderly patients with syncope and bundle branch block, as well as young patients with RBBB and syncope with the Brugada or long QT syndrome. Treatment involves a pacemaker for the former and an ICD for the latter.
Neurocardiogenic syncope
Neurocardiogenic syncope (NCS) is frequently and erroneously used interchangeably with vasovagal syncope when in fact, vasovagal syncope is a subset that falls under the broader neurocardiogenic or neurally mediated reflex syncope. It has an association with carotid sinus hypersensitivity (CSH), as well as micturition, cough and defecation syncope. Many patients with CSH may not have clinical NCS. NCS is a reflex syncope due to exaggerated orthostatic adjustments, resulting in the failure of the autonomic nervous system (ANS) to maintain adequate vascular tone. This causes hypotension, bradycardia, cerebral hypoperfusion, and unconsciousness. 13 Although the exact mechanism remains controversial, one prevailing thought is that peripheral venous pooling causes a precipitous drop in cardiac preload, increased cardiac inotropy and activation of mechanoreceptors (cardiac C fibers) that fire during stretch. 14 The sudden increase in neural traffic to the medulla causes the paradoxic decline in sympathetic activity resulting in hypotension, bradycardia and syncope.13,15
NCS may be associated with prodromal nausea, diaphoresis, lightheadedness, blurred vision, headaches, palpitations, paresthesia and pallor which occur in the upright position and resolve when supine. 13 The patient may complain of fatigue or a “washed-out” feeling after the event. 15 There is a striking similarity between the hemodynamic collapse profile in NCS and CSH. 13 Syncope due to CSH may occur with head turning, shaving, or carotid sinus pressure. 15
HUT may help diagnose NCS since prolonged upright posture can cause venous pooling and provoke an autonomic reflex in predisposed individuals.16,17 The patient is typically tilted upright at an angle of 70°-80° for 20-30 minutes. Isoproterenol may be infused after drug-free HUT, but this may reduce specificity in a dose-related manner.13,18 A cardioinhibitory, vasodepressive, or mixed response may be observed. In a cardioinhibitory response, the heart rate (HR) often abruptly decreases >20 bpm, followed by a precipitous blood pressure (BP) drop. In a vasodepressor response, the BP drops independent of the HR. 18 The test is positive if the clinical symptoms are reproduced, along with an abrupt drop in BP and/or HR. 19 It is important to note that an abnormal HUT alone is not necessarily indicative of or diagnostic of NCS, especially with structural heart disease present. Referral to a specialist is appropriate to rule out potentially lethal causes of syncope.
HUT has a 672%0 -83% sensitivity and a 75%-100% specificity 20 with variable reproducibility. 21 It may be helpful in recurrent unexplained syncope after an appropriate clinical and diagnostic evaluation. However, heart disease and arrhythmias must be excluded before HUT in cardiac patients. 22 HUT may be indicated in “high risk” occupation groups such as airline pilots, commercial vehicle drivers and competitive athletes presenting with a single syncopal episode. It is also useful in evaluating patients with an apparent cause but in whom susceptibility to NCS would affect treatment. Management of NCS involves situation avoidance and patient reassurance of its benign prognosis.15,16,23 Increasing salt and fluid intake, avoiding prolonged standing, using compression stockings, moderate exercise, tilt training, and limb muscle tightening may be helpful. Biofeedback therapy may prevent NCS induced by psychological stimuli. 13
The effectiveness of beta-blockers in preventing NCS in studies are mixed.24,25 The likelihood of recurrent NCS is similar between the metoprolol and placebo groups. 26 Based on the clinical scenario and the response observed at the time of HUT, whether primary vasodepressor, primary cardioinhibitory, or a mixed type picture, the choice of pharmacologic agent can be tailored accordingly. Depending on the specific situation, beta blockers with intrinsic sympathomimetic effects, alpha agonists selective serotonin reuptake inhibitors, fludrocortisone, disopyramide and scopolamine have been used, either as sole therapy or in combination, with some success in small, non-randomized studies. 27 33 While profound bradycardia and even periods of asystole are not uncommonly associated with NCS, the role of pacing remains highly controversial. Two trials showed that patients with tilt-positive cardioinhibitory syncope benefited from pacing.34,35 However, the control groups did not get a device and placebo effect could not be excluded. In a subsequent trial, patients with pacemakers were randomized to the device being “on” or “off”, and pacing therapy did not reduce NCS incidence. Patients with asystolic responses during preimplant HUT had a significant increase in time to syncope recurrence compared with those with bradycardia alone.13,36
Pacemaker (PPM) should not be recommended as first-line therapy for patients with recurrent NCS.37,38 However, in patients who are unresponsive to conservative therapy, lack a prodrome or have demonstrated prolonged pauses, pacing may reduce syncope frequency or increase the time from onset of prodrome to unconsciousness. 13 Patients with recurrent syncope and ventricular pauses exceeding 3 seconds due to carotid sinus stimulation may benefit from a PPM. However, pacing is not warranted in the absence of a hyperactive cardioinhibitory response, or if avoidance behavior is effective. 39
Orthostatic hypotension (OH)
Contrary to neurocardiogenic syncope which is a result of excessive autonomic activity, orthostatic hypotension (OH) is a failure of the autonomic reflex response to compensate for lower extremity venous pooling and presents as a rapid and precipitous drop in blood pressure upon assuming an upright posture.1,13,40 Under normal circumstances, there is a gravity-mediated downward displacement of approximately 300 to 800 mL of blood, representing a volume drop of 25%-30%, to the vasculature of the abdomen and lower extremities. 41 Successful maintenance of upright posture and hemodynamic stability is dependent on a complex interplay of neuro-hormonal changes, baro- and mechano-receptors, and circulatory changes. Orthostatic hypotension is defined as a 20 mmHg drop in the systolic blood pressure (SBP) or 10 mmHg drop after 3 minutes of standing.42,43 It frequently occurs in older patients, and causes 6%-33% of syncope.44,45 Diabetes and pharmacotherapy (Table 3)1,13 may cause autonomic dysfunction manifesting with OH. 46 OH may be an early manifestation of Parkinson's disease and predicts mortality in middle-aged adults. 42 Symptoms of orthostatic weakness, near syncope and syncope may be insidious. Other symptoms include urinary retention and incontinence in women and impotence in men. 13
Drugs that Commonly Cause Syncope.
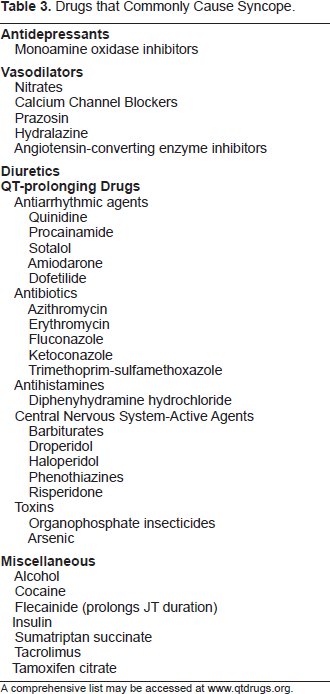
A comprehensive list may be accessed at www.qtdrugs.org.
Treatment of OH depends on the type and extent of autonomic dysfunction. Increasing dietary fluid and salt intake, exercise and compression stocking to improve venous return are often beneficial.47,48 Fludrocortisone is a mineral corticoid that increases peripheral ≈-receptor sensitivity to promote vasoconstriction. Other vasoconstrictive agents such as midodrine and methylphenidate have been used with some success. 50 In a small series, pyridostigmine, an acetylcholinesterase inhibitor, was shown to be effective in preventing orthostatic hypotension without exacerbation of supine hypotension. 49
Postural orthostatic tachycardia syndrome and inappropriate sinus tachycardia
Postural orthostatic tachycardia syndrome (POTS), is characterized by an abrupt increase in heart rate of at least 30 bpm from baseline or heart rate greater than 120 bpm within 10 minutes when moving from supine to upright position without significant orthostatic hypotension. 13 Associated symptoms include extreme fatigue, palpitations, near syncope, and syncope.50,51 The majority (90%) of POTS have no identifiable cause. Diabetes, amyloidosis, heavy metal poisoning, Sjogren's syndrome, lupus, and alcoholism are associated with secondary POTS. Other causes of orthostatic intolerance (e.g. medications) should be excluded.
There is significant overlap of symptoms between POTS and inappropriate sinus tachycardia (IST). IST is an ill-defined clinical syndrome with a heart rate response out of proportion to the physiological stressor. There is general agreement that a resting heart rate exceeding 100 bpm is inappropriate and the surface electrocardiogram P wave morphology is nearly identical to that of the sinus P wave. Secondary causes of sinus tachycardia such as fever, pain, thyroid disorder, anemia, medications and dehydration must be excluded. Although the mechanism of IST is not entirely clear, enhanced automaticity of the sinus node, altered sympathovagal balance, and impaired baroreflex sensitivity are some of the proposed mechanisms. 52 54
Supraventricular arrhythmias
Syncope due to supraventricular tachycardia (SVT) is an unusual presentation in the absence of structural heart disease. Structural abnormalities such as aortic stenosis (AS) and hypertrophic cardio-myopathy (HCM) must be considered and evaluated with an echocardiogram. Syncope typically occurs after SVT initiation or with a prolonged pause after abrupt SVT termination in the setting of sinus node dysfunction (SND). Symptoms are related to the ventricular rate, presence of underlying heart disease, and any concurrent conduction disturbances. 55 Rapid heart rates associated with a wide QRS complex are of concern. Atrial fibrillation (AF) occurring in the presence of an antegradely conducting accessory pathway, wherein ventricular rates may sometimes exceed 300 bpm, is associated with syncope and even a risk of VF and sudden death. 56 Patients characteristically manifest evidence of the Wolff-Parkinson-White (WPW) syndrome with a delta wave on the ECG. These patients should be referred to an electrophysiologist for catheter ablation. 57
Bradyarrhythmias
Aging causes fibrosis of the sinoatrial node and AV conduction. This leads to bradycardia and syncope, possibly necessitating a PPM. Third-degree AV block, and advanced second degree AV block are class I indications for PPM. Patients with bifascicular or trifascicular block in the setting of syncope have a class IIa indication for a PPM. However, an echocardiogram must be obtained to evaluate for LV dysfunction or other structural heart disease as this may necessitate an ICD. 58 PPM is also indicated in patients with bradycardia and syncope in the setting of SND. RV pacing alone should be minimized whenever possible. 59 In elderly patients, SND is often associated with AF and may manifest as tachy-brady syndrome—periods of sinus bradycardia alternating with AF with rapid ventricular response. These patients may also exhibit increased vagal activity or responsiveness that may be independent of age related nodal fibrosis.
Heart disease and syncope
Coronary artery disease (CAD) and syncope
Left ventricular (LV) dysfunction is a predictor of mortality in patients with syncope and CAD. 44 Transient episodes of near-syncope may also be clues in patients with ischemic cardiomyopathy. These patients should be referred to a cardiologist or electrophysiologist.8,60 Active ischemia must be identified with stress imaging and/or cardiac catheterization. The presence of prior infarction can serve as a VT substrate and a significant arrhythmia risk must be assumed if prior infarction has resulted in depressed LV function. Echocardiography is indicated in such patients. The current ICD guidelines recommendation of prophylactic ICDs for patients with significant LV dysfunction has reduced the role of diagnostic EPS for risk stratification. However, in patients with CAD and a borderline LV function, a diagnostic EPS may be helpful. The most common abnormality found at EPS is VT. 61 An ICD is indicated if sustained VT is inducible. 62 In syncopal patients with EF <35%, there is an increased one-year risk of death. 63
Coronary revascularization is indicated when VT/VF and syncope occur in the setting of acute coronary ischemia. Monomorphic VT (MMVT) indicates existence of a fixed anatomic substrate and necessitates treating ischemia and primary therapy directed at VT management. An ICD should be implanted in patients resuscitated from VF/syncope without a reversible cause. 64 Pharmacologic agents such as amiodarone, beta-blockers, and sotalol may be considered for reducing symptoms resulting from recurrent VT causing syncope. 64 Catheter ablation may be effective in eliminating recurrent VT 65 and has an important role as adjunctive therapy in patients with ICDs with multiple shocks due to recurrent ventricular arrhythmias
Nonischemic dilated cardiomyopathy (NIDCM)
Patients with NIDCM and syncope have an increased mortality due to sustained VT/VF. 66 HUT and EP testing have limited diagnostic utility in this patient population.44,67,68 An ICD is indicated in NIDCM with unexplained syncope and in patients with EF < 35%. 68 70 These patients should be referred to an electrophysiologist for further evaluation due to the risk of arrhythmia related sudden cardiac death.
Left ventricular outflow syndromes
Obstruction to the left ventricular outflow tract in hypertrophic cardiomyopathy (HCM) and aortic stenosis (AS) can cause syncope due to reduced cardiac output. HCM prevalence is 0.2%. 44 The 1% annual risk of sudden death results from VT or VF.71,72 Patients with HCM with high risk markers should be referred to an electrophysiologist for consideration of ICD. Risk factors include a family history of premature sudden death, documented sustained VF/VT, unexplained syncope, LV thickness exceeding 3 cm, hypotensive response to exercise and non-sustained spontaneous VT.64,73 Syncope may result from ventricular arrhythmias, dynamic outflow tract obstruction, or vagal mechanisms. Management includes beta blockers, verapamil and amiodarone, but controlled trials are lacking. 74 Prophylactic antiarrhythmic agents to suppress premature ventricular contractions (PVC) are not recommended. Genetic analysis may contribute to risk stratification. 64 Dual chamber pacing, alcohol septal ablation and myotomy-myectomy may be alternatives to medical treatment. 75
Aortic stenosis (AS) may be classified as congenital, rheumatic or calcific. It occurs in 25% of patients with chronic valvular disease. The obstruction of the LVOT results in a systolic gradient across the valve and LV hypertrophy. Patients become symptomatic in the fifth to seventh decades. Dyspnea, angina and syncope are the cardinal symptoms. Syncope results from vasodilatation with a fixed cardiac output. If not treated surgically, the average life expectancy after syncope onset is 3 years. Sudden death occurs in 10%-20% of patients with AS. Surgery or valvuloplasty must be considered in the setting of syncope. 76
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C)
In ARVD/C, the right ventricle (RV) muscle is replaced by fibrous and/or fibrofatty tissue which can be demonstrated by low-voltage areas on three-dimensional electroanatomic voltage maps, and a dilated, hypocontractile RV on echocardiog-raphy or magnetic resonance imaging. 77 Syncope occurs in 10%-20% patients with ARVD/C, typically due to sustained or non-sustained MMVT. 78 An autosomal dominant abnormality with incomplete penetrance, ARVD/C occurs between the second and fifth decades of life with palpitations or syncope associated with VT/VF or with SCD. 79
An isolated deflection at the end of the QRS complex in leads V1 or V2 (epsilon wave), and T wave inversion in leads V1-V3 may be present.80,81 PVCs and most VT originate in the RV and have a LBBB pattern. Patients with ARVC/D should be referred to an electrophysiologist. ICD implantation is recommended in patients with syncope or sudden death.64,82 Substrate-based catheter ablation of VT in ARVD/C has good short-term success in controlling recurrent VT, with reported acute success of 77%-100% in some small series.64,83 The recurrence rate at mean of 30 months post ablation is 11%-36%. 83 85 In a series by Dalal et al. 23 out of 24 patients had recurrent VT at 32 months. 86 However, it is important to note that no epicardial or substrate based ablation was performed in their series.
Syncope without structural heart disease
Right ventricular outflow tract (RVOT) tachycardia
Right ventricular outflow (RVOT) tachycardia is the most common ventricular arrhythmia in patients without structural heart disease. Patients may present with exercise induced palpitations and syncope. However, true syncope is an uncommon presentation (<10%) since these patients can tolerate the VT due to their younger age and structurally normal hearts. These VT typically arise from the septal aspect of the RVOT beneath the pulmonic valve. The ECG shows an inferiorly directed left bundle branch block (LBBB) pattern. 87 These VT tend to be adenosine sensitive and may be treated with beta blockers or calcium channel blockers, although breakthrough may occur. 88 The success of catheter ablation of this tachycardia exceeds 90 percent and should be considered if the VT is drug refractory or in patients reluctant to take lifelong drug therapy. 89
Long-QT syndrome (LQTS)
Multiple genetic abnormalities can cause a long QT interval on the ECG. 90 Patients with LQTS have abnormalities in ventricular repolarization and may develop a polymorphic VT (PMVT)—“torsades de pointes”. Syncope is the most common presenting symptom for this disorder, but seizures and cardiac arrest are also predictors of high risk.91,92 Arrhythmogenic syncope often occurs in association with acute physical, emotional, or auditory arousal. As with many of the previously described causes of syncope, myoclonic jerks can sometimes be observed and may be misinterpreted as a seizure.
The QT interval is measured as the longest QT in any of the standard 12 ECG leads. 1 A corrected QT interval exceeding 500 ms identifies patients with the highest arrhythmia risk. QT-prolonging medications (Table 3) can frequently precipitate life threatening VT/VF and must be avoided in patients suspected of having this syndrome. 1
Since VT/VF can be precipitated by exercise in patients with LQT1 and LQT2, avoiding competitive sports must be considered along with daily administration of beta-blockers. ICD implantation is recommended for patients who have recurrent syncope or are cardiac arrest survivors and have family members with marked QT prolongation. 64 Genetic testing is available for some subtypes of known mutations and may be a useful tool in screening family members. Patients with LQTS should be referred to an electrophysiologist.
Brugada syndrome
Brugada syndrome (BS) is characterized by ST-segment elevation in the right precordial ECG leads, and high incidence of sudden death in patients with structurally normal hearts due to PMVT. Its prevalence is 5/10,000 and is more common in Asian males. 91 It has an autosomal dominant inheritance pattern. An abnormality in the gene SCN5A encoding the ≈ subunit of the cardiac sodium channel gene causes the syndrome.1,90,91,93 The ECG changes may be dynamic and can be potentiated by administering sodium channel blocking drugs such as procainamide or flecainide.
Non-sustained PMVT can manifest as recurrent syncope. Sustained PMVT can cause cardiac arrest or sudden death. Syncope must be considered potentially malignant and not presumed to be vasovagal. One-third of patients with BS with syncope or VF develop a new episode of PMVT in 2 years. 94 ICD implantation is indicated for cardiac arrest survivors and patients with syncope and spontaneous or provocable ST-segment elevation in V1, V2, or V3. Clinical monitoring is considered in asymptomatic patients if the Brugada ECG pattern is elicited only with provocative pharmacological challenge. 64 Patients with ECG findings, syncope or a family history of sudden death should be referred to an electrophysiologist.
Catecholminergic polymorphic ventricular tachycardia (CPVT)
CPVT is an unusual cause of recurrent syncope and typically presents as PMVT during adrenergic surges. The baseline ECG is normal without structural heart disease. 95 Familial history of syncope or sudden death exists in 30% of patients. 95 The gene encoding the ryanodine receptor regulates intracellular calcium flux and is affected in autosomal dominant CPVT.96,97 Evaluation for premature CAD, cardiac catheterization for anomalous coronary arteries, and echocardiogram or MRI for ARVD and other etiologies should be considered in patients with exercise precipitated syncope. Genetic testing may play a role in clinical management. 98 If spontaneous or stress induced ventricular arrhythmias are documented, beta-blockers are indicated. Patients with syncope and/or PMVT during exercise on beta blockers should receive an ICD. 64 These patients must be referred to an electrophysiologist. (See Table 4)
Indications for Referral to a Cardiac Electrophysiologist.

Exercise induced syncope
Exercise induced syncope may herald important clinical risk. NCS can occur during or immediately after exercise. Syncope may also be the initial manifestation of several possibly lethal cardiac conditions including HCM, CPVT, congenital heart disease, anomalous coronary arteries, ARVD/C, myocarditis, LQTS, WPW, dynamic outflow tract obstruction, and valvular disease. Thus, patients with exercise induced syncope warrant a thorough evaluation including an exercise stress test, ECG, echocardiogram and appropriate referrals. 99 Although the great majority of exercise induced syncope is benign in the absence of structural heart disease, appropriate counseling of patients and lifestyle modification may be warranted. Even a “benign episode” of syncope occurring at an inopportune time may have catastrophic outcomes. (e.g. syncope during water sports)
Neurological evaluation for syncope
Syncope is an unusual presentation in neurological processes and should be pursued if the history or physical examination suggests a focal deficit. 100 Common neurological causes of syncope are transient ischemic attacks (TIA) and seizures, which may cause syncope in 9% of patients (Table 1).15,61 Patients with neuromuscular disease such as Duchenne dystrophy may have AV block, VT or VF rather than a primary neurologic basis for their syncope. 101 Neurological syncope is associated with an increased risk of all-cause mortality and fatal or nonfatal stroke. This increased risk is likely due to stroke in patients with neurological syncope who had preexisting cerebrovascular disease. 5
Common neurological tests in evaluating syncope include brain CT scans, electroencephalogram (EEG) and carotid Doppler.8,102 These have a low diagnostic yield in unselected patients. In one study, abnormal head CT or EEG was diagnostic in 4% of patients. In general, an EEG should be performed within 24 hours of the seizure to maximize diagnostic yield. 103 Doppler studies performed in 185 patients were abnormal in 19 patients but had no diagnostic yield.104,105 However, neurology consultations were obtained in only 18% patients undergoing such studies, suggesting that most tests were requested by non-neurologists. 106 It is likely that a neurologist who would be more likely to uncover pertinent historical facts and focal neurologic abnormalities from a given patient would reduce such unnecessary tests. 107 109
Unknown cause of syncope
Thirty seven percent of syncope is due to unknown causes. 5 The diagnostic yields of long-term loop electrocardiography and HUT are 30% and 60% respectively. These tests are reasonable in patients with recurrent syncope and a normal heart who are not suspected to have an arrhythmia.8,60,110 If arrhythmia is suspected, then an ILR is more appropriate than HUT. In patients with infrequent episodes of syncope with a negative workup, ILR can detect arrhythmias in 42% of patients in the year after insertion. 111 A strategy of primary monitoring with an ILR is cost effective and may be used if the history, physical exam and external loop monitor are non-diagnostic. 112
Conclusion
A methodical approach to evaluating patients with syncope allows effective delivery of care. A thorough history and physical are critical. A 12-lead ECG recording and a diagnostic echo-cardiogram will screen for most cardiac causes of syncope. Ordering multiple additional tests is rarely necessary or effective. There are multiple etiologies of syncope and an appreciation of the pathophysiology can assist in the evaluation. The diagnostic tools are imperfect and their limitations must be appreciated in order to utilize them effectively. Indications for referring to a specialist must be known in order to identify and treat patients at risk of sudden death. Ongoing research into diagnostic tools and methods for risk stratification should improve diagnosis and treatment in the future. Genetic screening for identifying patients suspected to be at risk for a heritable syndrome may help establish a definitive diagnosis in equivocal cases and may have prognostic value.
Disclosures
Dr. Lin had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
No funding organization or sponsor had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.