
Abstract
Purpose
Current first-line chemotherapy for patients with metastatic adrenocortical cancer (ACC) includes doxorubicin, etoposide, cisplatin, and mitotane with a reported response rate of only 23.2%. New therapeutic leads for patients with refractory tumors are needed; there is no standard second-line treatment.
Methods
Samples from 135 ACC tumors were analyzed by immunohistochemistry, in situ hybridization (FISH or CISH), and/or gene sequencing at a single commercial reference laboratory (Caris Life Sciences) to identify markers associated with drug sensitivity and resistance.
Results
Overexpression of proteins related to demonstrated chemotherapy sensitivity or resistance included topoisomerase 1, progesterone receptor, and topoisomerase 2-alpha in 46%, 63%, and 42% of cases, respectively. Loss of excision repair cross-complementary group 1 (ERCC1), phosophatase and tensin homolog, O(6)-methylguanine-methyltransferase, and ribonucleotide reductase M1 (RRM1) was identified in 56%, 59%, 71%, and 58% of cases, respectively. Other aberrations included overexpression of programmed death-ligand 1 or programmed cell death protein 1 tumor-infiltrating lymphocytes in >40% of cases. In all, 35% of cases had a mutation in the canonical Wnt signaling pathway (either CTNNB1 or APC) and 48% had a mutation in TP53. No other genomic alterations were identified.
Conclusion
Biomarker alterations in ACC may be used to direct therapies, including recommendations for and potential resistance of some patients to traditional chemotherapies, which may explain the low response rate in the unselected population. Limited outcomes data support the use of mitotane and platinum therapies for patients with low levels of the proteins RRM1 and ERCC1.
Introduction
Adrenocortical cancer (ACC) is a rare malignancy occurring in approximately two out of a million people in the US. 1 At the time of initial presentation with ACC, 20%–50% of patients have metastases or stage IV disease.2,3 Patients with localized disease, who are able to undergo surgical resection with curative intent, often have a recurrence.2,4 Systemic treatment, therefore, remains a key component of therapy for most patients with ACC. The rarity of this disease has made it challenging to conduct clinical trials to inform efficacious therapy. First-line standard therapy consists of mitotane, either alone or in combination with etoposide, doxorubicin, and cisplatin (EDP-M). In a previous phase II trial, this combination had a superior response rate of 48.6% and an overall survival of 28.5 months when compared with other chemotherapy schemes.5–11 Unfortunately, in the recently completed FIRM-ACT phase III trial, EDP-M was associated with a response rate of only 23.2% and a median survival of 14.8 months. 12 Furthermore, the regimen was associated with significant toxicities, including leukopenia and neurologic side effects. There is no established standard second-line treatment for refractory ACC.
A significant advancement in the treatment of ACC would be made if physicians could accurately predict, for a particular individual, their tumor's sensitivity and resistance to various chemotherapeutic treatments. Patients whose tumors are unlikely to respond could be spared the toxicity associated with an ineffective treatment and receive an alternative treatment that has a higher chance of success. Recent studies have shown that for patients with refractory tumors, treatment selected on the basis of tumor profiling may result in better outcomes when compared to treatment based on physicians’ choice without molecular analysis.13,14
Previous evidence in human studies has shown that loss of protein or low expression levels of ribonucleotide reductase Ml (RRM1) and P-glycoprotein (PGP) are correlated with positive response to mitotane 15 and doxorubicin, 16 while overexpression of topoisomerase 2-alpha (TOPO2A) is correlated with a positive response to etoposide. 17 Therefore, in this study, we investigated whether one could identify molecular markers in ACC, such as RRM1, PGP, and TOPO2A expression levels, which might explain why a patient's tumor might or might not respond to standard chemotherapy and identify alternative treatment approaches in patients with refractory ACC. We assayed markers of drug resistance as well as targets for anticancer drugs in a set of 135 tumor samples from patients with primary, recurrent, or metastatic ACC. We found that a majority of patients had elevated markers suggestive of drug resistance to standard first-line ACC chemotherapies. Encouragingly, we also identified potential second-line therapeutic options by observing the expression of a number of markers for sensitivity to other agents. Additionally, in a limited set of patients for whom treatment and outcomes data were available, we evaluated response to treatment based on biomarker status.
Materials and Methods
One hundred thirty-five formalin-fixed paraffin-embedded adrenal cancer samples sent to a commercial molecular profiling laboratory (Caris Life Sciences) for analysis by treating physicians around the world were analyzed using one or more technologies, described later, to identify markers of drug sensitivity and resistance. Biomarkers for analysis varied by case, dependent on tissue availability, physicians’ preference, technology standards over the course of the study, and their potential to be targeted therapeutically and/or based on clinical evidence of a utility in other solid tumors. The specific histology was confirmed by evaluation of hematoxylin and eosin slides. Pathology reports submitted by the treating physicians were further reviewed and verified by board-certified pathologists at Caris. Pediat-ric patients and patients with either adrenal large cell neuroendocrine carcinosarcomas or pheochromocytomas were excluded from the analysis. The Weiss score was not used, because only 30% of the cases submitted to Caris had details of the microscopic examination available that would allow for Weiss grading/scoring, and because in the absence of a strict education and standardization process, significant interobserver variation in Weiss scores has been demonstrated. 18 In accordance with Western Institutional Review Board (IRB) guidelines, because patient identity protection was maintained throughout the study, the study was considered IRB exempt.
Patient demographics
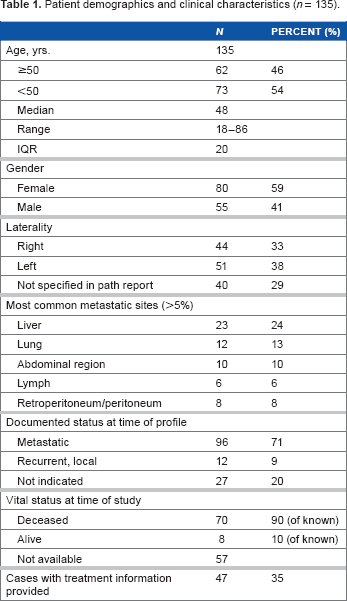
Patient demographics and clinical characteristics (n = 135).
Immunohistochemistry
Protein expression was assessed by immunohistochemistry (IHC), as previously described. 19 Cancer cells on slides were scored by pathologists. For PD-1, the tumor-infiltrating lymphocytes (TILs) were scored. Protein was considered overexpressed, when the percent staining and intensity were above previously published and validated thresholds specific to each marker, for proteins where increased expression levels were of interest; when loss of protein or underexpression of protein was of interest, percent staining and intensity below previously published and validated levels were reported. 19 Antibodies used included: androgen receptor (AR), topoisomerases 1 and 2 (TOPO1, TOPO2A, Leica Biosystems), estrogen receptor (ER), progesterone receptor (PR), cMet, human epidermal growth factor receptor 2 (HER2; Ventana), cKIT, epidermal growth factor receptor (EGFR), phosophatase and tensin homolog (PTEN; Dako), O(6)-methylguanine-methyltransferase (MGMT), PGP, thymidylate synthase (TS; Invitrogen), transducin-like enhancer of split 3 (Santa Cruz), excision repair cross complimentary group 1 (ERCC1; Abcam), RRM1 (Proteintech), SPARC (monoclonal; R&D Systems and polyclonal; Exalpha) and tubulin beta-3 chain (Covance), programmed cell death protein 1 (PD-1), and programmed death-ligand 1 (PD-L1; BD Pharmingen and R&D Systems).
In situ hybridization
Fluorescent in situ hybridization (FISH) and, more recently, chromogenic in situ hybridization were used for evaluation of HER2/neu, EGFR, and cMET, as previously described. 19
Mutational analysis
Next-generation sequencing (NGS)
Direct sequence analysis was performed on genomic DNA isolated from formalin-fixed paraffin-embedded tumor samples using the Illumina MiSeq platform (Illumina). Specific regions of 46 genes of the genome were amplified using the Illumina TruSeq Amplicon Cancer Hotspot panel, as described previously. 19
Sanger sequencing
Prior to the availability of Clinical Laboratory Improvement Amendments (CLIA) certified NGS, mutation analysis by Sanger sequencing included selected regions of BRAF, KRAS, cKIT, EGFR, and PIK3CA genes and was performed using M13-linked PCR primers designed to amplify targeted sequences. PCR products were bidirectionally sequenced using the BigDye Terminator v1.1 chemistry and analyzed using the 3730 DNA Analyzer (Applied Biosystems). Sequence traces were analyzed using Mutation Surveyor software v3.25 (SoftGenetics).
Statistical analysis
The patient population and profiling data were characterized using standard descriptive statistics, performing Fisher's exact test using GraphPad. The nonparametric Kaplan–Meier statistic was used to estimate the fraction of patients surviving in analyzed groups, to determine significance, using JMP software. When noted, subgroups were analyzed separately from the entire cohort.
Results
Analysis of biomarkers evaluated by immunohistochemistry
IHC markers of sensitivity and resistance to current ACC therapy.
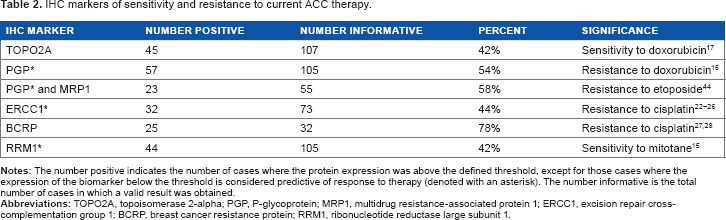
In the limited number of patients for whom we had clinical data, we analyzed the association between protein expression levels and treatments correlated to potential benefit. Forty-nine of the patients with clinical outcomes were evaluated for TOPO2A protein expression; 20 of these patients overexpressed TOPO2A (>1+ intensity and >10% staining); however, none were treated with the topoisomerase inhibitors doxorubicin or etoposide, perhaps because they had already been treated and they now exhibited refractory disease. Seven of the 29 patients with low TOPO2A were treated with doxorubicin, which is predicted to be associated with a lack of benefit. The average survival in those 7 patients was 38 months, compared to the 22 patients not treated with doxorubicin who had an average survival of 50 months (P-value = 0.574). PGP expression, a protein known to transport doxorubicin out of the cell, was not different between these two groups. Of 46 patients with RRM1 expression status who were treated with mitotane, 25 patients with low RRM1 levels survived an average of 9 months longer than 21 patients with high expression of RRM1 (P-value = 0.369). Notably, of 10 patients whose ERCC1 protein expression levels were tested and who with platinum therapy; four patients with low ERCC1 levels (<2+ intensity and <10% staining) had statistically significant survival benefit compared to six patients with normal ERCC1 expression (44 vs. 22 months; P-value = 0.0356).
IHC markers for sensitivity to other agents, in recurrent and metastatic cases analyzed in this study.
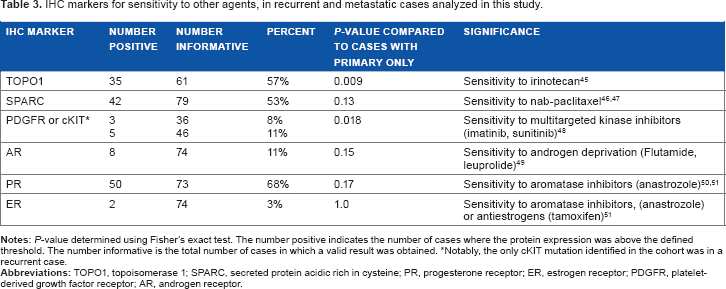
Notably, the only cKIT mutation identified in the cohort was in a recurrent case.
Analysis of immune checkpoint biomarkers, PD-1 and PD-L1, identified PD-1 TILs in 20% of cases (9/46), overexpression of PD-L1 in 30% of cases (14/46), concurrence of PD-1/PD-L1 in 9% of cases (4/46), and occurrence of either PD-1 or PD-L1 in 41% of cases (19/46; Fig. 1).
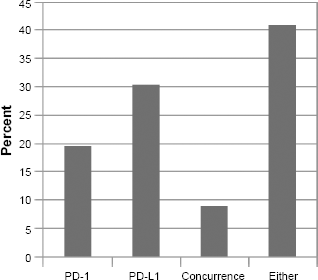
IHC analysis of PD-1 TILs and/or PD-L1 expression. Concurrence occurs when both an increase in PD-L1 and expression of PD-1 on the TILs were identified in a sample. Either indicates that either PD-1 or PD-L1 was identified in a sample.
All markers tested by IHC are shown in Figure 2. Of note, PR was overexpressed in 63%, AR in 8%, and EGFR in 33% of cases. EGFR overexpression was seen in half as frequently as previously reported
29
; however, the published incidence was obtained using a different and less specific antibody. Loss of MGMT protein expression was identified in 71%, loss of PTEN in 59%, and low TS in 65% of cases. PTEN loss is noteworthy, as the PI3 kinase pathway (specifically overexpression of mammalian target of rapamycin [mTOR]) has been identified in the tumorigenesis of ACC, and recent phase I trials with mTOR inhibitors have shown promise.30,31 Therefore, treatment with everolimus or temsirolimus may provide benefit in those patients with loss of PTEN. Loss of MGMT has been associated with beneficial treatment utilizing temozolomide in other cancers; therefore, this treatment in ACC patients with low MGMT may be another area for exploration.
Protein expression by IHC, reported as number positive (protein expression above defined threshold) of total cases tested in parentheses and shown as percent expression in graph. Associated therapies, based on current evidence, are indicated in the second parentheses.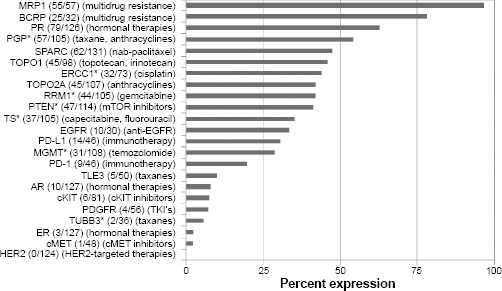
Analysis of biomarkers evaluated by in situ hybridization
The most commonly amplified gene was EGFR (5/45, 11.5%). Amplification of the cMET and HER2 genes were identified in single cases: cMET (1/38, 2.6%); HER2 (1/60, 1.7%). Together, EGFR protein overexpression or gene amplification of EGFR in 21% of cases suggests consideration of treatment targeting EGFR.
Analysis of biomarkers evaluated by mutation analysis
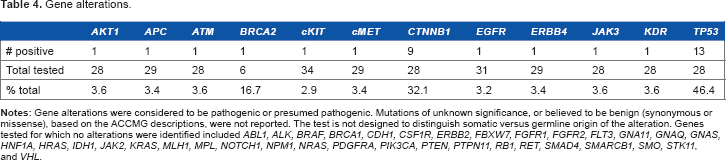
Gene alterations.
Discussion
Rare and aggressive tumors such as ACC pose a particular challenge to patients and their treating physicians. In ACC, little data exist to guide treatment decisions if first-line treatment with EDP-M fails. The present study is novel because it is the first to examine a large number of ACCs from patients with primary, metastatic, or refractory disease for established markers of sensitivity or resistance to chemotherapeutic agents. In the absence of clinical trials to establish second-line treatment, the expression of drug targets in refractory ACC can offer guidance to the selection of a chemotherapeutic regimen for these patients. While this study demonstrated that markers of resistance were elevated in a majority of patients with recurrent or metastatic disease, it also identified expression of markers and relevant genes that suggested other potentially more efficacious chemotherapeutic agents. The results suggest that biomarker-driven clinical trials might provide insights into potential novel targeted therapies. Histology-based trials may also be useful for ACC, to further refine biomarker-associated differences in response to chemotherapies, as suggested by the limited outcomes seen in this cohort. This is also the first report establishing the presence of PD-1 and PD-L1 receptors in ACC, suggesting that further study of the potential role for this class of immune modifier drugs in the treatment of ACC is warranted. Ongoing immunotherapy-focused clinical trials including ACC patients may shed further light on their efficacy in ACC.
EDP-M is a rigorous chemotherapy regimen associated with substantial toxicity. As the response rate is only 23%, 12 a method to predict whose cancer would be likely to respond could result in a higher quality of life for a significant number of patients. Patients who have biomarkers predictive of resistance to one or more components of EDP-M could be placed on another, potentially more effective regimen, which may reduce toxicity and increase the likelihood of clinical response.
One agent of EDP-M, doxorubicin, is an anthracycline that binds to and intercalates with DNA and functions as a topoisomerase II inhibitor. Evidence outside of ACC suggests that this drug may be beneficial for patients whose tumors have elevated expression of TOPO2A. 17 Unfortunately, in the limited cohort of patients for whom we have treatment and outcomes data, no patients with elevated expression of TOPO2A were subsequently treated with topoisomerase II inhibitors. However, we found decreased overall survival in low TOPO2A patients compared to the overall study population. Doxorubi-cin is a substrate for PGP, which binds and transports this drug out of the cell as part of the multidrug resistance mechanism.37,38 Patients with high levels of PGP have been shown to have higher levels of resistance to doxorubicin. We did not, however, observe any differences in survival between the high and low PGP cohorts treated with doxorubicin. Cisplatin, a platinum-based agent in EDP-M kills tumor cells by binding and cross-linking DNA strands, causing DNA damage and triggering cell death pathways. Tumor cells can offset the effects of platinum-based agents by implementing DNA repair mechanisms, particularly via the action of ERCC1. Platinum-based agents have been shown to be relatively ineffective in patients whose tumors harbor a high level of ERCC1 expression.16,17,22–24 In ACC, Ronchi et al showed that high ERCC1 expression was an indicator of poor responses in platinum-treated patients. 26 Our findings are supportive of this conclusion, in that patients with high expression of ERCC1 who received platinum therapy had significantly shorter survival than patients with normal ERCC1 expression receiving platinum therapy. Mitotane (o'p'DDD) is a part of the EDP-M regimen but is also approved as monotherapy for ACC. Drug toxicity at therapeutic doses often limits efficacy. 20 In vitro and in vivo data using gene expression support the use of RRM1 as a biomarker for prediction of response to adjuvant mitotane in ACC. Adjuvant mitotane resulted in improved progression-free survival in the presence of low expression levels of RRM1 by real time polymerase chain reaction (RT-PCR). 15 There was no benefit among patients whose tumors expressed high levels of RRMI, nor was there improved overall survival in either study population. Our limited clinical data, which examined protein levels of RRM1 by IHC, trend in the same direction for patients with metastatic ACC.
There is evidence from in vitro studies that mitotane offsets the action of PGP; 39 however, this has not been substantiated by in vivo studies. 6 Continued work on PGP antagonists such as tariquidar has shown evidence of PGP inhibition in vivo in metastatic ACC. 40 Our study demonstrated overexpression of PGP in 54% of tumors and provides further support for the pursuit of effective PGP antagonists. Our dataset was too small to evaluate the outcomes in patients with coincidence of overexpression of PGP and low expression of RRM1.
Our study suggests that other chemotherapeutic agents might have efficacy in selected patients with ACC. No protein or molecular marker suggesting efficacy was universally present, further indicating that an individualized approach to the selection of a treatment regimen for patients with refractory adrenal cancers is needed. Overall, we found that a majority of tumors in this cohort had high expression of markers indicative of drug resistance to one or more of the standard agents used to treat ACC, highlighting the need for the discovery of new options. Our study identified several biomarkers aberrantly expressed in ACC that have proven helpful in other cancers. For example, a recent case report
41
profiled an ACC tumor that had low expression of TS and high expression of TOPO1, leading to a decision to treat with
Other targets were identified in the Wnt and PI3K pathways, as well as TP53. While no currently FDA approved drugs target aberrations in the Wnt pathway, the finding of mutations in the beta-catenin gene and/or APC in 38% of ACC suggests that Wnt inhibitors under development, such as PRI-174, should be studied in patients with ACC. Similarly, clinical trials targeting TP53 might be warranted, as ~50% of ACC patients in our cohort of refractory ACC, presented with TP53 mutations. Another area for clinical trials might be the PI3 kinase pathway; 57% of cases had a loss of PTEN and a single case had an AKT1 mutation, despite no mutations being found in either PTEN or PIK3CA.
Considerable interest has arisen in oncology, with the promising new agent inhibiting PD-L1 and programmed death 1 (PD-1). 42 While PD-L1 and PD-1 are frequently found to be expressed at high levels in many cancers, there have been no prior reports characterizing the levels of expression in a large set of adrenal cancers. In our sample set, we found PD-L1 expression in 30% and PD-1 positive TILs in 20% of ACC cases tested. PD-L1 expression by tumors has been associated with favorable responses to target inhibition in clinical trials. 43
Combining drugs that target PD-1/PD-L1 with cytotoxic chemotherapy is also gaining interest for tumors, including melanoma, non-small cell lung cancer, renal cell carcinoma, and other cancers, and may be an attractive option for further investigation in ACC patients with tumors overexpressing PD-1/PD-L1.
One limitation of our study was a lack of clinical data, as is it was not known which agents were chosen for 70% of the patients. Furthermore, this study cannot address the question of whether one should use adjuvant treatment with mitotane or another agent in resected high-risk adrenal cancer. Also, because these cases were tested on a commercial platform over several years, the availability of different tests changed, and not all cases had the same group of tests performed. And finally, the low frequency of actionable mutations identified suggests that Hotspot analysis of a small gene panel may have limited scope in ACCs. Furthermore, an evaluation of the percent of patients with germline versus somatic incidence of TP53 may be relevant, as germline TP53 mutations (Li-Fraumeni syndrome) are more common than somatic mutations in ACCs. The Illumina technology used was not designed to provide this distinction.
Overall, our data suggest that a multiplatform molecular profiling of refractory ACC tumors can offer insights to explain disease progression on standard chemotherapy and can also offer options for second-line therapy, to improve both outcomes and quality of life. Continuing evaluation is needed in the understanding of the molecular landscape of ACC in order to develop new and more effective treatments. Toward that end, this report provides insights at both the protein and genomic level, identifying clinically applicable known therapeutic targets in a large subset of ACC patients.
Author Contributions
Conception and design: MJD, SE, and SZM. Collection and assembly of data: SZM. Data analysis and interpretation: MJD, SE, and SZM. Manuscript writing: MJD, SE, and SZM. Jointly developed the structure and arguments for the paper: MJD, SE, and SZM. Made critical revisions and approved the final version: MJD, SE, and SZM. Final review and approval of the manuscript: MJD, SE, and SZM.
Footnotes
Acknowledgments
The authors acknowledge the significant contributions made by Nancy Doll, RN, CTR, for extensive review of clinical data.