
Abstract
Purpose and Methods
Our secondary analyses compared survival with eribulin versus capecitabine in various patient subgroups from a phase 3, open-label, randomized study. Eligible women aged ≥18 years with advanced/metastatic breast cancer and ≤3 prior chemotherapies (≤2 for advanced/metastatic disease), including an anthracycline and taxane, were randomized 1:1 to intravenous eribulin mesylate 1.4 mg/m2 on days 1 and 8 or twice-daily oral capecitabine 1250 mg/m2 on days 1–14 (21-day cycles).
Results
In the intent-to-treat population (eribulin 554 and capecitabine 548), overall survival appeared longer with eribulin than capecitabine in various subgroups, including patients with human epidermal growth factor receptor 2-negative (15.9 versus 13.5 months, respectively), estrogen receptor-negative (14.4 versus 10.5 months, respectively), and triple-negative (14.4 versus 9.4 months, respectively) disease. Progression-free survival was similar between the treatment arms.
Conclusions
Patients with advanced/metastatic breast cancer and human epidermal growth factor receptor 2-, estrogen receptor-, or triple-negative disease may gain particular benefit from eribulin as first-, second-, and third-line chemotherapies.
Trial Registration (Primary Study)
This study reports the subgroup analyses of eribulin versus capecitabine from a phase 3, open-label, randomized study (www.clinicaltrials.gov; ClinicalTrials.gov identifier: NCT00337103).
Keywords
Introduction
Chemotherapy is an integral part of management of patients with breast cancer, either alone or in combination with other agents. While many chemotherapy options are available for patients with pretreated metastatic breast cancer (MBC), their optimal sequence is unclear with hitherto limited data from randomized trials.1,2 Despite recent advances, the five-year survival rate in patients with advanced/MBC is around 25%, with over 40,000 patients expected to die from the disease in the United States (US) alone in 2015. 3 There remains, therefore, a major unmet need for effective, well-tolerated therapeutic options with a robust evidence base for the treatment of advanced/MBC.
Eribulin mesylate is a microtubule dynamics inhibitor belonging to the halichondrin class of antineoplastic agents.4,5 Recent preclinical data suggest that eribulin may also have effects on vascular remodeling, the reversal of epithelial– mesenchymal transition, and suppression of cell migration and invasion.6,7 Eribulin is approved for the treatment of advanced or MBC in patients who have received at least one (European Union [EU]) or two (US) prior chemotherapy regimens for metastatic disease, including an anthracycline and a taxane in either the adjuvant or the metastatic setting.8,9 Approval is based primarily on results from Study 305/EMBRACE, a phase 3, randomized study in which eribulin was associated with a significant improvement in overall survival (OS) compared to the treatment of physician's choice (13.2 versus 10.5 months, respectively; hazard ratio [HR]: 0.81 [95% confidence interval (CI): 0.67, 0.96];
More recently, Study 301 compared the efficacy and safety of eribulin versus capecitabine as first-, second-, or third-line treatment in 1102 women (eribulin 554 and capecitabine 548) with locally advanced or MBC who had received prior anthracycline-and taxane-based chemotherapies.
11
In this study, eribulin achieved a numerically longer OS than capecitabine (15.9 versus 14.5 months, respectively; HR: 0.88 [95% CI: 0.77, 1.00];
Given these findings, practicing oncologists and their patients may want to understand whether specific patient subgroups could derive greater benefit from eribulin. Here, we assess the efficacy of eribulin compared to capecitabine in Study 301 across a range of subgroups, including those with human epidermal growth factor receptor 2 (HER2)- and triple-negative disease status.
Methods and Statistics
Patients
Patient eligibility criteria have been reported previously. 11 Briefly, these included females (aged ≥18 years) with histologically or cytologically confirmed locally advanced or MBC, ≤3 prior chemotherapy regimens (including ≤2 for advanced and/or metastatic disease), including an anthracycline and a taxane. HER2-targeted therapy was not allowed during study treatment.
As part of the original study (Kaufman et al, 201511), all patients provided written informed consent and the primary study protocol was approved by all relevant review bodies. Because these analyses use existing data from the Kaufman primary study, additional consent was not sought for these analyses. The study was conducted in accordance with the Declaration of Helsinki, guidelines of the International Conference for Harmonization/Good Clinical Practice, and local requirements.
Study Design
This was an international, phase 3, open-label trial (study number E7389-G000–301; clinicalTrials.gov identifier: NCT00337103). Patients were stratified by geographic region (Latin America, Western Europe/Australia, Eastern Europe, North America, Asia, or South Africa) and HER2 status (positive, negative, or unknown). 11 Patients were randomized (1:1) to receive eribulin mesylate 1.4 mg/m2 (equivalent to 1.23 mg/m2 eribulin [expressed as free base]) intravenously over two to five minutes on days 1 and 8 or capecitabine 1.25 g/m2 orally twice daily on days 1–14, both in 21-day cycles, until disease progression, unacceptable toxicity, or patient/investigator request to discontinue.
Study Objectives and Subgroup Analyses
The coprimary endpoints were OS and PFS; the secondary endpoints were objective response rate, duration of response, one-, two-, and three-year survival, and quality of life. These have been reported previously. 11
Prespecified analyses were performed based on (i) patient demographics, (ii) receptor status, and (iii) disease status.
Patient demographics included analyses based on age groups (≤40, >40 to <65, and ≥65 years) and geographic region of treatment. Receptor status analyses were based on the status of HER2 (positive, negative, or unknown), estrogen receptor (ER; positive, negative, or unknown), hormone receptor (positive [ER-positive and/or progesterone receptor (PR)-positive], negative [both ER-negative and PR-negative], or unknown), and triple-negative (ER-negative, PR-negative, and HER2-negative) disease. Analyses by disease status involved the number of prior chemotherapy regimens for advanced/metastatic disease (0 and ≥1); sites of disease (visceral or nonvisceral only); number of organs involved (≤2 and >2); setting of prior anthracycline and taxane therapy (both received as adjuvant therapy versus at least one received as treatment for metastatic disease); and patients whose disease was taxane resistant having progressed within 60 days after the last dose of the taxane.
A nonprespecified sensitivity analysis was previously requested by the EU health technology assessment authority based on the ER status and number of organs involved. In view of subsequent approval by the European Medicines Agency for eribulin in women who have received at least one prior line of chemotherapy for advanced/metastatic disease, further nonprespecified post hoc analyses were carried out in patients treated in this setting. These included analyses by HER2 status, ER status, triple-negative breast cancer, number of organs involved (≤2 and >2), presence of visceral disease, and disease progression within 60 days of the last dose of taxane.
Statistical Analyses
Subgroup analyses were carried out using the same general approach (ie, statistical model, missing data handling, and censoring rules) as the primary analysis.
11
The HRs of eribulin versus capecitabine for OS and PFS were estimated in stratified Cox regression models with HER2 status and region as stratification factors. Stratified log-rank tests were used to obtain
Results
Patients
Overall, 1102 patients in the intent-to-treat (ITT) population (see Supplementary Fig. 1) were randomly assigned to eribulin (
Forest plots of (
Prespecified Efficacy Analyses
Patient Demographics
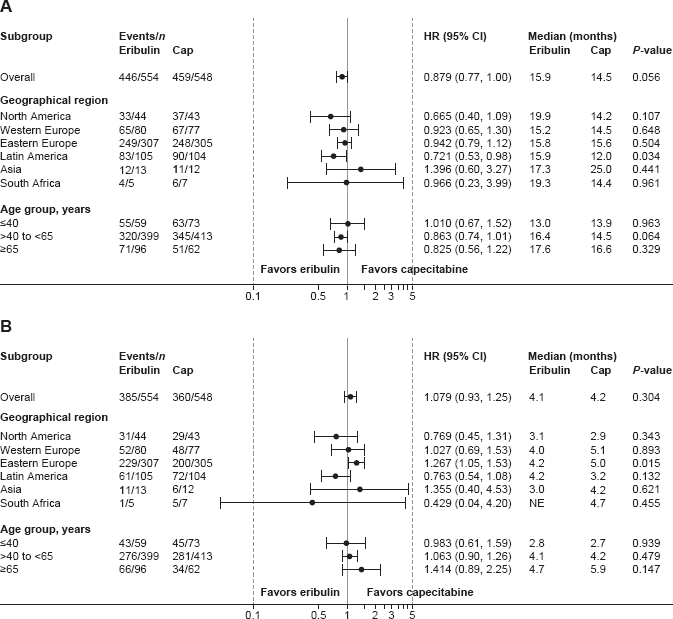
OS and PFS between the two treatment arms were similar across the age groups studied (Fig. 1). Comparison by geographic region found similar OS in both treatment arms, with the exception of patients treated in Latin America who appeared to have longer OS with eribulin than capecitabine (15.9 versus 12.0 months;
PFS was similar between the treatment arms, with the exception of apparently greater benefit from capecitabine than eribulin in patients treated in Eastern Europe (5.0 versus 4.2 months;
Receptor Status
OS was longer with eribulin compared to capecitabine in patients with HER2-negative (15.9 versus 13.5 months, respectively; HR: 0.84 [95% CI: 0.71, 0.98]; Forest plots of (
Disease Status
In total, 882 of 1102 (80.0%) patients in the ITT population (eribulin, Forest plots of (
In the overall patient population, longer OS (
Nonprespecified Efficacy Analyses
ITT Population
The potential benefit of eribulin versus capecitabine is supported by the sensitivity analysis requested by EU regulators using the Cox model adjusted for the number of organs involved and ER status (15.9 versus 13.5 months, respectively; HR: 0.81 [95% CI: 0.69, 0.95];
Sensitivity Analyses in Patients with ≥1 Prior Chemotherapy Regimens in the Metastatic Setting
Within this group of patients, the majority had received eribulin or capecitabine as second-line therapy (63.9% and 66.0%, respectively), the remainder receiving them in the third-line or later setting. OS was similar with eribulin and capecitabine in patients who had received ≥1 prior chemotherapy regimen (16.0 versus 14.5 months, respectively; HR: 0.87 [95% CI: 0.75, 1.01]; Forest plot of OS in patients who received eribulin after one or more prior chemotherapy regimens for advanced disease.
To allow for the impact on OS of the large treatment effects in patients with ER-negative disease and those with >2 organs involved, a further sensitivity analysis was conducted, adjusting the statistical model for these effects. In these analyses, median OS in the overall population was in favor of eribulin compared to capecitabine (16.0 versus 14.5 months; HR: 0.82 [95% CI: 0.71, 0.95];
Discussion
In light of the observed survival benefit seen in Study 305/EMBRACE,
10
eribulin is recommended by all major guidelines for the treatment of patients with advanced/MBC.1,2,12 As reported previously, eribulin was not statistically superior to capecitabine in Study 301 in terms of OS or PFS, although a numerical improvement in OS was seen with eribulin compared to capecitabine (
In prespecified analyses of well-known prognostic factors, improvement in OS appeared to be seen in some subgroups with eribulin compared to capecitabine. In particular, median OS was longer in patients with HER2-, ER-, and triple-negative disease receiving eribulin versus capecitabine (by 2.4, 3.9, and 5.0 months, respectively; all
A potential survival advantage was suggested in patients with nonvisceral disease and those with >2 organs involved receiving eribulin compared to capecitabine (9.5 and 3.3 months longer OS, respectively;
A small increase in OS (1.5 months) with eribulin versus capecitabine was observed in patients who had received ≥1 prior chemotherapy regimen for advanced/metastatic disease. Additional analyses suggested that eribulin prolonged OS compared to capecitabine in several subgroups, including those with HER2-, ER-, and triple-negative disease. These findings provide clinicians and patients with additional evidence specific to the patient population now approved in the EU and elsewhere (but not in the US) for treatment with eribulin.
Similar to the primary analysis of this study 11 and the EMBRACE study, 10 eribulin consistently had a greater impact on OS than PFS. This may, at least in part, be attributable to the phenotypic changes and/or eribulin-induced changes in tumor phenotype and vasculature observed in preclinical models, which may enhance the efficacy of subsequent therapies6,7 and improve outcomes. Further translational studies are needed to confirm these preclinical findings.
A limitation of these analyses is that all
Conclusions
In this subgroup analysis, eribulin was an effective therapeutic option for the treatment of patients with advanced/MBC and may especially benefit those with HER2-negative, ER-negative and triple-negative disease. These data in patients treated in the first-, second-, and third-line settings support eribulin as an active single agent for patients with advanced/MBC who have received prior chemotherapy, including an anthracycline and a taxane.
Author Contributions
Contributed to the study conception and design: CT, JC, CED, and PAK. Contributed to the collection of data: CT, AA, JC, LY, CED, MSO, GV, and PAK. Had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis: GV, JS. All authors contributed to the writing and development of the article. All authors reviewed and approved of the final manuscript.
Supplementary Materials
Supplementary Figure 1
CONSORT diagram for Study 301 (NCT00337103).
Supplementary Figure 2
Kaplan–Meier curve for OS in HER2-negative patients (ITT population).
Supplementary Figure 3
Kaplan–Meier curve for OS in patients with triple negative breast cancer (ITT population).
Supplementary Figure 4
Forest plot of OS in patients who received eribulin after one or more prior chemotherapy regimens for advanced disease: additional analysis model.
Supplementary Table 1
Patient demographics and baseline characteristics (ITT population).
Supplementary Table 2
PFS for Study 301 in patients who received eribulin after one or more prior chemotherapy regimens for advanced disease.
Footnotes
Acknowledgments
We thank all the patients and investigators who participated in this study (refer to Kaufman et al 11 for the full list). We would also like to thank Liang Liu, PhD, of Eisai Inc. and Yi He, PhD, formerly of Eisai Inc., for statistical analyses and Erhan Berrak, MD, for thoughtful discussions and guidance during article development.