
Abstract
This paper presents a fuzzy neural network (FNN) control system to automatically manage the hemodynamic variables of patients with hypertension and congestive heart failure (CHF) via simultaneous infusion of cardiac drugs such as vasodilators and inotropic agents. The developed system includes two FNN sub-controllers for regulating cardiac output (CO) and mean arterial pressure (MAP) by cardiac drugs, considering interactive pharmacological effects. The adaptive FNN controller was tested and evaluated on a cardiovascular model. Six short-term therapy conditions of hypertension and CHF are presented under different sensitivities of a vasodilator drug. The results of the automated system showed that root mean square errors were ≤ 5.56 mmHg and ≤ 0.22 L min-1 for regulating MAP and CO, respectively, providing short settling time responses of MAP (≤ 10.9 min) and CO (≤ 8.22 min) in all therapy conditions. The proposed FNN control scheme can significantly improve the performance of cardiac drug infusion System.
Keywords
Introduction
Hypertension and congestive heart failure (CHF) are the most common cardiovascular dysfunctions, especially for cardiac surgery patients. 1 In hypertension, the risk of structural damage for the cardiac work and the blood vessels increases as the arterial pressure increases. 2 Therefore the high blood pressure is not only the main cause of heart attack, but also it is a major cause of heart failure. CHF is a condition of the heart failure to pump insufficient blood to meet the needs of the body's tissue. 3 CHF clinical syndrome is characterized by exercise intolerance and shortness of breath.
Hemodynamic variables such as mean arterial pressure (MAP) and cardiac output (CO) are often required to be maintained within nominal ranges by infusing the therapeutic agents directly into the blood of post-operative surgery patients. 4 Intravenous (IV) cardiac drugs; namely vasodilators and inotropic agents provide the first aid to physicians for the treatment of hypertension and CHF.4,5 Vasodilators reduce the load on the myocardium, while inotropic agents increase directly the strength of contraction of cardiac muscle and oxygen demand of myocardial. Sodium nitroprusside (SNP) and dopamine (DPM) are good examples of vasodilator and inotropic drugs respectively. 5
Although the CVS modeling cannot completely describe the CVS human physiology, compartmental models provide a good tool to describe physiological systems, including clinical pharmacology for closed-loop control of drug administration.6,7 Our functional cardiovascular model (FCVM) was therefore used to simulate the physiological behavior of patient under different CVS disorders and pharmacological effects of IV cardiac drugs as well.8,9 Without loss of generality, the values of FCVM parameters are based on the experimental data for 18-kg canine.10,11
Closed-loop control systems for clinical pharmacology can significantly improve the quality of IV drug administration, specifically controlling of drug infusion rate in surgery and intensive care unit. 12 Therefore the motivation of this paper is to develop a well designed controller for automated IV cardiac drug infusion system.
Sheppard 13 applied a proportional-integralderivative (PID) controller with a decision table to administrate SNP infusion in hypertensive patients. Simultaneous control of hemodynamic variables is often a goal in clinical situations using multiple drug infusion.14,15 Different fuzzy logic control (FLC) schemes have been also implemented as Multiple-Inputs-Multiple-Outputs (MIMO) drug infusion controllers. Held and Roy16,17 developed multiple drug control by a supervisory-fuzzy rule-based adaptive controller to regulate the hemodynamic variables for the CHF only. Supervisory capabilities are added to ensure adequate drug delivery with different values of SNP sensitivities. Huang and Roy 18 extended the above supervisory fuzzy rules-based controller to manage more hemodynamic variables by using many IV cardiac drugs, assuming a constant SNP sensitivity.
The application of neural networks to control drug infusion system has been also investigated. Chen et al 19 and Kashihara et al 20 developed adaptive controllers based on multilayer neural networks to regulate the arterial blood pressure during hypertension and hypotension respectively. Kashihara 21 extended the controller 20 to MIMO infusion control of dobutamine and SNP drugs in acute heart failure.
Although a neural network is able to learn from data, the trained neural network is generally understood as a black box. 22 Also, no structural information can be extracted from the trained neural network. On the other hand, fuzzy logic controllers are designed to work with structured knowledge in the form of rules and nearly everything in the fuzzy control system is highly transparent and easily interpretable. 23 However, there is no formal framework of fuzzy control system for the choice of design parameters and the optimization of these parameters is generally done by trial and error. 24
A combination of neural networks and fuzzy logic offers the possibility of solving tuning problems and design difficulties of fuzzy logic. 25 The resulting network will be more transparent and can be easily recognized in the form of fuzzy logic control schemes. This approach combines therefore the well established advantages and avoids the drawbacks of both methods.
Few previous studies were carried out in developing FNN controllers for cardiac drug delivery system. Nie and Linkens 25 tested different fuzzy-neural control schemes to provide IV drug administration for controlling the changes in MAP and CO. Although these controllers showed good transient performance, a first-order steady state model of the CVS was used. Also, the small value of the patient's sensitivity was presented as a random noise of 10% variations in steady state gains and time constants.
We have previously presented a simplified TS fuzzy PID (STS fuzzy PID) controller for simultaneous administration of IV drugs under different CHF conditions only. 26 However, STS fuzzy PID controller did not completely satisfy the therapeutic drug effects in all therapy conditions, because a short overshoot response of blood pressure was observed outside the desired ranges.
In this paper, we present a FNN control system for automated IV drug infusion system, in order to regulate the hemodynamic variables under different short-term therapy conditions of hypertension and CHF. The developed FNN control system is based on direct adaptive control strategy of the neural networks using online back-propagation learning algorithm. Moreover, the performance of adaptive FNN control system has been evaluated by comparing the obtained results with different fuzzy controllers such as SFLC and STS fuzzy PID.
Automated Drug Infusion system
Figure 1 depicts the main components of closed-loop cardiac drug infusion system. The sensors detect and measure MAP and CO. Based on these measurements and the desired hemodynamic values (MAPd and COd), the developed FNN control system determines the suitable amount of drugs to be applied. Drug infusion pumps are then activated by the controller outputs, USNP and UCO, to inject the accurate doses of SNP and DPM inside the venous of patient. The patient's model and the FNN control system are described in the next sections.

Block diagram of automated intravenous cardiac drug infusion system.
Patient's model
In this study, a FCVM has been used as a patient's model.8,9 The FCVM is composed of a controlled CVS and therapeutic effects of SNP and DPM drugs. The controlled CVS includes full compartments of the systemic and the pulmonary circulations, integrated with a baroreflex-feedback regulatory mechanism model as short-term blood pressure regulation. The long-term blood pressure controls of hormonal and renal activations are ignored in this study because the effect of long-term regulation is much slower than the baroreflex-feedback. 27
Hypertension is induced in the FCVM by resetting of the baroreflex-feedback model to 20 mmHg or more above the nominal value. 28 CHF is represented as a reduction in the contractility of left ventricle below the nominal value. 3 Therefore, CHF provides a significant drop in CO to 1.5 L min-1 and MAP reduced to 99.0 mmHg as well.
The target sites of SNP effect are the unstressed blood volume of large veins, the arterioles resistance, and the pulmonary capillaries resistance which affects the arterial blood pressure. 11 The contractility of left ventricle and the arterioles resistance are modified by the pharmacological effects of DPM. 11 For more details about the FCVM and open-loop IV drug responses, see Ref.8,9
FNN control system
Controller criteria
For hypertension, the therapeutic goal of cardiac drugs is to reduce the high MAP to the normal level above the hypotension value. In CHF therapy, it is desired to bring the CO to an acceptable range while keeping the blood pressure at desired lower levels.
Imposing a maximum infusion rate in the controller limits its action. But it must be applied to avoid the drug toxicity and achieve the desired therapeutic drug responses. During the drug infusion time, t, the following constraints on SNP and DPM infusion rates are applied: 29


Control system configuration
The proposed control system includes a FNN controller (FNNC), and a reference trajectory of hemodynamic variables, see Figure 2. In this study, the type of adaptive FNNC is multi-layer feedforward networks. 22 The inputs of FNNC are the error, e, and the change of error, Δe, of MAP and CO. The outputs of FNNC are the drug infusion rates, uSNP and uDPM. The reference trajectory provides a smooth transition from the initial actual values of hemodynamic variables to the desired values. Hence, the IV cardiac drugs can be smoothly injected.
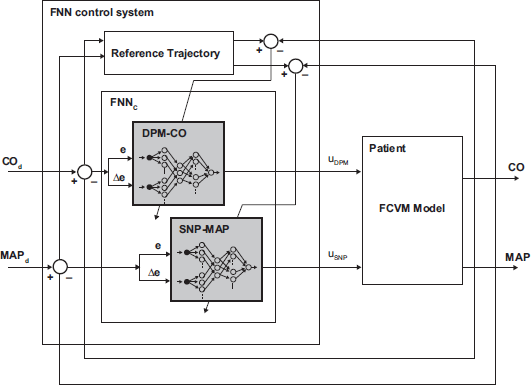
Block diagram of adaptive FNN control system in a closed-loop drug infusion system.
Using two separate FNN sub-controllers for heart failure therapy allows a better learning of FNN during closed-loop control and performs a faster control action than one controller including drug interaction disturbance. 21 Therefore, the FNNC includes two subcontrollers for the DPM-CO and the SNP-MAP, considering the drug effects of SNP on CO as well as the effects of DPM on MAP. Six Scaling factors are used to adjust the input/output of FNNC sub-controllers into proper ranges, which are: GeCO = 10.0, GΔeCO = 10.0, GeMAP = 0.05, GΔeMAP = 0.1, and the control outputs for the infusion rates of SNP and DPM are scaled by 10 and 6 respectively.
Each FNNC sub-controller consists of five connected layers based on the basic design of FLC. 30 In five-layered FNN structure the function and the signal propagation in each layer are described as follows.
Layer 1: Input layer
Every node i transmits the scaled e and Δe of hemodynamic variables to the next layer without any adjustment. The net input and the net output of this node are represented as

where x11 = e and x12 =Δe. The link weight at input layer is unity.
Layer 2: Fuzzification layer
The scaled hemodynamic errors are converted to the corresponding fuzzy values using a Gaussian membership function in jth node of layer 2 by

where mij and σ ij are, respectively, the centre (or mean) and the width (or variance) of the Gaussian function of the jth fuzzy term of the ith input linguistic variable x2 i to the node of membership layer. mij is also the link weight at layer 2.
Layer 3: Rule layer
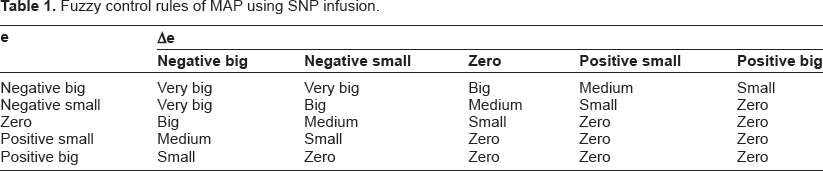
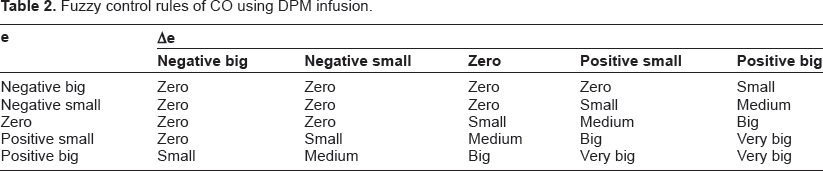
Tables 1 and 2 illustrate twenty five fuzzy control rules using IF-THEN rule for regulating the MAP and the CO respectively. Fuzzy control rules are implemented in the rule nodes using Larsen's product,

where x3j represents the jth input to the k node of rule layer. The link weight in layer 3 is unity.
Fuzzy control rules of MAP using SNP infusion.
Fuzzy control rules of CO using DPM infusion.
Layer 4: Fuzzy output layer
For the fired rules which have the same consequence x3 k , the links at layer 4 perform a fuzzy OR operation layer 4 to generate the fuzzy output y4g,

the link weight at layer 4 is unity. The output membership functions are similar to the input membership functions in layer 2, but they are shifted to the positive side to ensure the therapeutic ranges of cardiac drugs as illustrated in Tables 1 and 2.
Layer 5: Control output layer
The crisp control output is given by using the center of area (COA) method,

where y15 = uDPM for DPM-CO controller and y15 = u SNP for SNP-MAP controller. x4 g is the gth input to the node of layer 5. mog and σ og are the center and the variance of the Gaussian function respectively at the output layer. n is the total number of the fuzzy term set of the gth group at layer 4.
The initial setting of FNNC parameters are estimated to behave as a SFLC based on physician expert experience. Therefore, it is necessary to tune these values in order to achieve the therapeutic objectives and also to improve the performance of closed-loop drug infusion system. In this work, the basic idea of the back-propagation learning algorithm 31 is used to adjust online all FNNC parameters, particularly the shapes of Gaussian membership functions in layer 2 and layer 4 as follows: The learning algorithm is needed to minimize a least-squares error function

where yr and yh are the reference output and the current actual hemodynamic value. At the output layers of the FNNC, a backward propagated signal is used to compute ∂E/∂W for all nodes in the hidden layers. The adjustable parameter w is updated by

where w* and w are the single parameters of each layer connection after and before updating respectively, Δw is the modified parameter. y presents the net output of a node of each layer. The updated parameters are usually the center and the width of membership functions. η is the learning rate and equals to 0.1 for two FNNC sub-controllers. The error gradient at the output layers of FNNC is

where the term yh/y5 o presents the internal patient's sensitivity around the stationary state. In this study, we assumed that this sensitivity term can be directly obtained as 7 times of the back-propagated errors without using identification neural networks model of the patient, or changing the structure of FNNC to recurrent neural networks. 32
Validation
To determine the appropriateness of the developed FNNC for automated IV cardiac drug infusion system, the obtained results have been compared with SFLC and STS Fuzzy PID controllers. The accuracy of hemodynamic variables regulation was estimated by computing the root mean square error (RMSE) between the measured variable yh and the desired hemodynamic value yd over the total number of measurements N,

The settling time Ts is the time for the patients’ responses to reach 5% of its final hemodynamic values within the accepted levels. Ts is calculated in minutes for both MAP and CO to show the speed responses of fuzzy drug infusion controllers.
For SNP and DPM drugs, the total injected amount of each IV drug is estimated in μg, in order to assess a controller which achieves the desired therapeutic effects with a minimum pharmacological infusion.
Results and Evaluation
This study is valid only in short-term heart failure therapy. Therefore the IV infusion time is selected to be 20 min. The sample time interval of drug infusion is 30 sec. 29 The patient's model and control algorithms are implemented using MATLAB®.
In clinical situations, it is common for physicians to specify an operating range for the hemodynamic variables instead of a single setpoint. 15 Therefore, this study uses the allowable normal ranges which are ±5% of the nominal value for MAP and above 80% of the nominal value for CO. 16 A change in patient's sensitivity to a SNP drug from 50%–200% of the normal value (SNP sensitivity = 1) is simulated as low and high SNP sensitivities respectively.
For hypertension therapy, the desired range of MAP is 120.0 %pM 6.0 mmHg. In CHF therapy, CO is required to be elevated to 1.9 L min–1 above the lowest level 1.65 L min–1 and MAP is maintained at 99.0 ± 6.0 mmHg.
Figure 3 shows the patient responses under normal, high, and low SNP sensitivities in hypertension therapy using adaptive FNNC. The DPM infusion rate is not activated in hypertension cases, because the CO is always above the nominal level. Under normal SNP sensitivity, the FNNC causes a reduction in high MAP from 140 mmHg to 121.18 ± 4.317 mmHg in 2.313 min, see Figure 3A. The SNP-MAP controller maintains the SNP infusion rate at 1.763 ± 0.28 μg kg–1 min–1.

Results of FNN control system of SNP infusion for regulating the high MAP under different SNP sensitivities:
Figure 3B shows the performance of FNNC for high SNP sensitivity case. At t = 2.67 min, undershoot of MAP response is observed (115.5 mmHg) within the acceptable range by SNP infusion rate (1.72 μg kg–1 min–1). The SNP infusion is smoothly decreased to 0.935 ± 0.243 μg kg–1 min–1 which produces the desired convergence of MAP to 120.4 ± 4.25 mmHg in 3.97 min. For low SNP sensitivity, the MAP is reduced to 122.67 ± 4.87 mmHg in 5.44 min, see Figure 3C.
Simultaneous infusions of SNP and DPM are used for CHF therapy as depicted in Figure 4. In Figure 4A, the dropped CO is increased from 1.5 L min–1 to 1.76 ± 0.172 L min–1 in 8.2 min under normal SNP sensitivity. The DPM infusion shows a maximum rate of 5.2 μg kg–1 min–1 at t = 8.573 min to raise the CO rapidly to the acceptable level. In consequence, the MAP is also increased to 104 mmHg. Therefore the infusion rate of SNP is activated (1.1 ± 0.78 μg kg–1 min–1) and decreases the MAP to 100.5 ± 1.58 mmHg in 5.56 min.

Results of FNN infusion control of SNP and DPM infusion for a patient with CHF under different SNP sensitivities:
Figure 4B and 4C show the response of hemo-dynamic variables under high and low SNP sensitivities respectively. In both cases, the CO response and DPM infusion rate are approximately similar to the normal case. However, the total amount of DPM consumption in high sensitivity (147.4 μg) is larger than the low sensitivity (141.5 μg). In high SNP sensitivity case, the SNP infusion rate of 0.28 μg kg–1 min–1 is injected, when the MAP increased slightly over the desired level. Therefore a small hypotension of MAP occurred at 97.6 mmHg. But the DPM infusions rate elevates again the MAP level to 102.4 mmHg and keeps the CO at the healthy setpoint. The MAP is then regulated again by a small SNP infusion rate (0.62 ± 0.42 μg kg–1 min–1), reducing the MAP to 99.78 ± 1.15 mmHg in 3.07 min. On the other hand, the CO shows 3.0% overshoot (1.94 L min–1 at t = 9.58 min) under low SNP sensitivity, therefore the DPM infusion is decreased rapidly to 2.0 μg kg–1 min–1. High SNP infusion rate (2.01 ± 1.36 μg kg–1 min–1) is required to decrease the MAP to 100.94 ± 1.35 mmHg as shown in Figure 4C.
Figure 5 shows the evaluation results of different fuzzy controllers for regulating high MAP via SNP infusion under different SNP sensitivities. The developed FNNC achieved the lowest errors of controlling MAP (RMSE ≤ 5.56 mmHg) for all hypertension conditions (see Fig. 5A). Although the settling times using SFLC are shorter than that of STS fuzzy PID and FNN controllers as shown in Figure 5B, SFLC failed to minimize the RMSEs of MAP under all SNP sensitivities. Figure 5C shows no significant difference among three fuzzy controllers using the same amount of SNP drug.

Evaluation results of MAP by using fuzzy controllers of SNP infusion for short-term hypertension therapy under different SNP sensitivities:
Figures 6 and 7 depict the evaluation results of closed-loop drug infusion fuzzy controllers to regulate CO and MAP, respectively, for patients with CHF. For improving the CO by using DPM infusion, the FNN control system successfully achieved the best values of RMSE ≤ 0.22 1/min, Ts ≤ 8.2 min and total infused amount of DPM ≤ 147.5 μg. On the other hand, STS fuzzy PID controller showed the best performance for regulating MAP with RMSE ≤ 2.26 mmHg for CHF conditions. However, FNNC showed slightly better performance of controlling MAP than SFLC with a relatively smaller injected amount of SNP.

Evaluation results of CO regulation by using fuzzy controllers of DPM infusion; namely SFLC, STS fuzzy PID and FNN controllers for a patient with CHF under different SNP sensitivities:

Evaluation results of MAP regulation by using different fuzzy controllers of SNP infusion for CHF therapy under different SNP sensitivities:
Discussion and Conclusion
This study demonstrated the feasibility of using an adaptive FNN controller for the administration of IV cardiac drugs in a closed-loop system. In hypertension therapy, the FNNC controls the SNP infusion rate to regulate the high MAP at desired levels. Although the action of FNNC caused a small hypotension in case of high SNP sensitivity, the MAP is still within the accepted range and is rapidly converged to the desired setpoint, see Figure 3B.
We have also shown that DPM and SNP infusion rates can be controlled simultaneously by using two separate sub-controllers of the FNNC for CHF therapy. A good regulation of CO is achieved with no significant overshoot in a short settling time. The infusion of DPM led to small overshoots of MAP within the accepted range; therefore the FNNC activated SNP infusion to pull down the MAP response to its nominal level as shown in Figure 4. Because of the effect of SNP infusion on CO a drop of DPM infusion rate occurred for one sample time interval under low SNP sensitivity of CHF, see Figure 4C. The developed infusion control system regulated successfully the hemodynamic variables for all hypertension and CHF conditions.
The main drawback of using SFLC is that the parameters of the membership functions must be tuned for each patient to handle time-varying responses of hemodynamic variables with or without the drug infusion. 17 STS fuzzy PID overcomes the limitations of using SFLC, but the parameters of PID in rule consequences need further tuning. 26
The FNN control system provides self-adaptation according to the health status of patient. The developed controller showed best results in controlling MAP and CO with a minimum amount of IV cardiac drugs.
To prepare the FNN control system for animal trials and clinical use, a supervisor should be incorporated with the drug infusion controller 33 to manage the overall conditions of the control system and avoid taking undesirable decisions such as sensor signal conditioning.
Under different conditions of hypertension and CHF therapy, the developed automated IV cardiac drug infusion system contributes successfully a new FNN controller for regulating the hemodynamic variables of left heart failure patients.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
List of Abbreviations
Acknowledgements
This work was partially supported by Faculty of Electronic Engineering, University of Menofia, 32952 Menouf, Egypt.