
Abstract
We treated 21 patients with organizing pneumonia (OP) associated with rheumatoid arthritis (RA) or related to biological disease-modifying antirheumatic drugs (DMARDs) at our institution between 2006 and 2014. Among these cases, 3 (14.3%) preceded articular symptoms of RA, 4 (19.0%) developed simultaneously with RA onset, and 14 (66.7%) occurred during follow-up periods for RA. In the case of OP preceding RA, increased levels of anti-cyclic citrullinated peptide antibodies and rheumatoid factor were observed at the OP onset. RA disease activity was related to the development of OP in the simultaneous cases. In the cases of OP developing after RA diagnosis, 10 of 14 patients had maintained low disease activity with biological DMARD therapy at the OP onset, and among them, 6 patients developed OP within the first year of this therapy. In the remaining four patients, RA activity was not controlled at the OP onset. All patients responded well to systemic steroid therapy, but two patients suffered from relapses of articular and pulmonary symptoms upon steroid tapering. In most of the RA patients, DMARD therapy was introduced or restarted during the steroid tapering. We successfully restarted a biological DMARD that had not been previously used for patients whose RA would otherwise have been difficult to control. In this study, we also perform a review of the literature on RA-associated or biological DMARD-related OP and discuss the pathogenesis and management of OP occurring in RA patients.
Keywords
Introduction
Organizing pneumonia (OP) is a specific type of interstitial lung disease (ILD) histologically characterized by the presence of intraluminal buds of granulation tissue within alveolar ducts and alveoli.1,2 In 1983, Davison et al first described eight OP patients with no evidence of an infective or other causative agent. In order to avoid confusion with postinfective OP, they introduced the term cryptogenic organizing pneumonia (COP). 3 Because the buds of granulation tissue often involve respiratory bronchioles, the same clinicopathologic entity was also described using the term bronchiolitis obliterans with organizing pneumonia (BOOP).4–7 Currently, COP is more widely used because the major pathological feature of this condition is intra-alveolar organization, and bronchiolitis obliterans is a result of an extension of such organizing lesions to bronchiolar lumens (the proliferative type of bronchiolitis obliterans) and is only an accessory finding. 8 In addition, the use of BOOP may cause diagnostic confusion with airway diseases, such as the constrictive type of bronchiolitis obliterans.9–12
OP also occurs in association with several underlying conditions that can cause lung injuries, such as infections, drug reaction, radiotherapy, aspiration, organ or bone marrow transplantation, and autoimmune inflammatory diseases (secondary OP).13–16 There is no clear difference in clinical features or radiological findings between COP and secondary OP.17,18 The presenting symptoms include constitutional symptoms with a flu-like illness, cough, and dyspnea. A markedly elevated erythrocyte sedimentation rate and C-reactive protein as well as peripheral blood neutrophilia are common findings. Lung function test shows a mild or moderate restrictive ventilator defect.
Rheumatoid arthritis (RA) is a common inflammatory rheumatic disease characterized by persistent synovitis of multiple joints and is also a systemic condition that often affects multiple extra-articular organs. Approximately 40% of RA patients suffer from some type of extra-articular manifestations, including ILD, during the course of their disease.19–21 Nevertheless, the etiology of RA-associated ILD remains to be clarified. Genetic defects in the regulatory mechanism of the immune system and a repeated or persistent environmental stress may produce chronically inflammatory and persistently destructive processes in the synovium and other organs. ILD is an important pulmonary complication in RA. Although it is difficult to confirm the exact prevalence and incidence of ILD, recent studies have shown that the prevalence of clinically significant ILD was 7.7%-12% in RA patients.22–25 Compared with other types of ILD, such as usual interstitial pneumonia (UIP) and nonspecific interstitial pneumonia (NSIP), OP associated with RA is less common and has a much better prognosis.26–30 In several instances, however, rapid progression and fatal outcomes have been reported.31–33 An association between the occurrence of OP and RA disease activity is still not completely understood. In addition, the relationship between biological disease-modifying antirheumatic drugs (DMARDs) and OP is poorly established.
In this study, we present all patients with RA-associated or DMARD-related OP who were admitted to our hospital from 2006 to 2014 and also review the recent medical literature with the intention of exploring the pathogenesis of RA-associated OP as well as DMARD-related OP. This study was approved by the Ethics Committee of NHO Kumamoto Saishunsou National Hospital and was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all patients.
Case Presentation
Between 2006 and 2014, we treated a total of 21 RA patients who had developed OP: 3 cases (14.3%) preceded articular symptoms of RA, 4 (19.0%) developed simultaneously with the onset of RA, and 14 (66.7%) occurred during follow-up periods with or without the use of DMARDs (Table 1). The mean age of all patients was 61.5 years (range, 41-85 years), and the male-to-female rate was 8:13. All patients complained of flu-like symptoms at the onset of OP. The patients underwent chest radiography, high-resolution computed tomography (HRCT), and transbronchial lung biopsy (TBLB), which revealed typical radiological and histological features of OP as mentioned in the latter half of this review. Serum anti-mycoplasma IgM antibody, urine pneumococcal antigen, urine Legionella antigen, or cytomegalovirus antigen pp65 was not detected. Bronchoalveolar lavage (BAL) fluids were negative for bacterial cultures and polymerase chain reaction testing of Pneumocystis jirovecii. Antibiotics were not effective in any of the cases. The diagnosis of RA was made according to the 1987 American College of Rheumatology (ACR) criteria or the 2010 ACR/European League Against Rheumatism (EULAR) criteria for the classification of RA.34,35 The patients received treatment with high-dose steroids for approximately one month, and then steroid doses were gradually reduced. The length of steroid tapering-off periods varied among patients because the timing of final steroid discontinuation was determined based on not only pulmonary conditions but also the disease activity of RA (Table 1). All patients responded well to systemic steroid therapy, but two patients suffered from relapses upon a tapering off of the steroid (cases 7 and 9).
Cases of OP occurring in RA patients at our institution.

DMARDs being used at the time of OP development. The time interval from the start of DMARD therapy to OP development is shown in parentheses. Nonbiological DMARDs without showing the duration were used for more than one year.
The normal range is ≤4.5 U/mL. High titer was defined as levels ≥90 U/mL.
The normal range is <15 lU/mL. High titer was defined as levels ≥100 lU/mL.
Levels of anti-CCP Abs at patients' first visits to our institution were high in all the cases (100-890 U/mL).
When the patients first visited our institution, cases 11, 13, 20, and 21 were negative for RF. In the other cases, RF levels were high (100-910 lU/mL).
OP patients were first treated with the high doses of steroid for approximately one month, and then the steroids were gradually tapered off, based on the patient's pulmonary condition and RA disease activity.
DMARDs used after OP development. The time interval from the start of steroid therapy for OP to the initiation of DMARD therapy is shown in parentheses, along with the duration of this therapy.
Cases of OP Preceding RA Development
We had three cases of OP in which respiratory signs and symptoms preceded articular symptoms of RA. The time interval from the presentation of OP to the diagnosis of RA varied, ranging from 4 to 32 months (cases 1-3). All patients first visited a pulmonary section of our hospital because of the pulmonary symptoms. Upon examination after initial hospitalization, the patients were positive for anti-cyclic citrullinated peptide antibodies (anti-CCP Abs) and positive for rheumatoid factor (RF), and in most cases, the levels of these antibodies were high. We therefore performed radiographic examinations on the hands, wrist, and feet, but there was no evidence of arthritis at the presentation of OP, and no patients complained of articular symptoms at this point in time. Thus, no patients fulfilled the 1987 ACR criteria or the 2010 ACR/EULAR criteria for RA diagnosis. After hospitalization, the patients responded well to the treatment with high-dose steroids. Upon leaving the hospital, we strongly recommended the patients to visit us immediately if articular symptoms appeared. During the steroid tapering, they regularly visited our hospital for checkups of pulmonary and articular symptoms, chest radiographs, radiographs of joints (the hands, wrists, and feet), and serum levels of C-reactive protein and erythrocyte sedimentation rate. Even after completing steroid therapy, the patients visited us at least once every six months and received these examinations. In cases 1 and 2, the patients eventually developed articular symptoms 28 and 18 months after the discontinuation of steroid therapy, respectively. Once the RA diagnosis was made, DMARD therapy with methotrexate (MTX) was started. In case 3, articular symptoms appeared during the steroid tapering. The patient was diagnosed with RA based on the 2010 ACR/EULAR criteria. Because the patient's RA activity was high, humanized anti-IL-6 receptor monoclonal antibody (tocilizumab, case 1) was used as the first DMARD.
Cases of a Simultaneous Onset of OP and RA
We treated four patients with simultaneous development of OP and RA (cases 4-7). All the patients presented with flu-like symptoms and arthralgia of multiple joints simultaneously. At the onset of both conditions, they exhibited moderate-to-high levels of disease activity for RA, anti-CCP Abs, and RF, and they eventually met the 1987 ACR criteria or the 2010 ACR/EULAR criteria for RA diagnosis. There was no evidence for infectious causes or other characteristic contexts known to be associated with OP. All the patients responded well to a one-month course of high-dose steroid therapy. Pulmonary conditions improved markedly, as evidenced by HRCT scans, and respiratory symptoms cleared up. During the tapering off of steroids, MTX was introduced to all of these patients as the first-line DMARD for RA. In three patients (cases 4-6), their RA was well controlled after the discontinuation of steroid therapy, and no relapse of OP occurred. One patient (case 7), however, experienced a simultaneous flare-up of pulmonary and articular symptoms five months after the start of steroid tapering. The addition of a calcineurin inhibitor tacrolimus as the second-line DMARD produced favorable outcomes.
Cases of OP Occurring after the Diagnosis of RA
We treated 14 patients who had developed OP during the follow-ups for RA (cases 8-21). The period from the RA onset to the presentation of OP varied, ranging from 17 months to 40 years. Among these patients, two exhibited high disease activity (cases 9 and 12) at the presentation of pulmonary symptoms and/or signs. In case 9, RA activity had been controlled by etanercept therapy, but the treatment was stopped for economic reasons. Five months later, the patient developed pulmonary symptoms together with pain and swelling in multiple joints. In case 12, RA activity remained high despite MTX therapy. In cases 17 and 19, RA disease activity was not controlled, despite two or three months of etanercept therapy, and remained at moderate levels. In case 19, the patient had previously suffered from OP during MTX monotherapy, and she developed this condition shortly after the addition of MTX to etanercept therapy. This case was apparently an example of MTX-related OP.
In the other 10 cases, RA disease activity was low while under treatment with biological DMARDs, including tumor necrosis factor (TNF) inhibitors (infliximab: chimeric anti-TNFα monoclonal antibody, etanercept: soluble TNF receptor; adalimumab: humanized anti-TNFα monoclonal antibody, and certolizumab pegol: antigen-binding fragment of humanized anti-TNFα monoclonal antibody conjugated to polyethylene glycol) and tocilizumab, but the patients nevertheless developed OP. All patients, except for case 18, received MTX concomitantly with biological DMARDs. Cases 14 and 15 received additional tacrolimus because the RA disease control was not sufficient with a combination therapy of a biological DMARD and MTX. The duration of biological DMARD therapy varied, ranging from 1 to 60 months. Six patients developed OP within the first one year of biological DMARD therapy. Although there is a possibility that these cases were a manifestation of pulmonary toxicity of biological DMARDs used for RA, we were not able to establish a clear relationship between the development of OP and the use of these drugs. It may be less likely that these cases were MTX-related hypersensitivity because the patients had received MTX monotherapy for more than one year before the introduction of biological DMARDs.
DMARDs were withdrawn upon the development of OP. One month of high-dose steroid therapy induced a dramatic recovery from OP without any relapse in all cases except case 9. During the steroid tapering, we added MTX (for cases 10, 12-15, 17, and 20) and/or a biological DMARD (for cases 8, 15, 18, and 19) in order to control RA disease activity. Because there was a possibility of biological DMARD-related OP, we prescribed a biological DMARD that had not been previously used. For two cases, tocilizumab (case 17) and tofacitinib (case 20), a novel synthetic DMARD designed to target Janus kinases was prescribed after completing steroid therapy for OP. So far, no relapse has been seen in any of the cases. In case 9, MTX was not used because of the patient's medical history of MTX-induced pancytopenia. The patient suffered from a relapse of OP and RA during the steroid tapering. Introducing tocilizumab therapy improved both conditions, and the steroid was successfully tapered off. Currently, the patient's disease activity is well controlled by abatacept, a T-cell signaling inhibitor. In the other three cases (cases 11, 16, and 21), no type of DMARD therapy was restarted because RA disease activity remained low, even after completing steroid therapy for OP.
Literature Review
Using the PubMed database, we performed an electronic search of the published literature as of March 31, 2015. The following keywords and subject terms were used in the search: “organizing pneumonia,” “bronchiolitis obliterans,” “rheumatic disease,” and “rheumatoid arthritis.” Studies were confined to OP cases occurring in patients who had been diagnosed with RA before, simultaneously with, or after the development of OP. Studies that did not provide detailed information on RA were excluded. Patients who had not fulfilled the 1987 ACR criteria or the 2010 ACR/EULAR criteria for RA diagnosis were also excluded. Through this literature search, we evaluated a total of 129 articles and identified 27 cases of RA-associated OP (Table 2) and 7 cases of biological DMARD-related OP in RA patients (Table 3).
Cases of OP associated with RA in the literature.

RA duration was defined as the time interval between the diagnosis of RA and the presentation of OP.
RF was measured by latex agglutination test (positive or negative), RA particle agglutination test, or quantitative analysis.
The patients did not receive any treatment for OP, but they started intra-articular injection of steroid for joint pain (case 30, prednisolone into knee; case 46, methylprednisolone into knee and hip).
In these cases, anti-CCP and/or RF were positive at the onset of RA (case 22, RF, 1:640; case 24, anti-CCP, 268 U/mL; case 25, RF, 1:160, anti-CCP, 198 U/mL; case 26, RF, positive, anti-CCP, titration 5.9 for a positivity threshold of 1; case 39, RF, 1:160, anti-CCP, 524 U/mL).
The patient did not discontinue D-penicillamine after the development of OP.
In these cases, the patients discontinued DMARD therapy shortly before the development of OP (case 38, penicillamine and gold injection, two months before; case 41, prednisolone, one month before).
Cases of OP related to biological DMARDs occurring in RA patients.
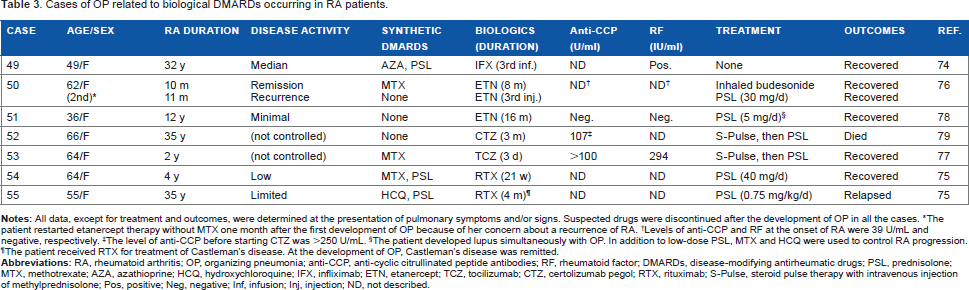
The patient restarted etanercept therapy without MTX one month after the first development of OP because of her concern about a recurrence of RA.
Levels of anti-CCP and RF at the onset of RA were 39 U/mL and negative, respectively.
The level of anti-CCP before starting CTZ was >250 U/mL.
The patient developed lupus simultaneously with OP. In addition to low-dose PSL, MTX and HCQ were used to control RA progression.
The patient received RTX for treatment of Castleman's disease. At the development of OP, Castleman's disease was remitted.
The mean age of all cases of RA-associated OP in the literature was 59.0 years (range, 21-86 years). The male-to-female ratio was 12:15. The mean age of all cases of biological DMARD-related OP in the literature was 56.6 years (range, 36-66 years), and all were female. In the case of COP, males and females are equally affected, with the mean age at onset being 50-60 years, 15 which may be applicable to RA-associated OP. A female predominance was observed in the biological DMARD-related OP cases, but the reason for this disparity was not clear. Antibiotics were not effective in any of the cases. Most cases had favorable outcomes through systemic steroid therapy with or without the additional use of a DMARD. Three patients did, however, eventually die (cases 34, 36, and 52).
Onset, RA Disease Activity, Serum Levels of Anti-CCP Abs and RF, and Outcomes in RA-Associated OP Cases
Through reviewing clinical data obtained from RA-associated OP cases in the literature (Table 2) along with those of our cases (Table 1), we addressed several issues that may be associated with the pathogenesis of OP.
Serum Levels of Anti-CCP Abs and RF in Patients with OP Preceding RA Development
We identified seven cases of OP appearing prior to the development of RA (cases 22-28).36–41 The interval between pulmonary and articular symptoms ranged from two weeks to two years. Among these seven cases, three were positive for anti-CCP and RF at the presentation of OP (cases 23, 27, and 28), while one case was negative for RF at this time (case 25). In the other three cases, there was no information regarding anti-CCP Abs or RF at the OP onset (cases 22, 24, and 26). Following the development of articular symptoms, however, these four patients showed positive results for anti-CCP Abs and/or RF, and titers of both antibodies were high. In cases 22-24, articular symptoms appeared before steroid therapy for OP was started. In cases 25 and 26, articular symptoms presented during the steroid tapering. In cases 27 and 28, the patients developed RA several months after the discontinuation of steroid therapy for OP.
A number of cohort studies have shown that the appearance of anti-CCP Abs and RF often predates the development of clinically apparent articular inflammation in patients who are ultimately diagnosed with RA. Thus, these autoantibodies can be used as predictors for the future development of RA. 42 Similarly, the detection of anti-CCP Abs has been reported in many cohort studies on patients with early disease, those with undifferentiated arthritis, and those with nonspecific musculoskeletal symptoms.43–45 Currently, the status of anti-CCP Abs and RF are the only autoimmune antibodies that have been included as serological markers in the 2010 ACR/EULAR criteria for the classification of RA. This new set of classification criteria defines the disease by focusing on its earlier stage features. 35 The initiation of DMARDs at the early stages of RA is strongly recommended, which has changed the course of RA and provided patients with the best outcomes and quality of life.46,47 It is, therefore, very important to make the diagnosis of RA as early in the disease stages as possible. Without the serological status of these two markers, we may fail to identify the COP patients at an increased risk of RA. As shown in Tables 1 and 2, among the OP cases preceding RA development in which data on anti-CCP Abs and RF were available, all except one were positive for these autoantibodies at the OP onset. We should, therefore, urge physicians to continue with the follow-up observations for COP patients, especially for those positive for anti-CCP Abs and/or RF. Measuring anti-CCP Abs and RF levels can provide useful information on the risk of future development of RA in OP patients.
RA Disease Activity at the Onset of OP in Simultaneous Cases
In the literature, we found no simultaneous onset case of OP and RA except for one of our cases (case 4 in Table 1). 48 As shown in Table 1, all simultaneous onset cases exhibited high or moderate RA disease activity at the onset of OP. In three cases, the RA disease activity was well controlled after the improvement of OP, and since this time, no relapse of OP has occurred (cases 4-6, follow-up periods of 43-76 months). In one patient, articular symptoms had rapidly exacerbated five months after the recovery from OP, followed by a reappearance of pulmonary symptoms (case 7). These findings suggest that OP may be a pulmonary reaction in the inflammatory process associated with RA.
RA Disease Activity and Serum Anti-CCP Abs and RF Levels at the Onset of OP in Cases Occurring during the Follow-Ups for RA
We found 20 cases of OP in which RA patients developed OP during the follow-ups.31,33,49-64 In all patients except two (cases 35 and 44), for whom data are available, RF was positive at the onset of OP, and in most cases, the titers were high. In cases 29 and 32, seroconversion for RF was observed at the OP onset. In cases 38 and 41, a rapid increase in RF values was observed during the development of OP (case 38, 1:2560 to 1:5120; case 41, 364 to 1460 IU/mL).
Among all patients except two (cases 35 and 39), for whom data are available, RA disease activity had flared up or was not controlled at the time of OP onset. In cases 29, 30, 34, 36, 40, and 46-48, the patients had not received any DMARDs, and therefore, disease activity was not controlled at the onset of OP. Two patients received synthetic DMARDs, but their disease activity was not controlled (cases 42 and 43). In cases 31-33 and 37, despite receiving antirheumatic therapy, such as synthetic DMARDs and/or steroids, joint symptoms flared up. In cases 38 and 41, antirheumatic therapy had been discontinued one or two months prior to the development of OP. These findings suggest a possible relationship between OP development and RA disease activity.
In cases 35 and 39, the patients developed OP while their disease activity for RA remained at low levels. Case 35 was seronegative RA, in which articular symptoms were not exacerbated despite giving no treatment for RA. In case 39, the patient had received treatment with methylprednisolone and hydroxychloroquine for six months when OP developed. It is not clear whether this case was a drug-related OP.
Outcomes of RA-Associated OP in the Literature
In the cases of OP preceding RA development, all cases responded well to systemic steroid therapy. In case 26, the reappearance of OP, together with the appearance of articular symptoms, was observed upon the steroid tapering. The addition of MTX as the first-line DMARD for RA induced a clinical and radiological improvement. In case 25, articular symptoms developed during the steroid tapering, which were improved by the start of DMARD therapy with MTX plus etanercept. In two cases, articular symptoms recurred during the steroid tapering, which were improved by the use of hydroxychloroquine (case 24) or MTX and bucillamine (case 23) in DMARD therapy for RA.
In the cases of OP occurring after the diagnosis of RA, all cases except two (cases 34 and 44) rapidly responded to steroid therapy, but two (cases 33 and 36) suffered from a recurrence of OP during the steroid tapering. In one case (case 33), an addition of cyclophosphamide produced a successful steroid tapering. The other was a fatal case (case 36); the patient died nine months after the onset of OP despite the additional use of cyclophosphamide and azathioprine. Cases 34 and 44 were steroid-resistant cases, in which the patients received aggressive care (pulse therapy with steroid and cyclophosphamide). In case 34, the patient died due to severe respiratory failure, while the other patient (case 44) completely recovered. In case 48, the patient's condition was complicated by pericarditis during steroid therapy. Fortunately, tocilizumab induced a rapid recovery of this condition.
The two fatal cases (cases 34 and 36) revealed that there is a subset of patients with RA-associated OP who present with a fulminant course leading to death. In case 34, an open lung biopsy was performed at the OP onset, which showed the typical pathological features of OP. No data at postmortem examination were shown. In case 36, an open lung biopsy performed at the OP onset showed the typical OP pattern, but after relapse, an open lung biopsy revealed alveolar septal inflammation with severe fibrosis and areas of honeycombing, which is typical of UIP. A postmortem examination revealed end-stage honeycombing of the lung.
Two cases (cases 30 and 46) achieved complete remission simply through the intra-articular injection of steroid, which was performed as part of the treatment for arthritis (case 30, prednisolone into the knee; case 46, methylprednisolone into the knee and hip joint). One case (case 43) spontaneously recovered without any treatment for OP. The reinstitution of MTX did not modify the clinical course.
DMARD-Related OP
Synthetic DMARDs, such as gold salts, MTX, penicillamine, sulfasalazine, and cyclophosphamide, have been reported to cause iatrogenic OP.15,65,66 There are several cases of DMARD-related OP in the literature, in which RA patients were under treatment with leflunomide, 67 bucillamine (an analog of D-penicillamine),68–71 sulfasalazine, 72 and MTX. 73 But a direct relationship between drug administration and OP development was not completely established in these cases.
There are several case reports suggesting that OP may appear as drug toxicity caused by biological DMARDs for RA patients (Table 3).74–79 Suspected drugs were discontinued after the development of OP in all the cases. In case 49, OP developed shortly after a third infusion of infliximab. The patient became asymptomatic three weeks after presentation, without any specific intervention. In case 50, the patient developed OP after eight months of etanercept therapy, although she had remained in remission. Steroid inhalation improved respiratory symptoms in this case. Shortly after the restart of etanercept therapy, however, a new infiltrate appeared on a chest radiograph. In case 53, the patient developed OP, accompanied by abnormal liver function data, three days after the first infusion of tocilizumab. A drug lymphocyte stimulation test for tocilizumab was positive. In case 51, the patient recovered following the etanercept cessation and low-dose steroid therapy. In cases 54 and 55, the patients' disease activity was low, but OP developed 21 weeks and 4 months after the introduction of rituximab (a chimeric anti-CD20 monoclonal antibody), respectively. Kaneko et al also reported two cases of OP out of 200 RA patients receiving adalimumab therapy, but it is not clear whether these cases were a direct manifestation of RA or a drug-induced lung injury. 80
Case 52 was a fatal case. OP occurred three months after starting certolizumab pegol therapy, and a surgical lung biopsy showed features consistent with OP. Despite systemic steroid therapy, the patient remained hypoxic and oxygen dependent through her admission. One month later, HRCT scans revealed a significant architectural distortion and traction bronchiectasis with rapidly evolving fibrotic lung disease. The patient had ongoing severe debility, and three months after discharge, she eventually died.
The pathogenesis of OP is more complicated in RA patients receiving DMARDs than in those not receiving RA therapy. Besides the possibility of direct toxicity, DMARDs may modify the inflammatory process of RA in the lung and cause pneumonitis or exacerbate preexisting ILD. 81 It is not clear which types of biological DMARDs are most strongly related to OP development. Because clinical features and radiographic findings are nonspecific and similar between COP, RA-associated OP, infectious OP, and DMARD-related OP,17,18 it is difficult to establish a causal relationship between OP and suspected DMARDs, especially without a clear temporal relationship. Drug initiation always precedes clinical symptoms or radiological findings, but the time interval between the last treatment cycle and the development of OP seems to vary. Even if patients have a medical history involving past or present medication use, it merely indicates the patients' exposures to drugs and does not necessarily establish drug toxicity. This type of diagnosis is made mainly by excluding other possible causes.
Pathological and Clinicoradiological Features of OP
Pathological Findings
The definitive diagnosis of OP depends on the pathological features, namely, the presence of intralumenal buds of loose granulation tissue consisting of fibroblasts embedded in connective tissue (Fig. 1). The buds extend into the alveolar ducts and alveoli (intra-alveolar organization) but often fill bronchiolar lumens. The connective tissue is all the same age, and the distribution of lung involvement is patchy. A variable degree of interstitial infiltration with mononuclear cells is present in the areas of OP, but this inflammation is usually mild. There may be focal alveolar accumulations of foamy macrophages, but lung architecture is relatively preserved. The pathological pattern of OP is not specific for determined causes or associated underlying conditions/clinical contexts but rather reflects one type of inflammatory process resulting from lung injury.14,15,82,83 Actually, as shown in Table 2, most cases of RA-associated OP occurred in patients whose disease activity was not controlled or had flared up.

A histological examination of a TBLB specimen shows intraalveolar buds of granulation tissue consisting of intermixed myofibroblasts and connective tissues. Interstitial infiltrates of mononuclear cells are seen (case 1; HE staining, original magnification × 400).
Open lung biopsy, video-assisted thoracoscopic surgery biopsy, and percutaneous/transthoracic needle biopsy under computed tomography (CT) guidance (CT-guided needle biopsy) are preferred in the diagnosis of OP, while TBLB often fails to obtain a large and adequate piece of lung tissue to make the differential diagnosis with confidence.14,82 Although surgical biopsy remains the gold standard diagnostic tool for OP, CT-guided needle biopsy is considered as an alternative because it provides larger samples of lung tissue than does TBLB. 84 These invasive tests may be unnecessary for patients diagnosed with RA and those with high levels of anti-CCP Abs and/or RF if these patients have typical clinical and radiological findings of OP. We should consider risks and complications of lung biopsies. Possible serious complications may include, but are not limited to, bleeding in the lungs, infection, and pneumothorax. In particular, the mortality rate within 30 days after surgical lung biopsy was reported to be 0%-22%. 85 In addition, this procedure is not appropriate for patients with arterial and venous pulmonary hypertension, those with a serious bleeding disorder or coagulation abnormalities, those with lung blood vessel abnormalities, and those with respiratory insufficiency. A provisional diagnosis of OP allows for the rapid introduction of steroid therapy, but a careful follow-up and patients' informed consent are required.
Cohen et al reported histological features in seven patients with rapidly progressive OP that had resulted in severe respiratory failure and death. The patients had characteristic histological findings of OP in open lung biopsy at onset, but the predominant histological pattern was UIP (alveolar septal inflammation with severe fibrosis and honeycombing areas) at the relapse and end-stage honeycombing at autopsy. These findings suggest that early lung injury rapidly progressed to steroid-resistant fibrotic lung disease. 31 Chang et al also reported six patients with rapidly progressive, fatal OP in whom open lung biopsy specimens showed more severe interstitial inflammation and alveolar septal fibrosis compared to those in patients with good prognoses. The authors speculated that the intra-alveolar organization might represent an early phase of the temporal spectrum of ILD. 32 Therefore, we may consider it prudent to perform a lung biopsy when we encounter patients who show unfavorable or atypical evolution under steroid treatment, even if they have previously been diagnosed with OP. We will of course keep in mind that the intra-alveolar organization is a nonspecific feature that can also be seen in early lesions of other types of RA-associated ILD, and in some cases, OP may overlap with the organizing stage of more fibrotic ILDs, such as UIP.
Radiological Findings
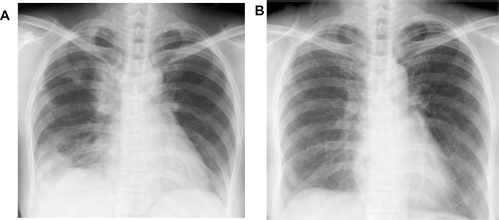
Chest radiography is characterized by multiple patchy alveolar opacities, which are bilateral or unilateral in the peripheral regions (Fig. 2). Their sizes vary, ranging from a few centimeters to an entire lobe. Although most of the findings are apparent on radiographs, CT scans more accurately depict the anatomic distribution and extent of OP. The most common CT features include multiple patchy alveolar opacities in a predominantly subpleural and peribronchial distribution (Fig. 3). The lower lung zones are more often involved. The density of the opacities varies from ground glass to consolidation. Bronchial wall thickening and cylindrical bronchial dilatation are also commonly seen in the areas of an air bronchogram.15,83 Such lesions are nonsegmental 86 and often migrate spontaneously during the course of the disease.13,56,87-89
(
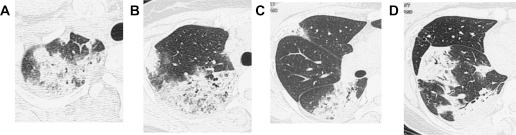
HRCT shows multiple patchy areas of consolidations with an air bronchogram in the right lung (case 1). These lesions are nonsegmentally distributed in S1 and S2 (
The differential diagnosis of RA patients with multiple alveolar densities on CT scans mainly includes infection, pneumonic-type adenocarcinoma, pulmonary lymphoma, and chronic eosinophilic pneumonia (CEP). Most of these diagnoses can be excluded by TBLB.15,83 An association between CEP and RA has been previously described. In most cases, arthritis was not controlled or had flared up at the appearance of pulmonary symptoms and radiological findings.90–94 Simultaneous onset cases of CEP and RA have also been reported.95–97 In addition, there are several cases reported in which CEP antedated joint symptoms.91,98 These clinical features are reminiscent of RA-associated OP. In many cases, the discrimination between OP and CEP may be possible on HRCT scans; however, these diseases can be differentiated with confidence in only a small percentage of cases. 86 An eosinophil number >40% in BAL fluids is highly suggestive of CEP, but the definitive diagnosis is made based on the histological examinations of lung biopsies.
Less commonly, CT scans reveal single or multiple nodules or masses, which create diagnostic problems with malignancy. 16 These nodules and masses have an irregular margin with the areas of an air bronchogram and, less often, pleural tags, spicules, pleural thickening, parenchymal bands, and focal thickening of interlobular septa. 99
Akira et al reported five RA patients who exhibited consolidation as the predominant pattern on thin-section CT scans. Among these, three cases were RA-associated OP and one was an overlapping case between OP and CEP, as evidenced by histological findings. In one RA-associated OP case and one overlapping case, consolidation persisted despite steroid therapy and evolved into honeycombing at serial CT scans. Another patient with RA-associated OP responded well to steroid therapy, and the consolidation disappeared. Two years later, however, steroid-resistant reticular opacities were seen on CT scans, which progressed to honeycombing, as evidenced by serial CT scans. Sequential monitoring of disease morphology by CT scans is noninvasive and useful in evaluating the prognosis of OP. 100
BAL Fluids
BAL fluid analysis shows increases in total cell numbers and lymphocyte percentages (up to 40%). Increases in neutrophils and eosinophils may be observed, but the lymphocyte number is higher than the eosinophil number. The ratio of CD4+ to CD8+ cells usually decreases.15,83
Treatment and Outcomes
The most interesting characteristic of COP is its reversibility in response to steroid therapy.87,89,101-103 In this respect, COP is distinguished from irreversible lung fibroses, such as idiopathic pulmonary fibrosis, and also from the constrictive type of bronchiolitis obliterans that is mainly characterized by airflow obstruction. It is not clear why the fibrotic tissue in COP can completely resolve itself in response to steroid therapy, while the fibroblastic process in the UIP lesion participates in the remodeling and progresses to end-stage fibrosis. 83 Nevertheless, some COP cases had unfavorable outcomes. Through histological comparisons between patients with steroid-responsive COP and progressive COP despite therapy, Yousem et al showed that the latter were accompanied by scarring and remodeling of the background lung parenchyma in 89% of cases, while the former were accompanied by these conditions in only 10% of cases. It remained unclear whether the progressive COP cases have a tendency to cause irreversible injury to the lung during the course or whether such cases represent a COP-like pattern in patients with an associated fibrosing ILD, especially UIP. 104
COP and secondary OP have similar treatment responses, relapse rates, and mortality rates. 18 However, Yoo et al showed that inflammatory rheumatic disease-related cases showed a lower complete recovery rate with a tendency toward a higher recurrence rate compared with COP cases. 17 Inflammatory rheumatic disease-related OP may be more likely to be poorly steroid responsive.88,103,105 As mentioned above, several fatal cases were reported occurring in RA patients despite extensive therapy.31,33,79
Steroid therapy can mask articular symptoms of underlying RA. There are several cases of OP preceding RA in our patients and in the literature, in which articular symptoms appeared upon the tapering of steroid dosage (cases 3, 25, and 26). Strict follow-ups are required after the disappearance of OP, especially for patients who had high levels of anti-CCP Abs and/or RF.
As mentioned above, the ACR and EULAR recommendations for biological and nonbiological DMARDs in the treatment of RA have stated that therapy with DMARDs be started as soon as the diagnosis of RA is made.46,47 Once a diagnosis of RA is made for patients who have developed OP prior to or simultaneously with the development of articular symptoms, we should consider introducing MTX as the first-line DMARD, as it not only reduces radiographic progression but also produces a steroid-sparing effect. Similarly, for patients who have developed OP during the follow-ups for RA, the introduction or restart of MTX should be considered during the steroid tapering, if not contraindicated, as it can prevent a flare-up of pulmonary and articular symptoms. Although biological DMARD-related lung injury has been reported, it seems to be relatively rare. 106 The additional use of biological DMARDs to MTX may be worth considering as one of the therapeutic options for steroid-resistant or recurrent cases of RA-associated OP. Drug-related OP is treated with drug withdrawal and steroid therapy. It may be difficult to decide to restart antirheumatic therapy with biological DMARDs, but there is concern that the disease activity of RA may be increased after the steroid tapering, and therefore, pulmonary manifestations of OP may recur. In such cases, it is reasonable to use a biological DMARD that has not been previously used.
Conclusions
The main limitation of the present study is its small sample size. OP occurred less commonly in RA patients than did NSIP and UIP, and the low incidence rate makes it difficult to perform a large-scale cohort study. Nevertheless, through our experience and a comprehensive review of the literature, we have reached a number of interesting hypotheses. Although OP is sometimes observed during the course of RA as one of the pulmonary involvements, we should pay careful attention to the presence of OP preceding or developing simultaneously with articular symptoms. In such cases, respiratory manifestations are both the first and the principle evidence of RA activity. Testing of anti-CCP Abs and RF is useful in predicting the future development of RA. We need a careful follow-up on the pulmonary signs and symptoms of those patients whose disease activity is not controlled or has flared up. OP can also result from drug toxicity of biological and synthetic DMARDs, which complicates the pathogenesis of OP in RA patients receiving DMARDs. It is difficult to establish a causal relationship between OP and suspected DMARDs, especially in cases without a clear temporal relationship, and so diagnosis requires a high index of suspicion. Fortunately, the prognosis of OP is usually good. The addition of MTX during the steroid tapering should be considered for patients who were diagnosed with RA, if MTX is not contraindicated, as it is effective in preventing the exacerbation of articular symptoms as well as OP recurrence. Some OP cases may progress to steroid-resistant fibrotic lung disease. A lung biopsy may not necessarily be required for RA patients who exhibit typical clinical and radiological findings, but a biopsy should be considered early for patients who show unfavorable or atypical evolution under steroid treatment, even if the first histological examination yields a diagnosis of OP. It can be a safe option to restart a biological DMARD that has not been previously used for RA patients who are suspected of having drug-related OP.
Author Contributions
Conceived the concept and design: SM, MS. Analyzed the data: SM, YK, MS. Wrote the first draft of the manuscript: SM, MS. Contributed to the writing of the manuscript: SM, YK, MS. Agree with manuscript results and conclusions: SM, YK, MS. Jointly developed the structure and arguments for the paper: SM, YK, MS. Made critical revisions and approved final version: SM, YK, MS. All authors reviewed and approved of the final manuscript.