
Abstract
We determined whether a non-invasive gas exchange based estimate of pulmonary vascular (PV) capacitance [PVCAP = stroke volume (SV) x pulmonary arterial pressure (Ppa)] (GXCAP) tracked the PV response to exercise in heart-failure (HF) patients. Pulmonary wedge pressure (Ppw), Ppa, PV resistance (PVR), and gas exchange were measured simultaneously during cycle exercise in 42 HF patients undergoing right-heart catheterization. During exercise, PETCO2 and VE/VCO2 were related to each other (r= -0.93, P < 0.01) and similarly related to mean Ppa (mPpa) (r = -0.39 and 0.36; P < 0.05); PETCO2 was subsequently used as a metric of mPpa. Oxygen pulse (O2 pulse) tracked the SV response to exercise
Introduction
Simple, non-invasive metrics to accurately quantify pulmonary hypertension (PH), particularly to assess the pulmonary vascular (PV) response to exercise in these patients, are lacking. 1 Recent studies have suggested that non-invasive measures of pulmonary gas exchange during exercise, including end-tidal CO2 (PETCO2) and ventilatory efficiency (VE/VCO2), may be useful indicators of the altered PV pressures associated with PH.2,3
PH, however, is also a hallmark of chronic heart failure (HF). In patients with left ventricular (LV) dysfunction, PH initially manifests as a “passive” increase in pulmonary venous pressure caused by the elevation in LV filling pressure. 4 Subsequently, patients with chronically elevated pulmonary capillary wedge pressure (Ppw) develop a form of PV disease that is associated with vasoconstriction and/or remodeling of the pulmonary arterial resistance vessels. This “reactive” component of PH is characterized by an excessive rise in pulmonary arterial pressure (Ppa) relative to the increase in Ppw, with a rise in PV resistance (PVR).5,6 Importantly, development of reactive PH is associated with a further increase in mortality in the HF population. 7 Like idiopathic pulmonary arterial hypertension (IPAH) patients, HF patients also demonstrate gas exchange abnormalities during exercise, including significant alterations in PETCO2 and VE/VCO2.8–10 Given that both disease processes (i.e. IPAH and chronic HF) have a significant impact on both PETCO2 and VE/VCO2, the ability to detect or estimate the presence of PH in diagnosed HF patients using these gas exchange parameters is likely limited. Accordingly, identification of other simplified metrics to determine the presence and severity of PH secondary to HF may be important.
One such measure that has received attention is an assessment of PV capacitance (PVCAP), which can be defined as the ability of the pulmonary vessels to accept a volume of blood under a given pressure (eg, PVCAP = stroke volume/Ppa). This measure has been related to prognosis and survival in PH populations.11,12 Typically, PVCAP is calculated from highly invasive right heart catheterization or technically difficult echocardiographic measures.11,12 It may be possible, however, to estimate PVCAP using easily assessable non-invasive pulmonary gas exchange surrogates [ie, oxygen pulse (O2 pulse) and PETCO2, representing blood volume and PV pressure, respectively]. 13 Indeed, it has been shown that there is a significant relationship between the O2 pulse and SV responses to exercise. 14 Moreover, we have demonstrated previously that PETCO2 measured during submaximal exercise allows discrimination between patients with differing severities of pulmonary arterial hypertension. 15
Thus, the aim of the present study was to assess the validity of a gas exchange based estimate of PVCAP (GXCAP) relative to invasively obtained measures. We hypothesized that a combination of O2 pulse and PETCO2 would track invasive measures of PVCAP better than the more common measures of either PETCO2, or VE/VCO2 alone.
Materials and Methods
Participants
Forty-two adult patients from the Mayo Clinic Heart Failure Service undergoing right heart catheterization participated in this study (Table 1). Of the 42 patients, 29 were classed as HF with PH and 13 were classed as HF only. Each participant gave written informed consent after being provided a detailed description of the study requirements. The experimental procedures were approved by the Mayo Clinic Institutional Review Board and were performed in accordance with the ethical standards of the Declaration of Helsinki. Functional class ranged from New York Heart Association (NYHA) classification II-IV and patients were prescribed a range of typical cardiac medications, including beta blockers, ACE inhibitors, angiotensin II antagonists, aspirin, and diuretics.
Subject characteristics and resting pulmonary hemodynamics.

Experimental Procedures
With patients well rested and in the supine position, a 22-gauge indwelling catheter was placed in the radial artery and a 7-French Swan-Ganz balloon-tipped catheter was advanced to the pulmonary artery through the right side of the heart via the right internal jugular vein. This allowed for the measurement of systolic, diastolic, and mean arterial pressure (SBP, DBP, and MAP), mean pulmonary artery and pulmonary wedge pressure (mPpa and mPpw), and arterial and mixed-venous blood gases. Cardiac output (Q) was calculated via the direct Fick method (Q = VO2/ CaO2-CvO2). PVR (PVR = mPpa -mPpw/Q) and pulmonary artery capacitance (PVCAP = SV/mPpa) were also calculated.
Following instrumentation, the patients performed incremental cycle exercise on a semi-recumbent ergometer (starting at 20 W and increasing by 10 W every 3 min) until they achieved a perceived exertion (RPE) of ∼16 on the Borg Scale 6-20. Patients maintained a constant cadence (∼60 rpm) throughout exercise. Pulmonary hemodynamics as well as simultaneous breath-by-breath measures of minute ventilation (VE), breathing frequency (fb), tidal volume (VT), oxygen consumption (VO2), carbon dioxide production (VCO2), respiratory exchange ratio (RER), and the partial pressure of end tidal CO2 (PETCO2) (via a metabolic gas analysis system) were taken at rest and throughout exercise. Ventilatory efficiency (VE/VCO2), oxygen pulse (VO2/HR), and a gas exchange equivalent of PVCAP (GX 2 CAP = O2pulse x PETCO2) were also calculated. All data were averaged over 60 s intervals.
Data Analyses
Linear regression analysis was performed using all HF patient data to assess the relationships between hemodynamic and pulmonary gas exchange data during exercise. To assess the ability of gas exchange metrics to differentiate between patients with and without PH, the HF group was split according to resting mPpa. Following current guidelines, patients with an mPpa >25 mmHg were deemed to have PH (HF-PH, n = 29). Independent sample t-test was used to compare hemodynamic and gas exchange measures during the final minutes of exercise in HF vs. HF-PH patients. Results are expressed as means ± SD and the acceptable type I error was set at P < 0.05. Statistical analyses were performed using SPSS version 12.0 for Windows (SPSS, Chicago, IL).
Results
Subject Characteristics
Participant characteristics are shown in Table 1 The majority of patients were male with a relatively even number of ischemic and idiopathic HF etiologies. Patients were predominantly NYHA functional class III, with a modest number of class II and class IV patients. LV ejection fraction was on average severely reduced with moderate elevations in mPpa, mPpw, and PVR relative to reported normal values.
Exercise Hemodynamics and Gas Exchange
Hemodynamic and non-invasive gas exchange responses to the final minute of exercise are shown in Table 2 With exercise, there was an increase in cardiac output (48% ± 32%, range 0.11 to 3.95 L/min), mPpa (58% ± 53%, range 1 to 35 mmHg) and mPpw (61% ± 86%, range -4 to 31 mmHg). Group mean PVR increased minimally during exercise (+6% ± 55%, range -8 to +3 WU). The average VE/VCO2 ratio was elevated and consistent with poor breathing efficiency while PET CO2 was reduced.
Hemodynamic and gas exchange responses to the final minute of exercise.

During exercise, PETCO2 and VE/VCO2 were similarly and modestly related to mPpa (Table 3 and Figure 1). Since VE/VCO2 and PETCO2 were highly correlated with each other (r = 0.93, P < 0.01), we chose to use PETCO2 as a general metric of mPpa with exercise. In addition, O2 pulse tracked the stroke volume response to exercise in HF (r = 0.91, P< 0.01) (Fig. 1). Accordingly, we used O2 pulse as a non-invasive estimate of SV for calculating the GXCAP.
Correlations between key exercise hemodynamic and pulmonary gas exchange measures.
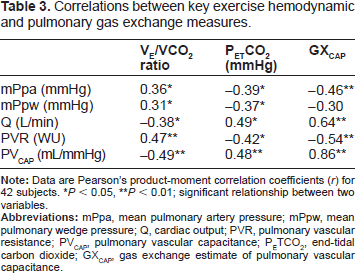
P < 0.05
P < 0.01; significant relationship between two variables.

Linear regression analysis of all HF (42 subjects) data examining the relationship of invasive hemodynamic and non-invasive gas analysis measures during exercise. The relationship of SV and O2 pulse
There was a highly significant positive relationship between the invasively derived measure of PVCAP and GXCAP with exercise (r = 0.86, P< 0.01) (Fig. 1). Moreover, GXCAP correlated modestly with mPpa, Q, and PVR, with incremental improvements over the correlation between these variables and the VE/VCO2 ratio or PETCO2 alone (Table 3).
Comparison of HF with and without PH
Exercise VO2, VCO2, O2 pulse, SV, and Q were markedly reduced in HF-PH patients compared to HF patients without PH (Table 4). By contrast, VE/ VCO2 was greater in HF-PH vs. HF patients, indicating poorer ventilatory efficiency in HF patients with PH (Fig. 2). Similarly, mPpa and PVR were elevated in HF-PH patients relative to patients with HF only (Fig. 2). Finally, both PVCAP and GXCAP were significantly reduced in the HF-PH group vs. the HF only group, suggesting that this metric may be used as an index to differentiate HF patients with and without PH.

Key exercise hemodynamic and gas exchange differences between HF patients with (HF-PH, n = 29) and without (HF, n = 13) PH. Mean and standard deviation are presented for mPpa
Hemodynamic and gas exchange responses to the final minute of exercise in heart failure patients with and without PH.
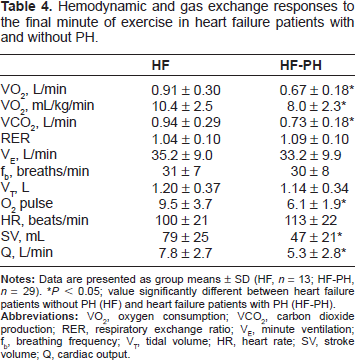
P < 0.05; value significantly different between heart failure patients without PH (HF) and heart failure patients with PH (HF-PH).
Discussion
Main Findings
The primary findings of the present study were that (1) non-invasive measures of PETCO2 and O2 pulse correlated closely with measures of mPpa and SV, respectively, (2) a non-invasive estimate of PVCAP (GXCAP) developed using the aforementioned surrogates of PV pressure and blood volume (GXCAP = O2pulse x PETCO2) correlated well with invasively derived PVCAP' (3) noninvasive measures of pulmonary gas exchange, specifically VE/VCO2, PETCO2 and GXCAP correlated significantly with invasive hemodynamic indices, including mPpa and PVR, and (4) VE/VCO2 and GXCAP during exercise were significantly different between HF patients with and without PH. In combination, these data potentially identify a unique non-invasive gas exchange parameter (ie, GXCAP) that may be used to track PV changes during exercise in HF patients. In addition, although somewhat speculative, it is possible that the GXCAP parameter may allow differentiation between HF patients with and without PH at rest. Further studies, however, are needed to support this conclusion.
The Link between the Heart and the Lungs
The lungs lie in series with the heart. Indeed, both organs share a common surface area and are exposed to similar intrathoracic pressures, receive nearly all of the cardiac output, and have receptors that are sensitive to pressure and extravascular fluid changes. Thus, it is unsurprising that diseases which influence one organ system (ie, the lungs or the heart) would affect the other.
It has been shown previously that the simple noninvasive gas exchange metrics VE/VCO2 and PETCO2 are markedly increased and decreased, respectively, during exercise in HF patients. 16 Moreover, both metrics are highly prognostic in the HF population and appear to track disease severity and response to therapy.17–19 The initial alterations in the VE/VCO2 and PETCO2 response to exercise in the HF population are most likely the result of a reduced blood flow to the pulmonary blood vessels with a consequent increase in the inhomogeneity of ventilation and perfusion matching, in particular high VA/Qc ratios in the lungs resulting in high dead space ventilation.17,20 Also, the reduction in blood supply to the skeletal muscles, arterial hypoxemia, and right-to-left shunting, all of which alter blood carbon dioxide, oxygen, and H+ ion concentration, are likely contributors to the enhanced drive to breathe, the greater hyperven-tilatory response, and altered VE/VCO2 and PETCO2 response to exercise in this population secondary to stimulation of the peripheral chemoreceptors. With the development of substantial PH (ie, a marked increase in PV pressures) there is a widening of the arterial to PETCO2 difference and presumably a significant limitation in forward flow of blood through the pulmonary vasculature, particularly with exercise, secondary to the increase left atrial and pulmonary venous pressures. This not only would further impair pulmonary gas exchange but would blunt the rise in stroke volume and thus the PVCAP'. Accordingly, we theorized that taking into account the stroke volume relative to the pressure should be a good index of the severity of PH in the HF population.
Usefulness of Non-Invasive Gas Exchange
Invasive measures of pulmonary hemodynamics are costly and subject to a number of errors, particularly during exercise. Patient anxiety, large fluctuations in intrathoracic pressures, assumptions related to valvular regurgitation, timing of measures, variation in blood/plasma volume, and, in some cases, use of estimates of cardiac output and/or VO2 can have profound influences on the calculations of PVR.21,22 Moreover, the classic measure of mPpw may also ignore much of the pulmonary circulation (smaller arterioles, capillaries and veins) that may be subject to adverse manifestation with HF progression.23,24 Additionally, resting measures of PV pressures may not be reflective of the hemodynamic pressure response to exercise.
A volume of more recent empirical data, however, has shown that HF is associated derangement of pulmonary gas exchange during submaximal exercise [low PETCO2 and reduced ventilatory efficiency (ie, increased VE/VCO2)] that is likely related to the development and severity of PH.24–27 Furthermore, administration of the pulmonary vasodilator sildena-fil causes a significant reduction in Ppa and PVR with a concomitant decrease in VE/VCO2 slope during exercise (ie, improved breathing efficiency) in HF. 25 Together, these data suggest that the deleterious alterations in pulmonary gas exchange with HF are related to the development of PH in these patients. In addition, our laboratory has demonstrated that the same key pulmonary gas exchange variables (ie, VE/VCO2, PETCO2) are similarly altered in patients with pulmonary arterial hypertension. 15 Given that both HF and pulmonary arterial hypertension have a significant and similar impact on both PETCO2 and VE/VCO2, the ability to detect or estimate the presence of PH in diagnosed HF patients using these gas exchange parameters is likely limited. Thus, we proposed that identification of other simplified metrics to determine the presence and severity of PH secondary to HF may be important.
In the present study, we found that measures of PETCO2 and O2 pulse closely reflect the changes in mPpa (ie, PV pressure) and SV (ie, blood volume), respectively, that occur during exercise in HF patients. Moreover, a unique index of PVCAP using a combination of PETCO2 and O2 pulse (GXCAP) was found to closely relate to an invasively derived measure of pulmonary arterial capacitance during exercise. Importantly, GXCAP along with VE/VCO2 was different between HF patients with and without PH at rest. Accordingly, the novel gas exchange based measure of PV function assessed in the present study may provide a simple metric to estimate the degree of PV derangement in the HF population. Moreover, although further studies are needed, these data suggest that GXCAP may allow differentiation between HF patients with and without PH at rest.
Clinical Implications
Development of the “reactive” form of PH (see Introduction) is associated with a further increase in mortality in the HF population, 7 making it an attractive target for detection and therapeutic intervention. To date, cardiopulmonary gas exchange measures have been used extensively to track disease severity in the HF population. However, the focus clinically has primarily been on maximal measures of oxygen consumption (VO2max). Recently, it has become clear that other gas exchange measures, particularly during submaximal exercise, are more reproducible and may have equal or be of greater prognostic value in the HF population. With simplified commercial gas exchange systems available, shortened, submaximal protocols (eg, 3 min) may be a convenient way to quickly grade severity of disease and track response to therapy. 28 Our current findings identify a novel noninvasive gas exchange based estimate of PVCAP that appears to track the PV response to exercise in the HF population and may also allow differentiation between HF patients with and without PH at rest. To further determine whether GXCAP can be used clinically to assess the progression of PH and the efficacy of therapeutic intervention in this population, further studies must be performed. Of particular interest may be the concurrent effect of pulmonary vasodilator therapy on pulmonary hemodynamics and pulmonary gas exchange indices. If our present observation that key gas exchange variables can track PV responses to exercise, then any reduction in PV pressures and PVR with vasodilator therapy should be matched by changes in key gas exchange variables, including GXCAP'. Such a finding would only strengthen the argument that GXCAP could be used as a clinically based assessment of PH severity, progression, and the response to therapeutic aid.
Limitations
We tested a HF population with relatively severe disease without significant additional co-morbidities (eg, severe chronic obstructive pulmonary disease) and gathered data during moderate supine cycle ergometry exercise. There tends to be large ranges in gas exchange and ventilatory responses to exercise, with the potential for volitional influences. However, we found a strong relationship between an invasive measure of PVCAP and the non-invasive estimate, and both measures appeared to clearly separate HF patients with and without resting PH.
Conclusion
In conclusion, non-invasive exercise gas exchange may represent a relatively simple way of tracking PV changes in HF. GXCAP, an estimate of pulmonary capacitance, appears to be a combination of variables that separate HF patients with and without resting PH.
Author Contributions
Conceived and designed the experiments: BJT, TPO, CK, DM, BDJ. Analyzed the data: BJT, CK. Wrote first draft of the manuscript: BJT, BDJ. Contributed to writing the manuscript: BJT, CK, BDJ. Agree with manuscript results and conclusions: BJT, TPO, CK, DM, BDJ. Jointly developed structure and arguments for paper: BJT, CK, DM, BDJ. Made critical revisions and approved final version: BJT, TPO, CK, DM, BDJ. All authors reviewed and approved the final manuscript.
Funding
This work was supported by grants from NIH (HL71478, HL98663), The American Heart Association (AHA12POST12070084) and Gilead Sciences.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
The authors would like to thank Kathy O'Malley and Minelle Hulsebus for their technical expertise.