
Abstract
This review discusses biomarkers that are being researched for their usefulness to phenotype chronic inflammatory lung diseases that cause remodeling of the lung's architecture. The review focuses on asthma, chronic obstructive pulmonary disease (COPD), and pulmonary hypertension. Biomarkers of environmental exposure and specific classes of biomarkers (noncoding RNA, metabolism, vitamin, coagulation, and microbiome related) are also discussed. Examples of biomarkers that are in clinical use, biomarkers that are under development, and biomarkers that are still in the research phase are discussed. We chose to present examples of the research in biomarker development by diseases, because asthma, COPD, and pulmonary hypertension are distinct entities, although they clearly share processes of inflammation and remodeling.
Keywords
Introduction
Breathlessness, fatigue, insomnia, and cough are some of the signs of many chronic lung diseases. Together these symptoms lead to decreased quality of life. Some of these chronic lung diseases end in early mortality. Therefore, early detection, good prognostic measures, and personalized management of these diseases are highly desired.
Many chronic lung diseases, such as chronic obstructive pulmonary disease (COPD), develop insidiously over many years and can remain undetected until large areas of the lungs are remodeled and have lost their structure.1,2 Others, such as asthma, can be detected early on in childhood, but it is difficult to predict if the condition is going to resolve, persist, resolve and reappear, or persist in a progressively worsening clinical trajectory. 3 Still other conditions such as pulmonary hypertension are a challenge to correctly diagnose, because the breathlessness can be mistaken for a problem of airway function, instead of recognizing the increase in the pulmonary blood pressure.4,5
To date, most of the markers used for phenotyping in clinical use are either based on lung function, right heart function measurements, and imaging – particularly high-resolution X-ray computed tomography (CT) scans – or cellular analysis of bronchoalveolar lavage or sputum specimens (Table 1).6–16 Molecular markers (Table 2),17–45 while still limited, are being developed to facilitate detection of injury to cells within the lung structure and to identify molecular disease mechanisms in order to personally tailor therapeutic management. Additionally, biomarkers of disease risk and biomarkers that predict disease progression are being developed. The following sections discuss specific chronic conditions of the lungs with respect to the application of these different types of biomarkers.
Examples of phenotyping procedures for asthma, COPD, or pulmonary hypertension.

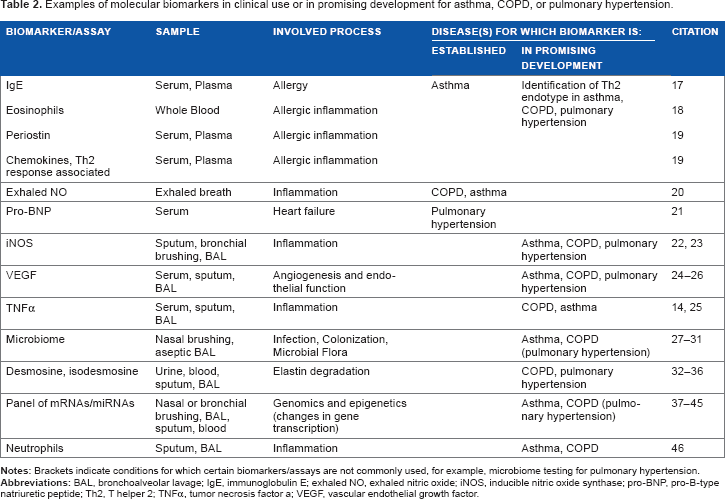
Examples of molecular biomarkers in clinical use or in promising development for asthma, COPD, or pulmonary hypertension.
Biomarkers for Asthma
Asthma affects approximately 300 million people worldwide (GINA guidelines 2015 6 ). Asthma is a heterogeneous disease with a diagnosis dependent on the confluence of symptoms and measurements of lung function showing variable airflow obstruction or airway hyperreactivity. Although the bronchi are the structures mainly affected in asthma, changes in small airways, bronchial blood vessels, and pulmonary blood vessels can also be present. Several biomarkers that characterize some of the phenotypes of asthma have included blood or sputum eosinophils, serum/plasma immunoglobulin E (IgE), and exhaled nitric oxide (NO). 20 An increase in the peripheral total IgE titer suggests the presence of an allergic response9,47; the allergic response can be further dissected by determining allergen-specific IgE or allergen-specific skin reactivity.
The challenge
The challenge is that asthma is heterogeneous and not all asthmatics are atopic (ie, have allergen-specific IgE). Moreover, some asthmatics fail to achieve control even with the use of high-dose therapy of broncho-dilators and inhaled corticosteroids.17,48 Additionally, current therapy is based on reducing symptoms and not curative; the symptoms of asthma return when the therapy is stopped. 17 The result is that bronchodilators and inhaled corticosteroids are often required for lifelong therapy, and these have the potential for significant side effects. Thus, new drugs are needed to modify pathways that are present in the different manifestations of asthma and that might reduce the need to use chronic corticosteroids.
Drugs that target specific inflammatory pathways have been sought after for years. The first leukotriene antagonists inhibited synthesis or receptors of the leukotriene pathways; however, they were incompletely effective and raised the possibility that there were subsets of patients who might respond better than others. 49 New examples include anti-IgE (first Food and Drug Administration [FDA] approval 2003),52–53 drugs that target interleukin (IL)-4 or IL-13 or both (in phase III clinical trials and in development),54–58 anti-IL-5 (awaiting FDA approval in 2015),18,59–64 and anti-IL-17 receptor (clinical trial for asthma stopped 65 ). Furthermore, it is increasingly clear that the different phenotypes of asthma may be associated with different endotypes, or biologic pathways, for example, T helper (T)2, T17, high eosinophils, or high IgE. 66 Because the specific drugs target the critical process that causes asthma in the particular patient, the therapy has to be personalized by matching the pathogenic mechanism and the specific therapy. 67 Thus, it is necessary to develop a biomarker or a set of biomarkers (biomarker profile) that characterizes the underlying disease pathways together with the new therapeutics. Because the process-specific therapies target the critical mediator, it is possible that there may be curative effects that provide long-term relief from the asthma symptoms. However, for anti-IL-5 therapy, this expectation was not met because asthma exacerbations and eosinophils returned when the therapy was withdrawn. 60
Biomarkers under development
These are examples of process-specific biomarkers that are under development (Table 2)68–71:
Total plasma/serum IgE levels or the presence of perennial allergen-specific IgE levels provide a cutoff value for use of anti-IgE therapy.
17
Numbers of eosinophils in the blood provide a marker value for the high-eosinophil asthma phenotype for which anti-IL-5 therapy is effective.
18
Serum/plasma periostin levels combined with numbers of blood eosinophils and additional biomarkers (eg, plasma eotaxin or IgE) are indicators of patients who respond to therapy with anti-IL-13.
19
In some instances, this profile is referred to as T helper 2 – high (T2-high) asthma. The concept of the T2-high asthma is challenging because therapies with anti-IgE, anti-IL-5, or anti-IL-13/IL-4 in asthma are designed for the T helper 2-high endotype. However, in studies involving T2-high mouse models (characterized by eosinophils and IgE), airway hyperreactivity and increased airway mucus were inhibited by anti-IL-1372,73 and not by IgE deficiency
74
or anti-IL-5
74
treatment. Therefore, the biomarker panel for the therapies with anti-IL-13, anti-IL-4, and anti-IL-13 + anti-IL-4 (or anti-IL-4 receptor α) is still in development19,57,58 and is expected to be of great significance for personalized asthma management. Sputum-derived molecular signatures of dendritic cells and airway epithelial cells are developed to more specifically understand the type of the immune response and the degree of inflammation.
46
This knowledge is expected to be of great value for assessing the progression of asthma and the response to therapy. Biomarkers of critical changes in glucose and lipid metabolism and oxidative stress are also being developed to specifically identify the mechanism that causes non-allergic asthma and asthma that is unresponsive to the therapeutic options detailed above.27,75–78
The challenge for biomarker-guided therapy and for biomarker-guided assessment of progression and/or response to therapy is the ability to measure these biomarkers in relatively accessible samples, ie, sputum biomarkers are usually only performed in research centers, whereas blood biomarkers are more easily accessible. An additional level of complexity that is introduced into the clinical algorithm is that the use of these markers makes diagnosis and monitoring of responses to therapy more expensive. The therapeutic dilemma for asthma patients whose biomarker profile does not fit an available specific therapeutic option is challenging. For these cases, bronchodilators and inhaled corticosteroids remain the therapeutic approach of choice, with antimuscarinic agents added when these fail, and few other options. This dilemma is not uncommon as approximately half of the patients who have severe asthma that is not controlled with bronchodilators and inhaled corticosteroids posses a biomarker profile that is not clearly understood,48,79 and no specific, biomarker-guided therapy is yet available.80,81
In conclusion, new asthma biomarkers are under development to better match the disease process with specific therapies. Several challenges remain to be tackled, among them are added costs and the clinical dilemma of patients presented with uncontrolled asthma and a biomarker profile that does not match available new therapies. The combination of specific biomarkers and new therapies is expected to achieve better asthma control with fewer side effects and perhaps long-lasting therapeutic success.
Asthma COPD Overlap Syndrome
Recent deep phenotyping and biomarker studies have identified asthma/COPD patients who also had a profile suggesting allergic inflammation (Th2-associated inflammation)/remodeling changes indicative of COPD, a condition known as “Asthma COPD overlap syndrome.”82–91 The existence of a syndrome where asthma and COPD overlap was predicted by studies in experimental animals.92–94 Biomarkers will be necessary to further subtype patients who show signs of this clinical overlap syndrome. For example, specific biomarkers of a Th2 response may identify individuals who might profit from therapy with IL-13/IL-4 inhibitors. Biomarker panels covering both inflammatory and remodeling markers would be particularly informative to determine personalized therapy in these individuals. Specific biomarkers and clinical characteristics need to be further defined by future research. 95
Development of Biomarkers for COPD
COPD is the third most common cause of death in the world. 96 COPD is characterized by progressive airflow limitation 97 that is not reversible by bronchodilator drugs. In addition to lung function measurements, imaging (eg, high-resolution CT), bronchoscopy, sputum, and exhaled breath (exhaled NO) 20 are used to assess the nature and the degree of tissue damage to the lungs. A major cause of COPD is exposure to cigarette smoke (primary exposure or indirect exposure via secondhand smoke) although exposure to biomass smoke is a major contributor worldwide. 98 Nearly the whole structure of the lungs is affected, including bronchi, small airways, alveoli, blood vessels, and connective tissue. The lung structures can show signs of destruction, leading to a loss of alveoli and subsequent emphysema or scarring and remodeling of the small airways. 99 Furthermore, the changes within the tissue from COPD can be a precursor to lung cancer.100–103
Measurement of lung function alone presents limitations to determine prognosis, predicting outcomes, selecting appropriate therapy, or monitoring disease activity. Thus, a biomarker that has the potential to identify exacerbations and provides prognostic information on the severity of the disease has long been sought.
Inflammation
C-reactive protein (CRP) was the first biomarker to be investigated in COPD,104–107 and most studies have shown that CRP levels are elevated in COPD patients, both nonsmokers and smokers without airflow obstruction when compared with controls. However, CRP levels are a marker of inflammation and because inflammation is one of the constant processes in COPD, it does not distinguish disease processes or understanding of the specific structure that is being affected in a patient with COPD.
A panel of six inflammatory markers in peripheral blood (white blood cell count, fibrinogen, CRP, IL-6, IL-8, and tumor necrosis factor [TNF]-α) in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study predicted increased mortality and exacerbation rates in COPD patients with inflammation when compared with patients without inflammation. 108
The chemokine cc-chemokine ligand-CCL18 may also be a component of the serum biomarker signature of inflammation in COPD. CCL18 concentrations were independently associated with the presence of COPD; its concentrations were independently associated with the future risk of cardiovascular hospitalization and mortality and with total mortality in COPD. Lastly, an intervention study showed that short-term steroid use modified serum CCL18 levels. 109
Sputum neutrophil count has been used as a biomarker to evaluate responses to COPD therapies. The advantage of this biomarker is that it is measured locally in the sputum and reflects inflammation in the airways. There is a clear association of increased sputum neutrophils with smoking and COPD progression. 110 The increased neutrophil numbers persisted for at least 1 year, even following smoking cessation, when measured in the sputum 111 or in biopsy 112 specimens.
Vascular changes
Pulmonary vascular changes are an integral component of COPD. 22 The vascular abnormalities can present as pulmonary hypertension associated with COPD. 113 Accordingly, biomarkers that determine endothelial cell function are associated with COPD. One example is inducible NO synthase that produces NO and contributes to oxidative and nitrosative stress in COPD. 22 Another biomarker example is vascular endothelial growth factor (VEGF). A significant difference in plasma VEGF levels between healthy control and COPD patients and correlation between plasma VEGF and FEV1 (forced expiratory volume in 1 second) was shown. 114 Similarly, a decrease in sputum VEGF was correlated with COPD severity. 115 Animal model studies have clearly established that inhibition of VEGF can cause emphysema116,117 and prepares the vascular bed for remodeling in response to a second stressor (eg, combination of VEGF blockade and hypoxia 24 ). As part of a larger panel, biomarkers of endothelial cell function are expected to be a valuable means to determine disease status.
Systemic organ involvement
COPD is a systemic disease associated with skeletal muscle wasting.118,119 Serum levels of chemokines (cx-chemokine ligand-CXCL9, CXCL10) were correlated with energy metabolism genes in skeletal muscles of COPD patients. 120 CT imaging of skeletal muscle mass shows promise as a marker of COPD severity and for the identification of gender-specific differences in COPD.121,122 Serum myostatin123,124 and serum creatinine 125 are also under investigation as biomarker of skeletal muscle function in COPD. High levels of serum creatinine are seen following acute muscle destruction while abnormally low levels indicate skeletal muscle atrophy. 125 Serum creatinine in addition to other kidney function markers is also an indicator of renal disease in COPD. 126 Circulating microRNA (miRNA) species are discussed in more detail under emerging biomarkers and are being considered as markers of muscle wasting in COPD. 39
Oxidative and nitrosative stress
A continuum of oxidative stress in virtually all cells in the lungs is thought to be another major pathogenic event in COPD.22,127–130 Oxidative (and nitrosative) stress is chemically characterized by the exposure to exogenous or endogenous radicals of oxygen or nitrogen. In addition to proinflammatory signals, the radicals are highly reactive and modify proteins and nucleic acids. The modified (eg, nitrosylated) proteins can lose proper function and therefore cause critical cell damage. 22 These processes are thought to be the basis for remodeling changes in the pulmonary blood vessels of COPD patients, which in turn causes COPD-associated pulmonary hypertension. 22 Biomarkers that would precisely reflect the source of the free radical – for example, oxidants in cigarette smoke, increased activity of inducible NO synthase, or decreased expression of antioxidant proteins that are in turn controlled by nuclear factor (erythroid-derived 2)-like 2 (NFE2 L2-NRF2) – could lead to the development of specific therapies.22,131 Therapy with nonspecific antioxidants has been evaluated in COPD. These have failed perhaps due to the inability to precisely and sufficiently target the root process that is causing the oxidative or nitrosative stress. 132
Assessment of structural cell and stromal function
Biomarkers that assess the function of lung cells in COPD 133 include club (Clara) cell secretory protein (CCSP, CC-16 134 ) and surfactant protein D (SP-D135,136). CCSP is produced almost exclusively by nonciliated, secretory club cells (formerly Clara cells).137–139 Club cells are transitional precursor cells for ciliated airway epithelial cells,140,141 and type II epithelial cells lining the alveoli produce surfactant proteins. 142 Serum CCSP levels were measured in 2083 patients with COPD (ECLIPSE cohort). 143 Serum CCSP levels were reduced in patients with COPD, and there was a correlation with disease severity in former smokers. 143 In the ECLIPSE cohort study, SP-D was higher in current than in former smoker controls but was significantly higher in both current and former smokers diagnosed with COPD. 144 There was a rapid and marked fall in serum SP-D levels among COPD patients who received oral corticosteroids. Its levels returned to baseline following the cessation of treatment, 144 but the risk of exacerbations increased with increasing baseline serum SP-D levels.144–146 However, after acute exposure to cigarette smoke, CCSP serum levels have been shown to be increased 147 or suppressed 148 by inhaled corticosteroids.
Unchecked and increased protease activity causes tissue destruction and emphysema in COPD.149–153 In addition to the destruction of the alveolar wall, the composition of the lung's matrix is also significantly altered in COPD. Sand et al. 154 found significantly elevated levels of circulating biomarkers of collagen types III, IV, and VI and elastin at the time of COPD exacerbation when compared with that during follow-up. The tissue turnover balance, assessed systemically by the collagen degradation/formation ratio, increased for type III and VI collagen and decreased for type IV collagen.
Desmosine and isodesmosine are small degradation peptides of elastin and can be measured by mass spectrometry in the plasma and urine. Associations between desmosines and several lung function variables suggest that desmosines, particularly those measured in urine, may be a useful biomarker of ongoing lung destruction in COPD.32,35,36,155–157
Alpha-1 antitrypsin is a major endogenous inhibitor of serine proteases such as neutrophil elastase and has therapeutic application in COPD with focus on emphysematous changes 158 because cigarette smoking induces functional deficiency of this inhibitor in the lungs. 159 Individuals who have a loss-of-function mutation in the α1 antitrypsin have increased risk of developing emphysema.160,161 Plasma desmosine values did not significantly change following therapy with α1 antitrypsin in deficient individuals, 162 perhaps indicating that the α1 antitrypsin did not fully inhibit the excess protease activity in this initial study. Later studies showed a significant effect of α1 antitrypsin replacement therapy in lowering desmosine and isodesmosine levels in plasma and bronchoalveolar lavage fluid. 163 These data again suggested the utility of desmosine and isodesmosine as biomarkers of matrix turnover in the lungs.36,157,164,165
In addition to the serine proteases, metalloproteinases (MMPs) also have major destructive activity in COPD.151,152 Both metalloelastases 166 and metallocollagenases 151 contribute to the process. The proteolytic activity of MMPs is inhibited by tissue inhibitors of metalloproteinases (TIMPs). Concentrations of MMPs and TIMPs in the serum or sputum, as well as the molar ratio between MMPs and TIMPs, are currently being evaluated for their use as a marker of COPD severity, predictors of COPD exacerbations, with specific focus on emphysematous changes.167–170
Protease inhibitors with broad-spectrum activity have therapeutic potential in COPD. However, the challenge is that matrix protein turnover is critical for lung health and requires proteases at optimal activity levels. Biomarkers of matrix turnover and therapies that would normalize matrix could greatly aid the management of COPD and also all diseases that cause lung fibrosis.
Progression of COPD from the inflammatory and remodeling condition to lung cancer
Large-scale proteomic profiling has revealed a biomarker panel that is hoped to aid in the detection of the emergence of lung cancer in the continuum of changes in the cells from the lungs of COPD patients.100,101,103 Proteomic and genomic profiling of epithelial cells obtained from buccal or nasal swabs showed that molecular programming of these cells reflected changes in airway epithelial cells, 102 further emphasizing inhaled exposures to toxic substances as a cause of COPD. 38 The search for biomarkers that will identify endotypes of COPD is still under intense investigation and is expected to significantly improve the management of this disease.86,171–174 It is to be emphasized that in all studies a multimolecular signature was necessary to cluster the patients who had COPD and cancer. The signature comprised, for example, five diagnostic and six normalization proteins in plasma samples, 103 59 genes in the airway transcriptome, 102 or 13 proteins in the blood. 101 These data suggest that a biomarker test that is useful for cancer diagnosis in COPD patients will be multimolecular and can be performed in blood 101 /plasma 103 samples and in nasal and buccal epithelial samples. 102 This latter property is important because it suggests that the multimolecular biomarker test can be performed on samples that can be acquired noninvasively.
Biomarkers for Pulmonary Hypertension
Pulmonary hypertension has multiple etiologies. It can be considered a stand-alone condition (eg, idiopathic, heritable, or high-intensity exercise-induced pulmonary hypertension) or as an exacerbating change in obstructive sleep apnea and many lung, heart, blood, and autoimmune diseases. 175 The diagnosis of pulmonary hypertension can predict a short survival rate (eg, 15% mortality rate over 1- to 2-year period for heritable pulmonary hypertension and even higher mortality rate for systemic sclerosis-associated pulmonary hypertension). 175 Pulmonary hypertension can occur alone or in association with many different diseases, and it is classified into five groups by World Health Organization (WHO). The available drugs are targeted for specific WHO groups. 175
Pulmonary hypertension is characterized by remodeling in the pulmonary vascular bed and can affect the pulmonary artery or vein. Functional measures of right heart function, pulmonary artery pressure, imaging of the right heart (Table 1), and a circulating biomarker of cardiomyocytes 176 (N-terminal pro-B-type natriuretic peptide, pro-BNP; Table 2) are in clinical use for pulmonary hypertension. Furthermore, mutations in several genes, most importantly in the bone morphogenetic protein receptor type 2 (BMPR2) gene,177–180 increase the risk of developing pulmonary hypertension significantly. The identification of these mutations by a genetic screening test is being used to aid carriers of the mutated genes with additional monitoring.
Current studies are under way to identify additional biomarkers that would help to better match pulmonary hypertension to optimal therapies and to better understand disease pathogenesis. 181 For example, pulmonary hypertension in association with COPD can be the result of diffuse changes in the lung's structure, affecting the airspaces and the vasculature, and in that case, patients would benefit from targeted pulmonary vasodilator therapies. 114 In this situation, the exposure to toxic substances, eg, cigarette smoke, could have a primary impact on the pulmonary vasculature and the associated lung structure and less impact on inflammation. 22 Conversely, pulmonary hypertension in association with COPD can also be the result of focal tissue remodeling of the airways, alveoli, and blood vessels caused by foci of inflammation or foci of oxidative/nitrosative stress. 114 In that case, vasoconstriction is function-preserving because it restricts blood flow to the remodeled, nonfunctional areas of the lungs and instead directs blood to areas of the lungs that are less remodeled and still have gas-exchange activity. Therefore, administration of vasodilators would not be helpful and could worsen the condition. 113
Desmosine and isodesmosine, two amino acids that form cross-linkages in elastin, are also being evaluated as biomarkers of matrix turnover in pulmonary vascular remodeling. 182 This is hoped to detect the abnormal elastin and collagen content and turnover that is a critical process in the remodeling of the vascular bed in pulmonary hypertension.183–188
Pulmonary hypertension can be associated with autoimmune diseases that manifest in generalized connective tissue remodeling (eg, systemic sclerosis). In some of these cases, specific immune dysfunction can induce pulmonary hypertension, and specific biomarkers are being sought that would match patients with specific immune inhibitors (eg, anti-IL-1, 189 anti-IL-6, 189 anti-IL-13/IL-4,190,191 anti-IL-17, 192 or interferon 190 ). Animal model studies suggest that the immune mediators have a causal relationship with vascular remodeling and increased right ventricular pressures.193–198 Therefore, the expectation is that specific biomarkers of the immune processes will be important guides for personalized therapy in pulmonary hypertension associated with significant inflammation.
Several large multicenter clinical trials (eg, Pulmonary Vascular Disease OMICS (PVDOMICS)) are currently under way to identify additional biomarker candidates in a variety of types of pulmonary hypertension, including those with underlying parenchymal lung disease.
Biomarkers of Environmental Exposures
Environmental exposures exacerbate all chronic lung diseases by inducing oxidative stress or inflammation, directly injuring the cells that line the airspaces, and causing associated damage to the cardiovascular system and increased mortality.199–201 Techniques to measure fine dusts and volatile chemicals such as ozone in air are well established.202,203 Tracers are available that track the source of the fine dusts and distinguish between fossil fuel 204 and biomass (plant) combustion205–208 or identify fungal products in indoor air. 209
Additionally, there are several examples of drugs that can cause chronic lung disease or exacerbate an existing condition 210 : aspirin 211 or angiotensin-converting enzyme inhibitors 212 can cause asthma; fenfluramine/phentermine (a weight loss drug) can cause pulmonary hypertension 213 ; fenretinide (a cancer drug) can cause emphysema 214 ; bleomycin (a cancer drug) 215 can cause parenchymal inflammation and interstitial fibrosis; and kinase inhibitor cancer drugs 175 can cause pulmonary hypertension. Naturally occurring toxins have also been linked to chronic lung disease, for example, molds in water-damaged houses 209 and asthma/COPD or monocrotaline (from many types of plants) 216 and pulmonary hypertension. In all these cases, the relationship between the natural or drug toxicity and the chronic lung disease could be causally resolved by combining studies in human subjects and animal models.
Biomarkers that would quantify environmental exposures of the lungs and establish an etiology of exposure for the chronic lung disease are much less established. Causality of exposure is established for silica/coal dust exposure causing bronchitis and pulmonary hypertension,217,218 as is cigarette smoke exposure and COPD. 98 Cotinine is a specific and sensitive serum marker for cigarette smoke exposure and in large epidemiologic studies shows the detrimental effects of exposure to secondhand cigarette smoke.219,220 However, more specific chemicals need to be measured to determine the individual exposure to specific toxins in tobacco smoke. 221 Levels of IgE antibodies or asthma exacerbations to indoor or outdoor allergens are an indirect measure of exposure because responses occur in at-risk or in sensitized individuals.222,223 For example, high IgE levels may be produced by exposure to large doses of allergen or low doses of allergen in a highly sensitized individual. Direct detection of particles in induced sputum224–228 or bronchoalveolar lavage 229 is possible when the exposure levels are very high (as occurred during the World Trade Center disaster) or is the result of occupational exposures. However, these measures lack specific quantification. Current research efforts are directed toward the identification of biomarkers that predict increased risk of developing chronic lung diseases and other detrimental health effects due to occupational, residential, or outdoor ambient exposures.230–235 The tests under development are not yet specific for the exposure but indicate protective or injurious metabolic, inflammatory, or tissue remodeling activities. Environmental disasters such as the World Trade Center collapse are being used to identify biomarkers that would detect individuals at risk for the development of chronic progressive lung disease in response to the exposures.236–239
Emerging Classes of Biomarkers
Gene and protein expression has been the paradigm for biomarker studies, and these classes of biomarkers, particularly messenger RNA (mRNA) measured by polymerase chain reaction or proteins determined by enzyme-linked immunosorbent assay (ELISA or multiplex ELISA) or proteins determined by mass spectrometry assays, have been used for the biomarkers that are currently in clinical development. New classes of biological molecules are emerging as potential sources of valuable biomarker information as outlined below.
Noncoding RNA
Noncoding RNA species are being evaluated for their utility in many different disease processes, including all types of chronic lung diseases. One class of non-coding RNA, miRNA, serves not only for communication between adjacent cells but also between cells from different organs. miRNA is packaged in exosomes or adheres to carrier proteins and then exported into the blood and to other extracellular spaces. Therefore, levels of specific miRNAs can be determined in serum, plasma, and exosomal fractions of plasma, serum, sputum, or bronchoalveolar lavage.41,42 Specific miRNAs are being investigated for their role in disease pathogenesis and also as potential biomarker in all chronic lung diseases, including asthma,43,45,240–244 COPD,37,40,245,246 muscle wasting in COPD,39,123,247 and pulmonary hypertension.248–256 Although there is great enthusiasm, currently none of the miRNA species has been established as a clinical biomarker for chronic lung diseases.
Metabolites
Biomarkers that detect molecular changes in metabolism are also emerging as important contributors to virtually all chronic lung diseases. For example, major adipokines leptin and adiponectin were reported to be abnormally regulated in COPD and related to systemic inflammation, body mass index (BMI), and gender. 257 Resistin, another adipokine, is under investigation as a biomarker in asthma. 258 Furthermore, many cases of severe treatment-refractory asthma and cases of pulmonary hypertension are thought to be associated with severe reprogramming of metabolism and high BMI.259–261 Mutations in the bone morphogenetic protein receptor 2 gene that increase the risk of developing pulmonary hypertension are now thought to cause reprogramming of cardiac lipid storage and glucose metabolism.262,263
Biomarkers of metabolic remodeling in the pulmonary vasculature and right heart are expected to be of diagnostic and prognostic value in pulmonary hypertension.264–268 Lower circulating levels of the soluble receptor for advanced glycation end products (RAGE) were associated with the severity of COPD, specifically emphysema, and a genetic polymorphisms in the RAGE gene locus. 269 Lower RAGE levels were also associated with neutrophilic asthma. 270 However, animal models suggest that the role of RAGE in asthma requires further studies because in the model the presence of RAGE is critically required for the asthmatic response to natural allergens. 271
Vitamins
Vitamins have been widely studied for their contribution to chronic lung diseases, and vitamin levels can be used to determine increased risk for developing disease. In the ECLIPSE study, low levels of vitamin D in blood – reflecting insufficient nutritional intake and insufficient exposure to sunlight – were related to the presence of emphysema, exercise capacity, airways reactivity, and blood CCSP levels. 272 Abnormally low circulating levels of vitamin D have been related to exacerbations of asthma and asthma susceptibility. 273 However, vitamin D as an add-on therapy for asthma has shown inconsistent results,274,275 suggesting that an optimal level of vitamin D may be required.
Coagulation markers
Coagulation markers have long been implicated in chronic lung diseases. Serum von Willebrand factor, a glycoprotein that is a marker of endothelial cells and initiates coagulation, has been reported to indicate early structural and functional changes of the pulmonary vasculature and to be an interesting marker for COPD. 276 Inflammation in the lungs causes another coagulation cascade initiation protease, tissue factor activity to be expressed and to be released via exosomes from mononuclear cells, airway epithelial cells, and endothelial cells.277,278 By this mechanism, tissue factor causes increased coagulation due to inflammation or tissue injury, including asthma.279–281 Abnormally increased or decreased coagulation leading to pulmonary intravascular thrombosis or contributing to pulmonary hemorrhage can be seen in pulmonary hypertension.282–285
Microbiome
Markers to distinguish an intact microbiome from a microbiome that protects, predisposes, or causes disease are being refined in ongoing research.31,286–288 The most frequently used methodology consists of deep sequencing of 16S ribosomal (r)RNA of bacteria.289,290 Additionally, sequencing methods to study the fungal and viral microbiomes and metabolic state of a specific microbiome are in development as tool for the understanding of chronic lung diseases.28,291 The sequencing approach circumvents the necessity to culture bacteria, virus, or fungi and allows for detection of microbes that cannot be cultured. Furthermore, sequencing allows the vastness of the microbiome to be appreciated. Changes in the microbiome of the lungs in COPD are currently being mapped out to understand the recurrent microbial infections that cause hospitalizations and exacerbations of COPD.29,30,291,292 Viral infections, including rhinovirus 293 and respiratory syncytial virus, 294 are thought to initiate asthma in early life and are major triggers of exacerbations in asthma patients of all ages.295,296 Furthermore, when compared with controls, patients with uncontrolled asthma had a higher microbiota burden in the airways. 297
Conclusions
The lungs are catching up with many other organs for the availability of molecular biomarkers that would indicate molecular disease processes or detect injury to specific cell types in the lungs. The readily available specific lung and right heart function tests may have slowed the discovery of molecular biomarkers. In addition to lung and right heart function tests, imaging was also developed early, with bronchoscopy providing for direct inspection of airways and the ability to obtain biopsies of lung and lung-draining lymph node tissue under visual guidance. 298 Furthermore, high-resolution CT, positron emission tomography, and magnetic resonance imaging scans are allowing for detailed imaging of lungs and heart.299–303 The disadvantages of the above tests include the specialized equipment, the invasiveness of some of the procedures (bronchoscopy, right heart catheterization), and the time required and the potential for radiation exposure by the imaging procedure.304–306
New therapies that are specific to a molecular pathway are still in clinical trials or have been approved during the past 10 years, eg, anti-IgE or anti-IL-13/anti-IL-4 for asthma. These new therapies have provided demand to identify molecular biomarkers so that therapies can be personalized for the disease driving molecular process.19,57,62,307,308 Improved therapies and management of a deadly condition, pulmonary hypertension, have led to improved quality of life and increased life expectancy. 309 This clinical success in pulmonary hypertension has created demand for the development of molecular biomarkers for early detection and better matching of aberrant disease-causing molecular process and therapy.21,113,310 Improved detailed imaging of lungs of COPD patients has resulted in the detection of early changes in the lung structure, 311 and there is a great demand for prognostic biomarkers.101,103,173,174
For these reasons, it is expected that in the future molecular biomarkers will become critically important tools for the clinical management of many of the chronic lung diseases.
Author Contributions
Idea for the review: GG. Writing of the manuscript: GG, ND. Preparation of the tables: GG, AB. Finding of references: GG, ND, AB, JR. Editing: GG, AB, S-HP, SP, BB, JR, EB-R, ND. All authors reviewed and approved of the final manuscript.