
Abstract
Background
Increasing evidence shows the importance of young age, estrogen receptor (ER), progesterone receptor (PR) status, and HER-2 expression in patients with breast cancers.
Patients and methods
We organized an analytic cross-sectional study of 105 women diagnosed with breast cancer who have been operated on between 2008 to 2010. We evaluated age, size, hormone receptor status, HER-2 and P53 expression as possible indicator of lymph node involvement.
Results
There is a direct correlation between positive progesterone receptor status and being younger than 40 (
Conclusions
Although negative progesterone receptor tumors were more likely to have HER-2 overexpression, it is possible that higher stage and larger size breast cancer in younger women is related to positive progesterone receptor status.
Introduction
The world's most common cancer and the second main cause of cancer death among women in the United States is breast cancer. 1 The mean age at diagnosis is about 63 years in the United States and Western Europe, while it is around 51 years in Iran.
Studies show that the breast cancer in younger women is unique and needs a different treatment strategy than what might be used for older women with breast cancer.2–5
Since breast cancer in older women is more common, they have usually been the centre of attention so the most breast cancer studies have focused on older women. 6
According to many studies breast cancer in younger age groups tends to be more advanced and more aggressive than older age groups.2–5,7,8 Also breast tumors in younger age groups were more likely to be of higher grade, hormone receptor–negative, poorly differentiated, and aneuploid, and to have high S-phase fraction, abnormal expression of P53, greater extent of lymphovascular invasion, and overexpression of human epidermal growth factor receptor 2 (HER-2) than breast tumors in older age groups.2–5
Local recurrence in women younger than 45 was found to be four times more frequent than in women older than 65. 9 In another retrospective study, local recurrence rate was 38% at 10 years, and relative risk of locoregional recurrence increased by 7% for every decreasing year of age in women younger than 40 who were treated with a primary breast-conserving operation followed by adjuvant radiation with or without chemotherapy. 10 In that study, the only prognostic factor for locoregional recurrence was young age. The reason of poor local recurrence in women younger than 40 in comparison with women older than 40 is still unclear and not fully understood.
Clinically, breast cancer in younger women that are diagnosed with a palpable mass have larger tumor sizes, more lymph node metastasis and are more invasive cancers than those in older women.2,7,8
Metastasis to the lymph nodes is an important prognostic factor, which indicate advanced disease status with the probability that cancer cells have spread to distant sites. At diagnosis, 30% to 50% of all breast cancers have spread to the sentinel lymph node.11–13
Patients and Methods
The study population consisted of 105 patients with unilateral breast cancer treated by modified radical mastectomy with axillary dissection from August 2008 until March 2010 at the Imam Reza and Shams Medical Centers in Tabriz. All types of histologically confirmed invasive carcinoma were included.
The information was extracted retrospectively and included patient age, tumor size, stage, histologic type, estrogen and progesterone receptor status, P53, and HER-2 expression. Each of these factors was separately evaluated for correlation with lymph node involvement and degree of positivity defined as number of nodes with metastases.
All analyses were done in a single laboratory using the same method, eliminating the problem of inter laboratory differences. Patients were divided into two age groups: <40 years and ≥40 years.
Patient and tumor characteristics of age, tumor size in cm (≤2 or T1, 2 to 5 or T2, ≥5 or T3, and T4), number of nodes involved (none or N0, one to three or N1, four to nine or N2, more than ten or N3, and unknown), stage (I, II, III, IV, and unstaged), estrogen receptor (ER), progesterone receptor (PR) (positive and negative), P53 expression, HER-2 expression (positive and negative), and laterality were recorded. Tumor size was measured from the largest diameter in the gross specimen.
Hormone receptors were considered negative when concentration was below 10%. P53 was considered positive when nuclear staining was positive in more than 10% of tumoral cells. HER-2/neu overexpression was considered positive when complete and intense membrane staining was observed in more than 10% of tumoral cells.
The chi-square test was used for statistical analysis for categorical variables. If the expected number in any cell of the 2 × 2 contingency table was less than five, Fischer's exact test was used. As the analysis involves multiple subgroups, significance was set at the 5% level (
Our study was in accordance with rules and regulation of the ethics committee of Tabriz University of Medical Sciences, and because the study was a retrospective one, the IRB approval was not required.
Results
The distribution of patients by age classifications was as follows: 18 patients (17.1%) were younger than 40 years old, and 87 patients (82.8%) were 40 years and older.
Mean age at diagnosis in the younger women was 34 years (range 27 to 39 years) compared with a mean age of 53 years in the older women (range 40 to 80 years).
Stage distribution of the tumors was as follows: Stage I: 13 patients (12.3%), stage II: 40 patients (38.1%), stage III: 47 patients (44.7%), stage IV: 3 patients (2.8%) and unstaged: 2 patients (1.9%).
Tumor characteristics in younger women also were significantly different from tumor characteristics in older women. Younger women had tumors that were more likely to have higher stage, larger size, and progesterone receptor positive (

Younger women had tumors that were more likely to have higher stage (
Tumor characteristics of the study population.

77.7% of the younger women had positive lymph nodes, as compared to 56.3% of the older women. Although this difference was not significant (
14 (77.7%) of 18 patients younger than 40 years old had positive progesterone receptor compared with 49 (56.3%) of 87 patients 40 years and older. The differences were statistically significant (
The most common histologic finding was invasive ductal carcinoma, involving 92 patients (87.6%). 55 patients (59.7%) with this histology had lymph node metastasis compared to 8 out of 13 patients (61.5%) with mixed cell and other carcinomas. The differences were not significant (
34 out of 57 estrogen receptor positive patients (59.6%) had lymph node involvement; 29 out of 48 estrogen receptor negative patients (60.4%) had involved nodes, and the difference was not statistically significant (
36 out of 63 progesterone receptor positive patients (57.1%) had lymph node involvement compared with 27 out of 42 progesterone receptor negative patients (64.2%). The relation between lymph node involvement and progesterone receptor status were not statistically significant (
Statistical associations between lymph node status with size, histology, and hormone receptor status.

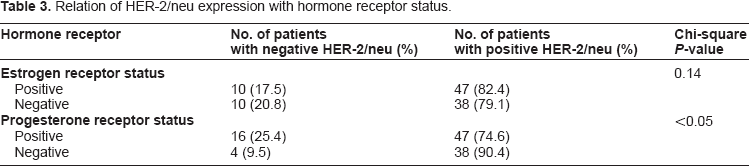
We investigated the relation between progesterone receptor status and positive HER-2/neu. 38 out of 42 patients (90.4%) with negative progesterone receptor status had positive HER-2/neu, while progesterone receptor positive patients that had positive HER-2/neu were 47 out of 63 patients (74.6%). Negative progesterone receptor status was associated with HER-2 overexpression and this relation was statistically significant (
Relation of HER-2/neu expression with hormone receptor status.
A significant correlation was not found between the positive lymph nodes, size, or stage with estrogen receptor, progesterone receptor status, P53, or HER-2/neu expression.
Discussion
Breast cancer risk increases with age. In the United States it is estimated that 5% to 7% of breast carcinomas are presented in women younger than 40 years old, 14 while in our study it is about 17%. The cause of this high percentage compared to the United States may be due to a large young population in Iran, or there may be genetic and environmental factors.
Clinically, the relation between tumor size and lymph node involvement is well known 15 and it is the only most powerful indicator of poor prognosis in breast cancer.16,17 Pathologic data consisting of patients with breast cancer shows that, at diagnosis, presence of tumor-infiltrated lymph nodes is common, with estimates ranging from 30% to 50% of cases, depending on tumor size.11,13
The younger women had tumors that were clearly different from tumors in older women and were characterized by unfavorable biologic parameters. The result of our research accounts for the significant within-stage disparity between the younger and older women. The majority of tumors in younger women had positive progesterone receptor and higher stage. There is a relation between all of these features and more aggressive tumors and poorer prognosis. Another analysis also found that tumors in young women have lower ER positivity, higher HER-2/epidermal growth factor receptor expression, and a trend toward inferior disease-free survival. 5 All of these studies support the concept that tumors developing in younger women are biologically different from tumors in older women and tend to be more aggressive with unfavorable biologic markers.
Many studies from Europe and America have been reported showing that young age at diagnosis is as an independent predictor of poor survival.18–22 The risk factor profile in young women is worse than older women. Young women had a tendency to have larger tumor sizes, more positive lymph nodes, more negative hormone receptors, higher tumor grades than older women.2,4,21,23,24 This issue remains controversial, as in a retrospective study of breast cancer patients from Singapore Chia et al suggested that young women with breast cancer had a better survival than older females. 25 It is also in contrast to our study's finding that younger women were more likely to have progesterone receptor positive tumors. Moreover according to our results negative progesterone receptor tumors had a tendency to have HER-2 overexpression.
As in our study, Winstanley et al 26 have not found a significant association between estrogen or progesterone receptor and lymph node status.
Conclusion
Breast cancer in younger age groups is more aggressive than in older age groups. Although negative progesterone receptor tumors were more likely to have HER-2 overexpression, different biologic behavior of breast cancer in younger age groups may be due to progesterone receptor positive status.
Additional studies should focus on association between hormone receptor status, HER-2 expression, and lymph nodes metastasis.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgments
This paper is an adaptation of corresponding author's thesis submitted for specialty degree in General Surgery (thesis number 88/3-5/3).