
Abstract
Introduction
The variable number of tandem repeats (VNTR) of the dopamine receptor D4 (DRD4) gene among humans may elucidate individual differences in susceptibility to neuropsychiatric diseases. Dopamine dysfunction may be involved with Attention Deficit Hyperactivity Disorder (ADHD) symptoms. In this study, we report the association between the phenotype of ADHD, a condition characterized by inattentiveness, hyperactivity, and impulsiveness, and a 48–base pair VNTR in exon 3 of the DRD4 polymorphism.
Subjects and Methods
We used a case control approach conducted on 29 ADHD and 31 ethnically matched control Egyptian children (ages 6–12 years). Cases were assessed by a psychiatric semi–structured interview and the Conners’ Parent Rating Scale. VNTR polymorphisms of the DRD4 gene were done by touchdown PCR program using exon 3–specific primers followed by agarose gel electrophoresis.
Results
We observed a significant association between the existence of D4.4 allele of DRD4 and ADHD (P < 0.002); 6.9% of cases showed a single D4.4 and 10.3% showed a double D4.4 as compared to controls in whom D4.4 has never been detected.
Conclusion
Children with smaller number of repeat alleles (two to four repeats) of the DRD4 gene have higher possibility to develop ADHD in Egyptian children.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a heterogeneous neuro behavioral disorder with multiple possible causes. Genetic and environmental factors lead to neural pathway alterations and subsequent ADHD. 1 Children with ADHD suffer from inattention, hyperactivity, and impulsivity. 2 It was estimated that 50% of children with ADHD develop symptoms in Childhood that may persist until adolescence. 3 It was estimated that more than half of the ADHD children showed comorbidity with at least one other psychiatric disorder. Children with ADHD may exhibit autistic traits. It was found that 20% to 50% of children with ADHD showed criteria for autism. 4 The twin, family, and linkage studies showed an evidence of genetic overlap between the two disorders. Few studies have been done to determine the specific genetic polymorphisms that can induce both types of symptoms.
It was observed that the neurotransmitters dopamine and norepinephrine were involved in neuronal activity as well as the maintenance of attention and alertness.5,6 It is mandatory to identify genetic markers for ADHD in order to improve the diagnostic process and in turn lead to better management. The knockout gene study in mice showed an alteration of dopamine metabolism in ADHD. 7 Several genes have been implicated in ADHD such as DAT1, DRD1, DRD2, DRD3, and DRD4. 8
Dopamine receptor D4 is the most studied receptor gene in association with ADHD. 9 Te DRD4 receptor is expressed in multiple brain regions and these brain regions are thought to be involved in the etiology of ADHD.10,11 This receptor gene is mapped to chromosome 11p15.5. 12 It contains quite a large number of polymorphisms in its nucleotide sequence. The 48-bp variable number of tandem repeat (VNTR) in exon 3 is the most studied polymorphism to investigate the association with ADHD. This region couples to G proteins and modulates the cAMP production. 13 The length of exon 3 varies from 2916 amino acids to 11916 amino acids, in which the 48–bp sequence exists as a 2– to 11–fold VNTR, denoted as D4.2 to D4.11. 14 Quite a few studies divided these repeat alleles into two categories: short repeat (two to four) alleles and long repeat (five to eight) alleles. 15 Meta analysis studies have shown significant associations of ADHD with DRD4.16,17 The worldwide prevalence of ADHD ranges from 2.2% to 17.8%. 18 A more valuable prevalence estimate is that based on the prevalence of children suffering from symptoms of ADHD at the clinical levels using validated ADHD rating scales, such as the Conner's Scale. The identification of ADHD has been shown to vary across geographical regions, and by ethnicity and gender 19 ; however, Holden et al. 20 pointed out that this could be due to differences in the diagnostic criteria. It was reported in Egypt that ADHD– inattentive type constituted 39% of the finally diagnosed cases. 21 The detection of the genetic factors for children with ADHD in the Egyptian population becomes imperative. In this study, we examined the distribution of different VNTR alleles of DRD4 exon 3 in children suffering from ADHD.
Subjects and Methods
I–Study subjects
This study was conducted on a sample of 60 children recruited from the Child Psychiatry Clinic, Abul Reesh, Kasr el Eini Hospital. Twenty nine (29) of these children were diagnosed with ADHD, according to DSM–IV–TR criteria and Conners’ Parent Rating Scale (CPRS–R). 22 The inclusion criteria included both sexes and ages 6 to 12. The exclusion criteria was the co–morbidity of oppositional defiant disorders, conduct disorders, anxiety and depressive disorders. The control group consisted of 31 age, sex and socioeconomic status matched children. They were free from any psychiatric disorders, developmental disorders, or chronic medical conditions. Complete clinical and psychiatric examinations including, parental age, and degree of consanguinity were done for all studied subjects. Autistic symptoms were detected using the social responsiveness scale (SRS).
For participation in the study, informed verbal and written consents were obtained from cases, controls and their parents/guardians. The study protocol was approved by Institutional Ethical Committees of the National Research Center and Faculty of Medicine, Cairo University. The study followed the principles of the Helsinki declaration.
Genotyping of DRD4 gene
Whole blood samples were taken at Cairo University, which owns the samples. Genomic DNA was isolated from the whole blood samples using QIA amp DNA blood mini kit according to the manufacturer's protocol. Purity and quality of DNA were determined by spectrophotometric analysis. The following oligonucleotide primers were used: forward: 5'–HEX–AGG ACC CTC ATG GCC TTG–3’, reverse: 5'–GCG ACT ACG TGG TCT ACT CG–3’. Amplification by PCR was performed in 20 μL reaction mixture containing 20 ng genomic DNA, 2 μL 10 × buffer, 25 mM MgCl2, 2 mM deoxynucleotide triphosphate, 7–deaza–2–deoxy GTP, 10 mM from each primer, and 0.2 μL Taq DNA polymerase. Amplification was performed using touchdown PCR. A 95°C incubation for 10 minutes was followed by two cycles of 95°C for 30 seconds, 65°C for 30 seconds, and 72°C for 60 seconds. The annealing temperature was decreased at every two cycles from 65°C to 57°C in 2°C decrements (10 cycles total), and a final 30 cycles of 95°C for 30 seconds, 55°C for 30 seconds, and 72°C for 60 seconds and a final 30–minutes incubation at 72°C. After amplification, PCR products were resolved and visualized in 2% agarose gel stained with ethidium bromide. 23
Statistical analysis
The results were analyzed on a compatible personal computer using the statistical package SPSS version (16.0). Qualitative data were statistically represented in terms of number and percent. Comparison between different groups in the present study was done using the χ 2 test. A probability value (P) ≤0.05 was considered significant.
Results
Demographic results
There was no statistically significant difference between cases and controls regarding sociodemographics. A higher percentage of male cases (73%) were seen as opposed to male controls (46.9%), which is consistent with the literature where there are more male children with ADHD than females. 24
Degree of consanguinity of parents showed a significant statistical difference when comparing cases to controls (P = 0.027). Cases’ parents were mostly first degree relatives and none were distant. Control's parents were mostly distant cousins. Family history of hyperactivity was statistically significant (P ≤ 0.001) when comparing cases to controls. However, family history of other psychiatric illnesses was not statistically significant. Parental age at birth of child was not statistically significant when comparing cases to controls. Among our ADHD patients, 34.4% (10 patients) had autistic symptoms, and 65.6% (19 patients) did not show autistic symptoms. Among those 65.6%, 14 patients showed ADHD combined type whereas 5 patients showed ADHD inattentive type.
ADHD and DRD4
The data illustrated in Table 1 reveals that the medium–sized repeats (4R, 5R and 6R) represent 82.3% of the VNTR variants among the studied sample of controls and 89.6% in ADHD children. When comparing allele frequency in ADHD patients with controls, the present data reveals that 4R variant is significantly different between the two groups. The 4R variant was not detected in the 62 studied chromosomes of controls, whereas it was detected in 8 of 58 ADHD chromosomes representing 13.7% with logical significance. On the other hand, the allele frequencies of the 5R and the 6R were not significantly different between the two groups. Short (2R and 3R) and long (7R, 8R, and 9R) repeats constitute 17.7% and 10.4% of the total number of variants in controls and ADHD patients, respectively, with no significant difference between the two groups.
Distribution of DRD4 48 bp VNTR among ADHD patients and controls.

Association of autism with DRD4
When comparing allele frequency in ADHD patients who exhibit autistic features with ADHD alone, the data in Table 2 demonstrate that there is a significant association between the possession of the four repeat allele with the children with ADHD alone (n = 19) than the ADHD with autistic features (n = 10) (P < 0.034).
Distribution of 48 bp VNTR of the DRD4 gene among ADHD children with and without autistic symptoms.
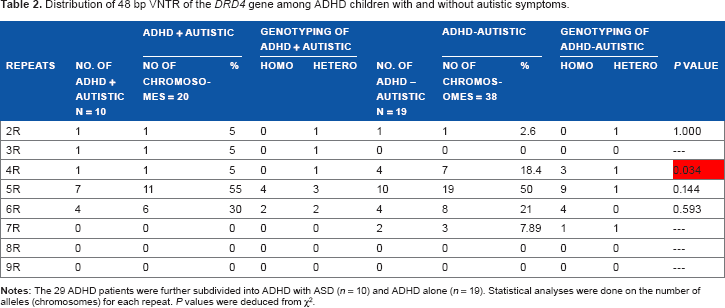
On the other hand, the allele frequencies of 2R, 5R, and 6R variants were not significantly different between the two groups. Long repeats (8R and 9R) were not detected in our patients, whereas 7R was only detected in the ADHD without autistic features and constitutes 7.89%.
Distribution of the most prevalent homozygous genotypes in the ADHD group and control
The data of Table 3 illustrates that 100% of ADHD patients (n = 3) had the homozygous genotype 4R/4R. The 4R/4R genotype was not observed in the control group.
Medium-sized DRD4 homozygous genotypes.

Association of the VNTR DRD4 gene with ADHD
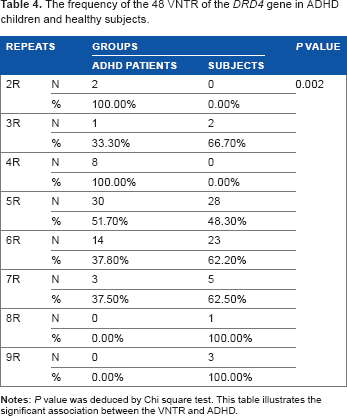
The data of Table 4 demonstrates that there was a significant association between possession of the 4R allele and ADHD (P= 0.002) as compared to control.
The frequency of the 48 VNTR of the DRD4 gene in ADHD children and healthy subjects.
Discussion
ADHD is considered one of the most common neurobehavioral disorders of childhood. 25 Among the genetic factors involved in ADHD, the DRD4 gene has been shown to be linked to ADHD in several meta–analyses.9,16,17,26,27 To our knowledge, no studies have been published on DRD4 linkage to Egyptian ADHD children. Improving the diagnostic process of ADHD children would have social and economical impacts. This study aims to explore the association between DRD4 polymorphism (which can serve as a diagnostic biomarker) and ADHD in a sample of Egyptian children.
The results of this study showed no statistical difference in socioeconomic (age, gender, and residence) between recruited cases and controls. Male:Female ratio is almost 7:3 in ADHD, a finding consistent with an earlier report of Pastor and Reuben. 24 The majority of ADHD cases (89.2%) and controls (78.1%) live in urban areas. The above findings indicate that controls and cases were homogeneously recruited regarding sociodemographics, thus excluding bias in subject enrollment. The importance of the genetic involvement in ADHD was supported in the present study, where approximately 30% of ADHD cases were offsprings of consanguineous marriages (21.6% first cousins and 8.1% second cousins). Parental age at pregnancy is not significant in ADHD cases from parents of controls, a finding supportive of earlier reports by Amiri et al. 28
Knowledge of genes of major effects allows identification of specific diagnostic biological markers. In the absence of clear definite objectives of clinical characteristics, the identification of these peripheral biomarkers in ADHD would be highly relevant for the diagnostic process. Identifying risky individuals at a younger age would allow implementation of treatments sooner to decrease the severity of ADHD symptoms or even to prevent future symptoms. 29 The enormous variability in the response of ADHD to treatment remains unexplained, while initial pharmacogenetic studies are intriguing and lack consistent reproducibility. 30 Understanding the contribution of genes to the phenotype and their interplay with specific medications would help in the treatment process. 8 This would inform better medication choices and maximize individual treatment outcomes, as well as identify optimal targets for future drug develop– ment. 30 Hopefully, specific genes with major effects and specific risk factors will be identified for future implementation of personalized medicine. This would be of great economical and social benefit because of the cost of the education of ADHD children, employment problems, and risks of developing addictions and antisocial behaviors associated with this disorder. 29
DRD4 gene exists in all individuals in a two–nine repeat alleles with the majority (80%–90%) of individuals either ADHD or controls; the most commonly detected alleles in our study are 4R, 5R, and 6R. The most striking finding in the current data is the prevalence of the 4R allele ~14% in ADHD versus zero in controls (highly logical significant difference). The current data are similar to those reported by Bidwell et al who showed the relevance of the 4R to ADHD. 23 Cheuk et al. 31 reported that the 4R allele (84%) and the 4/4 repeat genotype (70%) were the most prevalent; however, neither the family-based analyses nor the case control analyses showed any association between the DRD4 and ADHD.
The finding that 4R is a potential marker for ADHD in our population is obviously different from Caucasians who have the 7R allele, representing the more pathognomonic genetic factor. 27 The 7-repeat allele in the present study did not show any statistically significant difference where 6.8% of cases had the 7R as opposed to 16.1% in controls. The rest of the repeat alleles did not show any statistically significant difference as well.
Langley et al. 32 found that the children with and without the 7R did not show any statistically significant difference in the inattentive and hyperactive/impulsive ADHD symptoms.
Moreover, Carrasco et al. 33 found a negative association between the 7R allele and ADHD in a small case control study conducted on 26 ADHD children from Chile. In addition, Brookes et al. 34 reported that DRD4 gene markers investigated were not found to be associated with ADHD in this Taiwanese sample.
Swanson et al. 35 found that the distribution of the 4R and 7R were different between ethnic groups and between communities. Chang et al. 36 reported that the 4R allele is the most prevalent repeat in many populations and the distribution of the 4R allele varies from 0.16 to 0.96, while the 7R represents the second relevant allele and its distribution ranges from 0.01 to 0.78 Calahorro et al. 37 reported a positive association of the 7R allele of the DRD4 gene and autism; however, our present work did not show any association. The DRD4 exon 3 polymorphism is still unlikely to play a major role in the etiology of autism. Moreover, Grady et al. 38 reported that DRD4 7R haplotypes are ADHD specific.
Functional differences in the DRD4 intracellular signaling system have been studied for the 48-bp repeat alleles, and showed that the 7-repeat allele may be less sensitive to endogenous dopamine. The 7-repeat allele has been shown to mediate a blunted intracellular response to dopamine.13,39,40 The methylphenidate treatment has ameliorative effects as it increases the synaptic dopamine levels and compensates the blunted response of the receptor. Other studies demonstrated that all the 2, 4, and 7 repeat alleles displayed similar binding profiles. However, several others report no significant impact of the VNTR variants on the function of the DRD4 receptor.
Jovanovic et al. 40 suggested no major discrepancies in pharmacological or functional profile between long and short variants. Both receptors display, on average, a 15- to 90-fold lower potency for epinephrine/norepinephrine, respectively, compared with dopamine.
We postulate the poor association of the 7R allele with the DRD4 in our cohort to either of the following reasons (1) DRD4 is more strongly related to the inattentive than the hyperactive – impulsive symptoms of ADHD. Several studies have suggested that DRD4 is related to attention problems in the general population. 16 Bearing this in mind, our sample of children with ADHD consisted mostly of severe combined type, and the inattentive type was the smaller portion, thus explaining why 7R allele was not associated with ADHD symptoms. (2) Possible association of DRD4 with oppositional traits (which was in our exclusion criteria, and in turn, not well represented in the current sample). (3) Small sample size of the current study and that a larger sample size is needed for a genetic study to be able to identify multiple genetic factors, or (4) the cultural and the socioeconomic status have been found to moderate externalizing behavior and could also contribute to the difference in association between ADHD and DRD4 across racial–ethnic groups. 27 When comparing the homozygous genotypes of VNTR in DRD4 gene, the 4R/4R genotype has been found to carry a risk for developing ADHD suggesting that children with the 4R risk allele at both loci are at greater risk of ADHD.
In conclusion, contrary to the results of studies involving the Caucasian population in whom the 7R variant is found to be the better genetic marker associated with ADHD, this study reveals that 4R is the most diagnostic polymorphic variant of this disorder. The presence of 4R as either a single (heterozygous) or a double (homozygous) allele could be prognostic for ADHD.
Moreover, few studies have examined the association of candidate genes for one disorder in relationship to the other disorder. Our study has drawn attention to the involvement of the DRD4 in the specific ADHD children who did not exhibit autistic features, suggesting that the DRD4 is unlikely to play a role in ASD. When comparing ADHD children with autistic versus those without autistic symptoms, the possession of the 4R allele was statistically significantly different, P = 0.034 in the children with ADHD without autistic features. Our finding is consistent with the genetic linkage studies that have reported that the dopamine–related genes play pivotal roles in the ADHD. Nevertheless, further study is needed to increase the sample size in order to identify both common and rare genetic variants that account for the heritability of ADHD, especially regarding the Middle Eastern populations in which studies are limited.
Author Contributions
Conceived and designed the experiments: NAM, MKE. Formulated the hypothesis and methodology: OS, OR. Analyzed the data: RMD, MD. Wrote the first draft of the manuscript: RMD. Contributed to the writing of the manuscript: MD, NGB, OR. Agree with manuscript results and conclusions: OS, OR. Jointly developed the structure and arguments for the paper: OS, OR. Made critical revisions and approved final version: NAM, MKE, OS. All authors reviewed and approved of the final manuscript.