
Abstract
Aim
To assess serum Hepatocyte Growth Factor (HGF) levels in individuals with depression and to test the hypothesis that there is a relationship between severity of depression and HGF concentration.
Subjects and methods
Serum from 26 clinically depressed individuals and 19 controls were tested for serum HGF using ELISAs. Correlation was established between HGF concentration and disease severity.
Results
Depressed individuals had significantly lower serum levels of HGF compared to controls (P < 0.0001). HGF concentration correlated with overall depressive behavior (P = 0.03) and specifically depression (P = 0.02), but not anxiety (P = 0.36).
Discussion
These results suggest an association between HGF serum levels and clinically depressed individuals and demonstrate a correlation between severity of depression and HGF levels. Further studies of the predictive strength of HGF as a biomarker for depression may be warranted.
Introduction
Clinical depression is a considerable public health problem. 1 Approximately 32 to 35 million adults in the United States have experienced depression at some point in their life and approximately 13 million adults have experienced depression within the past year. 2 Clinical depression is also a considerable medical problem as those with major depressive disorder (MDD) are at increased risk for serious medical illness, including cardiovascular disease,3–5 diabetes,6–8 cancer,9–11 and stroke. 12
Hepatocyte growth factor (HGF), an 82 kDa, 674 amino acid residue heterodimeric glycoprotein, was originally isolated from rat platelets.13,14 This growth factor has also been called scatter factor, hepatopoietin A, and mammary growth factor. 15 It is one of a small family of factors lacking significant homology with other known growth factors, but including an HGF-like factor known as macrophage stimulating protein (MSP)16–19 HGF has mitogenic, morphogenic, and motogenic effects on hepatocytes, as well as endothelial, mesenchymal and hematopoietic cell types,18,20,21 and demonstrates noticeable species cross-reactivity. 22
HGF regulates cell growth, cell motility, and morphogenesis by activating a tyrosine kinase signaling cascade after binding to the protooncogenic c-Met receptor (translated by the MET gene). HGF is secreted by mesenchymal cells and, although it was first considered to exert biological effects only on specific target cells, it has since been demonstrated to mediate inflammatory responses to tissue injury, and regulate cell growth, cell motility, and morphogenesis in a wide variety of cells. Its ability to stimulate branching morphogenesis, cell migration, survival and proliferation gives it a central role in angiogenesis, tissue regeneration, as well as tumorogenesis.23–29
Signaling by HGF has also been found to have anti-inflammatory, antifibrotic, and pro-regenerative activity on various types of tissue. But it seems to be particularly active in the nervous system, where it has been found to have neurotrophic and angiogenetic activity on CNS neurons, promote both the survival of neurons and the regeneration of injured nerves, and function as a target-derived axonal chemoattractant, guiding axons to their target. As a result, it plays significant roles in the development of the CNS. 30
Because of the potential association between HGF and neurological disease we tested patient with clinical depression for serum concentration of HGF and then compared those levels with severity of disease.
Materials and Methods
ELISA to measure serum HGF (ELISA kit, R&D Systems, Minneapolis, Minn.)
All reagents and specimens were equilibrated to room temperature before the assay was performed. A 1:51 dilution of the patient samples was prepared by mixing 10 μl of the patient's sera with 0.5 ml of Serum Diluent. One hundred microliters of calibrators (20–200 Eu/ml antibodies), positive and Negative control serums, serum diluent alone, and diluted patient samples were added to the appropriate microwells of a microculture plate (each well contained affinity purified polyclonal IgG to HGF). Wells were incubated for 60 minutes (±5 min) at room temperature, then washed 4x with wash buffer. One hundred microliters of pre-diluter anti-human IgG conjugated with HRP was added to all microwells, incubated for 30 minutes (±5 min) at room temperature, then wash 4x with wash buffer. One hundred microliters of enzyme substrate was added to each microwell. After approximately 30 minutes at room temperature, the reaction was stopped by adding 50 μl of 1M sulfuric acid, then the wells were read at 405 nm with an ELISA reader (BioRad Laboratories, Inc., Hercules, CA, USA).
Subjects
Experimental and controls
Serum from individuals with diagnosed clinical depression (n = 26; 12 male; mean age 36.7 years) and controls (n = 18; 5 male; mean age 42.3 years) was obtained from patients presenting at the Health Research Institute/Pfeiffer Treatment Center. Most of these individuals were diagnosed using The Hamilton Rating Scale for Depression before presenting for treatment at the Pfeiffer Treatment Center, Warrenville, Il. *
Patient consent was obtained from all patients involved in this study and this study was approved by the IRB of the Health Research Institute/Pfeiffer Treatment Center.
The Pfeiffer Treatment Center is a comprehensive treatment and research center, specializing in the care of with neurological disorders, including Depression.
Severity of disease
A modified Hamilton Scale was used to determine the severity of depression. Patients were asked to rate their depressive behavior such as; irritability and anger, lack of ability to focus/concentrate, racing thoughts, trouble sleeping, light sensitivity, migraines, OCD behavior, intrusive thoughts, overall anxiety, disorganization, panic, obsessive behavior, and overall depression. The patients were rated on a scale of 0–5 (5 being the highest) for each of these behaviors. We evaluated the overall severity of depressive behavior by establishing the mean of all of the scores for each patient and also compared the overall anxiety and overall depression rating of each patient. The overall severity of depressive behavior assessment includes assessment of all the behaviors (above). The overall anxiety and overall depression rating includes assessment of just anxiety and depression behavior, respectively.
Serum/Plasma
All experimental and control serums were treated in an identical fashion–-frozen at –70C immediately after collection and cell/serum separation, then stored at –70C until thawed for use in ELISAs.
Statistics
Inferential statistics were derived from t-test with 95% confidence intervals. ANOVA analysis was used to do an analysis of variance and multiple comparisons. Pearson Product Moment Correlation and Spearman's Rank Correlation were used for correlation between HGF and severity of disease.
Results
Serum from 26 clinically depressed individuals and 19 controls were tested for serum HGF using ELISAs (described above). Each assay was repeated two or more times, with multiple wells for each serum in each assay.
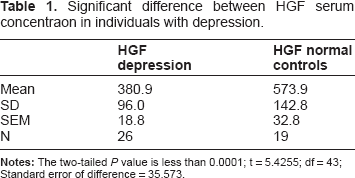
Serum HGF concentration (pg/ml) of individuals with clinical depression (N = 26; Mean SD; HGF=380.9 ± 96) were significantly lower than healthy controls (N = 19; Mean SD; HGF = 573.9 ± 142.8) (P 0.0001) (Table 1).
Significant difference between HGF serum concentraon in individuals with depression.
HGF concentration of individuals with depression was compared to HGF concentration. There was a significant positive correlation between HGF concentration and severity of overall depressive behavior (Pearson correlation 0.48; Spearman's correlation 0.37) (P = 0.03) (Fig. 1) and specific severity of depression (Pearson correlation 0.54; Spearman's correlation 0.49) (P = 0.02) (Fig. 2), but not severity of anxiety (Pearson correlation –0.12; Spearman's correlation 0.08) (P = 0.36) (Fig. 3).

This scatter plot demonstrates a direct relationship between HGF concentration and Overall Severity of Depression (Mean value of depression behaviors) (P = 0.03).

This scatter plot demonstrates the relationship between HGF concentration and Specific Severity of Depression (score of severity of depression for each patient) (P = 0.02).
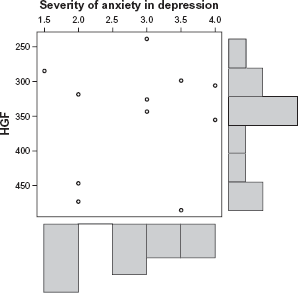
This scatter plot demonstrates that there is no relationship between HGF concentration and Severity of Anxiety (P = 0.36) in this patient group.
Discussion
HGF has been found to be associated with a variety of diseases of the CNS. For instance, immunohistochemistry using anti-HGF antibody has revealed more intense immunolabeling in Alzheimer's disease (AD) than in control brains, and there appears to be a significant correlation between CSF HGF levels and white matter high-signal foci determined on brain magnetic resonance imaging (MRI) in AD patients. 31 In Amyotrophic lateral sclerosis (ALS), overexpression of hepatocyte growth factor (HGF) in the nervous system attenuates motoneuron death and axonal degeneration and prolongs the life span of transgenic mice overexpressing mutated Cu2+/Zn2+ superoxide dismutase. 32 However, overexpression of HGF after gene transfer prevented neuronal death in a Parkinson's Disease rat model. 33 Decreased levels of HGF has been found in autistic children with GI disease. 40
Major depressive disorder has been found to be associated with oxidative stress 34 and oxidative stress levels have been found to correlate with severity of depression. 35 There is also much support for the role of GABA in mood disorders, particularly anxiety and depression. 36
HGF expression has also been found to be associated with oxidative stress markers 38 and receptor gene expression may be suppressed by oxidative stress. 37 HGF has also been found to be associated with GABA regulation, particularly through anxiolytic activity, modulating GABAergic inhibition and seizure susceptibility. 39
This study reports an inversion relationship between serum Hepatocyte Growth Factor (HGF) concentration and severity of depressive symptoms among patients in treatment. Kahl et al 41 measured angiogenic factors in patients with major depressive disorder, comorbid with borderline personality disorder, and did not note a statistically significant relationship between HGF and clinically-established depression. Also, Wakatsuki 42 administered antisense DNA for hepatocyte growth factor to rats, causing a depressive and anxiogenic response. Our results, therefore, represent a novel finding.
Our study shows that depressed individuals have significantly lower levels of HGF than normal controls, and that there is a direct correlation between levels of HGF and severity of depression. We suggest that the low levels of HGF may cause lower GABA, having an anxiogenic effect. This may also help to explain the significant number of depressed individuals who also present with anxiety. To evaluate this relationship, future studies will assess more patients with depression and evaluate GABA levels along with HGF concentration.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material.