
Abstract
Aim
To measure levels of the collagen V formation marker CO5-1230 during liver fibrosis progression and regression.
Methods
Monoclonal antibodies were raised against the sequence TAALGDIMGH located at the start of the C-terminal propeptide between amino acid position 1230′ and 1239′ (CO5-1230). An assay developed using the biotin-streptavidin system was evaluated in a rat reversible model of fibrosis. Animals were treated for duration of 4, 6 and 8 weeks. Animals that were treated for 8 weeks were left to regress for a period of 14, 20 and 26 weeks.
Results
Mean CO5-1230 level for control animals was found to be 8.7 ng/mL. CO5-1230 marker levels, at termination points, for CCl4 treated animals was be 8.7 ng/mL at 4 weeks (P < 0.05, ROC: 0.83), 11.4 ng/mL at 6 weeks (P < 0.001, ROC: 0.93) and 10.8 ng/mL at 8 weeks (P < 0.05, ROC: 0.82). During regression phase, marker levels were statistically significantly decreased when compared with the marker levels at 8 weeks of treatment. Marker levels were found to be 5.9 ng/mL (P < 0.001, ROC: 0.8) after 14 weeks of regression, 3.9 ng/mL (P < 0.001, ROC: 0.95) after 20 weeks and 4.5 ng/mL (P < 0.001, ROC: 0.97) after 26 weeks of regression.
Conclusions
The data indicates that CO5-1230 levels are statistically significantly increased when CCl4 intoxication stimulus is applied in all treatment time points. CO5-1230 levels return back to control levels when the stimulus is removed. The above finding adds to our previous evaluation of the marker and suggests that CO5-1230 may be a promising potential marker for liver fibrosis staging and monitoring in both disease progression and regression.
Introduction
Excessive deposition of fibrillar extracellular matrix (ECM) components may occur in all tissues and organs as either a disease-specific fibrogenesis or as scar formation.1,2 Extensive tissue remodeling and fibrosis ultimately lead to organ failure due to the significant architectural modifications in the ECM. 3 This is evident in end-stage chronic liver disease, where cirrhosis is associated with significant morbidity and mortality.2,4
Fibrosis may begin in response to various acute or persistent stimuli that damage tissue.5,6 The tissue injury is followed by acute or chronic tissue repair which occurs as a series of dynamic events involving both cellular, molecular and immunological mechanisms.1,3,6,7 In the case of liver fibrosis, a series of events that involves several cell types including fibro-blasts, hepatocytes and hepatic stellate cells working in synergy ultimately causes damage to the liver.1,2,8
We have shown that as fibrosis develops, the formation of ECM molecules occurs more rapidly than during the degradation of fibrotic tissue. 9 We have also identified and described a panel of protein fingerprint markers for collagens I, III, IV and VI.5,10–16 These markers could potentially be useful for assessing chronic liver disease by evaluating the importance of different collagen types during pathology progression, and, by measuring different ECM constituents, building up a comprehensive ECM remodeling map. The markers could be classified according to the Burden of disease, investigative of intervention and diagnostic BIPED criteria for monitoring fibrotic pathology. 17
We have recently shown that increased serum levels of the formation marker PVCP-1230, from now on called P5CP, were associated with the extent of collagen deposition in two different models of fibrotic processes in the liver. 18 Type V collagen constitutes about 1%–5% of the total collagen in healthy tissue. However it has been shown to rapidly proliferate during ECM remodeling due to its structural position.19,20 Collagen V is known to be highly expressed during tissue development, wound repair and fibrogenesis, and its interaction with other cells such as fibroblasts seems to also affect ECM stiffness and cell behaviour.21,22 Increased amounts of collagen V have been reported in human alcoholic liver and in human bile ductule epithelia.23–25 Interestingly, increased amounts of collagen V localized in the thick fibrous septa have been reported during the progression of cirrhosis in rats injected with CCl4. 26 Takai et al interpreted the finding as a mechanism to protect the parenchyma from the excess type I collagen formed during pathogenesis. They also suggested that the increased collagen V played an anchoring role between the collagen fibril in the connective tissue and the lamina densa which ultimately enabled collagen V to regulate the surrounding stellate cells. 26 Collagen V has been shown to play a key role in the formation and assembly of collagen fibrils. 27 Thus, its regulation and remodeling may be of particular interest in a range of connective tissue pathologies. Despite the evidence regarding the implication of collagen V in fibrosis progression, its role is not fully explored and no markers based on collagen V have been utilized in clinical settings.
The aim of this study was to further characterize and validate serum P5CP as a marker of hepatic fibrosis progression or regression in a reversible liver fibrosis model using CCl4 in rats. Additionally, the study aimed to measure the marker in a less severe model of liver fibrosis which could potentially mimic the slow and progressive events occurring in human pathology.
Materials and Methods
Reagents
All reagents used for experiments were standard high-quality chemicals from Merck (Whitehouse Station, NJ, USA) and Sigma Aldrich (St. Louis, MO, USA). The synthetic peptides used for monoclonal antibody production were purchased from the Chinese Peptide Company, Beijing, China.
P5CP assay protocol
The assay protocol previously described
28
was altered significantly with a new assay buffer, coater/anti-body ratio and standard curve. A 96-well streptavidin plate (Roche Diagnostics, Basel, Switzerland) was coated with 3 ng of the biotinylated synthetic peptide, TAALGDIMGH-GGC-Biotin, diluted in coater buffer (25 mM PBS, 1% BSA, 0.1% Tween-20, pH 7.4 and 0.36% Bronidox) and incubated for 30 minutes at 20 °C. 20 μL of the peptide calibrator or sample were added to appropriate wells, followed by 100 μL of 15 ng horseradish peroxidase (HRP) (Innovabioscience, Babraham, Cambridge, UK). Conjugated monoclonal antibodies were diluted in the same buffer that was used for coating, and incubated for 1 hour at 20 °C. Finally, 100 μL tetramethylbenzinidine (TMB) (Kem-En-Tec cat.438OH, Taastrup, Denmark) was added, and the plate was incubated for a further 15 minutes at 20
Technical evaluation
From 2-fold dilutions of pooled human serum and urine samples, linearity was calculated as a percentage of recovery of the 100% sample. The lower limit of detection (LLD) was determined from 21 zero samples (ie, 25 mM buffer as described above) and calculated as the mean +3x the standard deviation. The inter- and intra-assay variation was determined by 10 independent runs of 8 human serum samples run in duplicate.
Reversible rat CCl4 liver fibrosis model
This animal study was performed according to the European Standard for Good Clinical Practice (2008/561-1450). P5CP levels were measured in a reversible CCl4 rat model of liver fibrosis. One hundred and twelve male Sprague-Dawley rats, 6 months old, were treated with CCl4 while another 28 male Sprague-Dawley rats were not treated and served as controls. Induction of liver fibrosis was performed as previously described.11,29 Briefly, 0.5 mL/kg of CCl4 diluted 1:10 in intralipid was administered by intraperitoneal injection once weekly. Animals receiving CCl4 were stratified into groups treated for 4 (n = 12), 6 (n = 18) and 8 (n = 22) weeks. To monitor the regression phase, another 60 animals received CCl4 until week 8 after which they were left to regress until being terminated at 20 weeks (n = 20), 26 weeks (n = 20) or 34 weeks (n = 20). Seven control animals were terminated at week 8 and at each of the three regression durations. At termination, blood was collected from rats that had fasted for at least 14 hours. The blood was allowed to stand at room temperature for 30 min to clot, before centrifugation at 2500 rpm for 10 minutes. All clot-free liquid was transferred to new tubes and centrifuged again at 2500 rpm for 10 minutes. The serum was then transferred to clean tubes and stored at −80 °C. Liver sections 4 μm thick were stained with 0.1% Sirius red (F3B) in saturated picric acid (Sigma-Aldrich, St. Louis, MO, USA).
Fibrosis quantification in CCl4 livers
Histology sections stained with Sirius red were analyzed using quantitative histology software Visiopharm version 3.2.8.0 (Hørsholm, Denmark). Images were acquired using Pixelink PL-A623C microscope digital camera (Pixelink, Ottawa, Canada).
Statistical analysis
Comparison of serum P5CP levels was performed using the unpaired t-test with Welch correction. Comparison of levels between regression time points (14, 20 and 26 weeks) and at week 8 of CCl4 treatment was performed using a one way ANOVA test, with a Dunnett's post test. Differences were considered statistically significant if P < 0.05. For correlation calculations the data was assumed to be sampled from Gaussian populations, and two tailed P values were calculated. ROC curves and all of the above calculations were performed using GRAPH PAD PRISM 5 (Graph Pad Software, La Jolla, CA, USA).
Results
Technical evaluation
The LLD of the modified P5CP assay was 0.51 ng/mL. Dilution recovery was within 100% ± 15% (Table 1). The inter- and intra-assay variation was below 10% (Table 2).
Percentage of the dilution recovery of the P5CP assay.

Inter- and intra-assay variation for the P5CP assays using human serum as quality control samples.

Serum P5CP during CCl4 induced hepatic fibrosis and regression following treatment
Mean serum P5CP levels of the control animals were 5.2 ng/mL at 4 weeks, 6 ng/mL at 6 weeks, and 6.1 ng/mL weeks at 8 weeks. The marker levels and ROC values were statistically significantly elevated in all CCl4 treatment groups (Fig. 1 and Table 3) compared with control rats. In CCl4-treated rats, the mean marker levels were 8.7 ng/mL at 4 weeks (P < 0.05, ROC: 0.85) representing a 67.7% increase over controls, 11.4 ng/mL at 6 weeks (P < 0.001, ROC: 0.93) and 10.8 ng/mL at 8 weeks (P < 0.05, ROC: 0.82) representing 113.4% and 107.6% increases respectively over controls. During the regression phase the marker levels were statistically significantly decreased when compared with the marker levels at week 8 of treatment. The mean marker levels were found to be 5.9 ng/mL (P < 0.001, ROC: 0.80) after 14 weeks of regression, 3.9 ng/mL (P < 0.001, ROC: 0.95) after 20 weeks and 4.5 ng/mL (P < 0.001, ROC: 0.97) after 26 weeks of regression. The best ROC sensitivity and specificity for P5CP during the progression phase was found to be 91.1% and 52.4% respectively. Overall the ROC sensitivity and specificity for the marker during the regression phase was found to be 96% and 60% respectively at the selected cut off points (Table 3). Sirius red staining of liver slices showed no sign of fibrotic bands in the control animals at any treatment time point (Fig. 3A). However, in CCl4-treated rats, fibrotic band formation was noticed at all progression time points (Fig. 3B). Fibrotic bands gradually reduced during the regression phases (Fig. 3C). The marker seemed to be correlated with total collagen levels as measured by quantitative histology (Fig. 2).

Serum P5CP levels during progression phase at 4 (n = 12), 6 (n = 13) and 8 (n = 20) weeks of CCl4 treatment.

Correlation of P5CP levels to total hepatic collagen during progression levels as measured by quantitative histology of a Sirius red staining in the livers of CCl4 rats at progression time points.
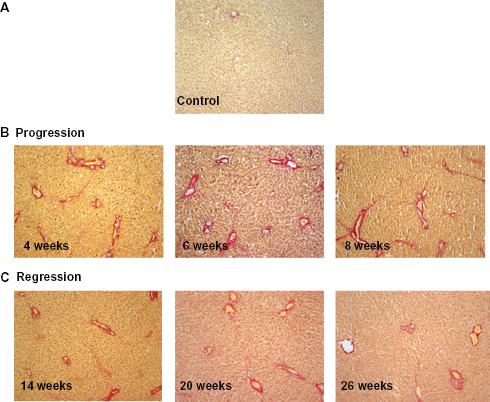
Total collagen deposition in liver slices as seen with Sirius red staining. Rats which received no CCl4 showed no visible collagen deposits or fibrotic band formation (A). Animals receiving a weekly dosage of CCl4 for 4, 6 or 8 weeks showed increased collagen deposition and fibrotic band formation (B). Rats which were treated for 8 weeks with CCl4 after which they were left to regress for 14, 20 or 26 weeks, revealed a gradual decrease in the total collagen deposition and fibrotic band formation (C).
ROC values of the P5CP marker during progression and regression phases.

Discussion
During fibrogenesis, levels of ECM components are significantly increased. Collagen V is an ECM component which seems to be an active participant in the events that lead to liver fibrosis and cirrhosis, 26 and in the process, collagen V fragments are released into the bloodstream. We have previously shown that levels of the collagen V formation marker P5CP were associated with the extent of collagen deposition in two different rodent models of fibrotic processes in the liver. 18 The ELISA used in those studies was further optimized for this experiment with resulting good native reactivity in both human and rat serum. The new assay was technically robust with acceptable inter- and intra-assay variation, dilution recovery, and a LLD (Tables 1 and 2). Our data show that serum P5CP was statistically significantly elevated in all CCl4 groups treated for up to 8 weeks. This result follows our initial evaluation of the marker in a more aggressive pre-clinical model of liver fibrosis. We believe that this finding may be related with the suggestion that increased collagen V levels may be a protective mechanism for the parenchyma and indicative of disease progression as suggested by Takai. However, additional studies are needed to confirm this suggestion. When the CCl4 intoxication was stopped, serum P5CP levels decreased to the level of the untreated, control rats. This is a key new finding for this study. This finding could be interpreted as an indication of the marker's association with the persistent stimulus (CCl4) fuelling ECM remodeling which leads to liver fibrosis. The ROC analysis at all progression and regression time points indicated the potential prognostic value of P5CP (Table 3). However, the prognostic potential should be interpreted with some caution as the fibrosis observed was only mild due to the once-weekly CCl4 treatment.
The P5CP amino acid sequence is located in the first 10 amino acids of the C-terminal propeptide which is a collagen formation specific region. We saw an increase in the collagen V fragment in the early stages of fibrosis in our preclinical model, and we therefore suggest that this fragment may hold a diagnostic potential that needs to be further investigated. The observation that the P5CP formation marker levels were reduced during the regression phase to the same level as controls may be suggestive of the underlying ECM adjustment towards balanced remodeling when CCl4 intoxication is removed.
Once-weekly administration of CCl4 was chosen in this study instead of the previously followed twice-per-week strategy. The decision was made in order to reduce the animal mortality rate and crucially to simulate the slower fibrosis process that takes place in human pathology. The initial characterization of the P5CP marker included a CCl4 model in which CCl4 was administered twice a week. 18 The histology results from that model revealed an aggressive pathology with severe fibrotic band formation and deaths among the experimental animals. In contrast, histology results from this study are indicative of a milder form of fibrosis in which increased collagen deposition and fibrotic band formation occurred at a slower rate. The histological examination during the regression phase suggested that the disease is reversible once the stimulus is removed. The observation that the P5CP marker levels also declined during the regression phase indicates that ECM remodeling also slows during the transition from pathology to physiology. The marker's potential utility in assessing efficacy of fibrosis treatments requires further investigation.
Conclusion
The study provides additional evidence that the collagen V formation marker P5CP may be a promising non-invasive marker for monitoring liver fibrosis. This study adds to our initial assessment of the marker, the finding that collagen V formation levels are normalized during regression stage of liver fibrosis. The observation that the marker is only elevated when the CCl4 stimulus is applied may indicate the marker's prognostic capacity due to early collagen V production. The observation that levels declined when toxic CCl4 administration ceased indicate this marker may also have potential as a measure of efficacy of treatments against fibrosis. However, further validation in pre-clinical and well characterized clinical cohorts is needed.
Study limitation
This study carries some limitations. One major limitation is that it was carried out in homogeneous, inbred laboratory rats with a synchronous induction of liver disease, which bears little resemblance to the highly complicated clinical presentation of liver fibrosis. Another major limitation was the lack of immunohistochemistry and western blots to add to the biological evaluation. This is due to the inability of the monoclonal antibody to show any applicable immunohistochemistry and western blot results, despite numerous attempts. Additionally, the preclinical study utilized is a mild model of fibrosis, and the marker should also be evaluated in the standard more aggressive models which typically administer CCl4 twice a week.
Author Contributions
Conceived and designed the experiments: EV. Analysed the data: EV. Wrote the first draft of the manuscript: EV. Contributed to the writing of the manuscript: SSV, MK, CH, DJL. Agree with manuscript results and conclusions: EV, MK, DJL, CH, MK. Jointly developed the structure and arguments for the paper: EV, MK, DJL, SSV. Made critical revisions and approved final version: MK, DJL. All authors reviewed and approved of the final manuscript.
Funding
The study conducted with funding from Nordic Bioscience.
Competing Interests
Efstathios Vassiliadis, Sanne Skovgård Veidal, Christina Hansen and Diana J. Leeming are full-time employees of Nordic Bioscience. Morten Karsdal also holds shares of the same company.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgment
We acknowledge the funding from the Danish Ministry of Science, Technology and Innovation and the Danish science foundation (“Den Danske Forskningsfond”).