
Abstract
Introduction
Breast magnetic resonance imaging (MRI) is considered a more sensitive diagnostic test for detecting invasive breast cancer than mammography or breast ultrasound. Breast MRI may be particularly useful in younger premenopausal women with higher density breast tissue for differentiating between dense fibroglandular breast tissue and breast malignancies. The main objective of this study was to determine the impact of preoperative breast MRI on surgical decision-making in young women with breast cancer.
Methods
A retrospective review of patients with newly diagnosed invasive breast cancer and age of ≤50 years was performed. All patients underwent physical examination, preoperative mammogram, breast ultrasound, and bilateral breast MRI. Two breast cancer surgeons reviewed the preoperative mammogram report, breast ultrasound report, and physical examination summary and were asked if they would recommend a lumpectomy, a quandrantectomy, or a mastectomy. A few weeks later, the two surgeons were shown the same information with the breast MRI report and were asked what type of surgery they would now recommend. In each case, MRI was classified by two adjudicators as having affected the surgical outcome in a positive, negative, or neutral fashion. A
Results
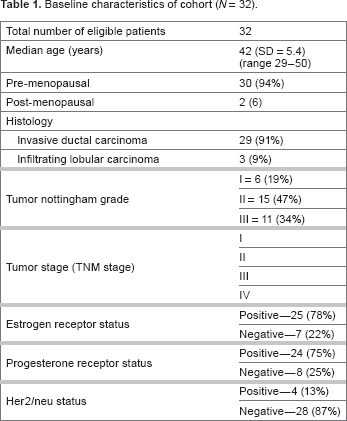
Of 37 patients whose charts were reviewed, five patients were deemed to be ineligible due to having received neoadjuvant chemotherapy, having previous breast implants, or having had their tumor fully excised during biopsy. In total, 32 patients met the inclusion criteria of this study and were appropriate for analysis. The median age of our study patient population was 42 years. The pathologic diagnosis was invasive ductal carcinoma in 91% (29/32) of patients and invasive lobular carcinoma in 9% (3/32) of patients. For surgeon A, clinical management was altered in 21/32 (66%) patients, and for surgeon B, management was altered in 13/32 (41%) patients. The most common change in surgical decision-making after breast MRI was from breast-conserving surgery to a mastectomy. Mastectomy rates were similar between both surgeons after breast MRI. After reviewing the pathology results and comparing them with the breast MRI results, it was determined that breast MRI led to a positive outcome in 13/32 (41%) patients. Breast MRI led to no change in surgical management in 15/32 (47%) patients and resulted in a negative change in surgical management in 4/32 (13%) patients. Bilateral breast MRI detected a contralateral breast cancer in 2/32 (6%) patients.
Conclusions
Preoperative breast MRI alters surgical management in a significant proportion of younger women diagnosed with breast cancer. Prospective studies are needed to confirm these findings and to help determine if this change in surgical decision-making will result in improved local control.
Introduction
Breast cancer is the most common cancer affecting women, with over 23,000 patients diagnosed in Canada each year. 1 The usual preoperative work-up for a suspected breast mass includes clinical breast and lymph node examination, mammography, breast ultrasound, and biopsy of the lesion in question. Following the pathologic confirmation, women with early-stage breast cancer are seen by their surgeon for a discussion regarding breast-conserving surgery versus mastectomy.
Breast magnetic resonance imaging (MRI) has been shown to be a more sensitive preoperative staging technique for detecting invasive breast cancer than mammography and/or breast ultrasound. 2 However, over the past few years, the introduction of preoperative breast MRI into the clinical setting has led to some controversy regarding its role in staging patients with early-stage breast cancer.
Young women (age less than or equal to 50 years) account for approximately 25% of all newly diagnosed breast cancers. 3 These women tend to have breast cancers that are associated with a worse prognosis than their older counterparts, including higher local recurrence rates and worse overall survival.4,5 One potential explanation for this phenomenon is that younger women tend to have higher risk tumor features, including larger tumor size, higher tumor grade, and a higher incidence of human epidermal growth factor receptor 2 (HER2)-positive disease. 6 In addition, most breast cancers in young women are identified by patients themselves, and they tend to present at a more advanced stage than women over the age of 50 years. 4 Young women also tend to have more fibroglandular breast tissue and a higher mammographic density, which makes it more difficult for mammography to differentiate normal breast tissue from a new breast cancer. 7 Breast MRI may be able to better differentiate between dense breast tissue and actual breast cancers in young women compared to routine mammography and breast ultrasound based on the tumor enhancement characteristics.8–10
In this retrospective study, we studied young women with early-stage breast cancer who underwent a preoperative bilateral breast MRI and asked surgeons what type of surgery they would recommend before and after being shown the breast MRI results. We hypothesized that the preoperative breast MRI in young women aged ≤50 years would result in a significant change in surgical recommendations.
Methods
A retrospective review of women aged ≤50 years with newly diagnosed invasive breast cancer treated between November 2004 and March 2008 at the Juravinski Cancer Centre, St. Joseph's Hospital, and the Henderson Hospital was performed. Patients were included for review if they had undergone a preoperative physical examination, preoperative mammogram, breast ultrasound, and bilateral breast MRI followed by definitive surgery. Patients were excluded if they had received neoadjuvant chemotherapy, had preexisting breast implants, or if their tumor had been completely excised during the initial biopsy. The mammogram and breast ultrasound could have been performed at a community hospital or diagnostic center; however, the breast MRI had to have been performed at either St. Joseph's Hospital or the Henderson (now named Juravinski) Hospital.
Two breast cancer surgeons initially reviewed the reports of the preoperative physical examination, mammogram, and breast ultrasound and were asked which type of surgery they would recommend based on this information: a lumpectomy, a quandrantectomy (more extensive lumpectomy), or a mastectomy. Several weeks later, both surgeons were shown the patient's preoperative breast MRI report in addition to the same radiological reports as before and were again asked to select which type of surgery they would recommend using this new MRI information. Following this, two adjudicators reviewed each case in detail to determine if the preoperative breast MRI would have had a positive impact, a negative impact, or no impact (Fig. 1) on the surgical procedure chosen based on the following definitions.
CONSORT diagram.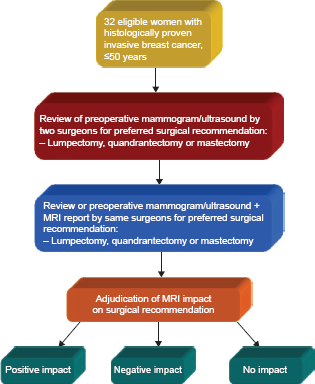
Positive impact: breast MRI detected additional disease that was not found on physical examination, mammogram, or breast ultrasound and led to an appropriate change in surgical management.
Negative impact: breast MRI led the surgeon to recommend more extensive surgery, with less extensive disease actually found at pathology.
No impact: breast MRI findings coincided with other imaging tests and did not significantly alter surgical recommendations or outcomes.
It should be noted that all patients in this study had previously undergone definitive surgical treatment for their breast cancer. The purpose of this study was to retrospectively determine whether the preoperative breast MRI would have actually changed the surgical decision-making. Based on the final pathology results and preset definitions, it was then determined whether the preoperative breast MRI resulted in a positive, negative, or neutral change in the surgical recommendations (see Fig. 1 for the CONSORT diagram).
Sample Size
The primary outcome was the proportion of patients for which preoperative breast MRI would result in a change in surgical management. Based on the literature, we estimated conservatively that this proportion was expected to be approximately 20%. To have a 0.3 (30%) width in the 95% confidence interval of this estimate, 32 patients were required for this retrospective study. The confidence interval was estimated by the Clopper–Pearson method. 11
Mammography Technique
All patients had bilateral diagnostic mammogram and additional views as required available for review. Mammograms were obtained through our diagnostic imaging department and were performed using the full-field digital mammogram systems, 2000D unit (Senographe; GE Medical Systems). The images were read using a dedicated GE system Mammo-Viewer. Any mammograms performed outside the institution were also loaded onto the Mammo-Viewer workstation in DICOM format for review (Seno Advantage 2.2; GE Medical Systems).
MRI Technique
Breast MRI acquisition was performed using a 1.5-T whole body system with a bilateral breast surface coil. Dynamic MRI measurements were performed before and after intravenous gadolinium 0.1 mmol/kg weight contrast. Breast MRI sequences included pre- and postgadolinium-enhanced contrast imaging. Postcontrast sequences were obtained within 60 seconds of injection followed by a total of five sequences at one minute intervals. The postimage processing included image subtraction, temporal enhancement curves for lesions, and maximum intensity projection images. Breast MRI result was interpreted by radiologists based on guidelines published by the American College of Radiology. 12
Physician Involvement
Three radiologists from St. Joseph's Hospital and the Henderson Hospital interpreted all preoperative breast MRI results of patients in this retrospective review. Two surgical oncologists (surgeon A and surgeon B) specializing primarily in breast cancer surgery participated in the study. Tissue processing and histopathology performed on all breast cancer specimens were evaluated by pathologists with expertise in breast cancer. The two adjudicators involved in this study included a medical oncologist and a clinical research coordinator, both with interests in breast cancer research.
Ethics
This study was approved by the Research Ethics Board of the Hamilton Health Sciences.
Results
Baseline characteristics of cohort (
The addition of preoperative breast MRI would have resulted in a change in clinical management in 21/32 (66%) patients for surgeon A in 14/32 (44%) patients for surgeon B. The most common change in surgical recommendation was from lumpectomy or quadrantectomy to mastectomy due to more extensive disease identified on the preoperative breast MRI (see Fig. 2). Mastectomy rates were similar for both surgeons A and B after the breast MRI results were available.
Change in surgical recommendations following access to breast MRI reports.
Impact of Preoperative Breast MRI
Using the definitions of impact described in the “Methods” section, the two adjudicators determined that breast MRI led to a positive impact on surgical management in 14/32 (44%) patients, no impact in 14/32 (44%) patients, and a negative impact in 4/32 (12%) patients (see Fig. 3). For cases where preoperative breast MRI had a positive impact on surgical management, the most common scenario was that breast MRI detected additional disease not seen on mammography or breast ultrasound, which was confirmed at pathology following the surgery. In these cases, the preoperative breast MRI led the surgeon to appropriately recommend more aggressive breast cancer surgery. We found that 28% (surgeon A) and 47% (surgeon B) of patients in our study had their surgical recommendation changed from breast-conserving surgery to mastectomy after being shown the preoperative breast MRI.
Impact of preoperative breast MRI on surgical management.
In total, 12/32 patients were found to have additional disease found on breast MRI and confirmed at pathology in the ipsilateral breast with 2/32 patients in the contralateral breast. Images from a patient who underwent preoperative breast MRI and was found to have a contralateral breast cancer and more extensive disease in the ipsilateral breast compared to the initial mammogram are shown in Figure 4.
Contrast-enhanced preoperative breast MRI in a 36-year-old patient with bilateral breast cancers. Breast MRI shows more extensive multifocal disease in the left breast on two minutes subtracted postcontrast axial imaging compared to initial mammogram (not shown here). There is also contralateral disease in the right breast (arrow), which was detected only by breast MRI and not on mammogram or ultrasound. All findings were confirmed with pathology following definitive surgery.
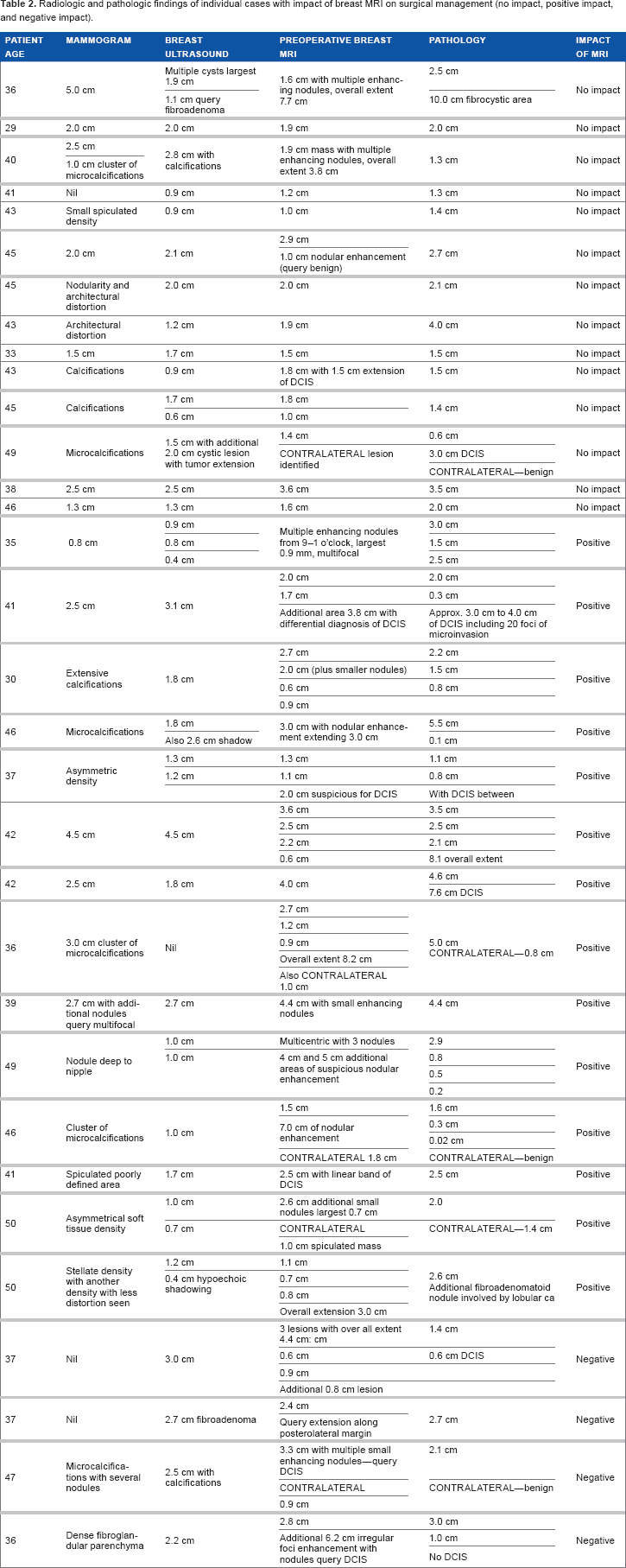
Radiologic and pathologic findings of individual cases with impact of breast MRI on surgical management (no impact, positive impact, and negative impact)
Ipsilateral Breast Biopsies
None of the patients in this study underwent additional ipsilateral MRI-guided breast biopsies in this study.
Contralateral Breast Biopsies
A total of 4/32 patients had a suspicious contralateral breast abnormality detected on bilateral breast MRI. This led to a biopsy of the contralateral breast in each case; however, of the four patients, only two patients were found to have a contralateral breast cancer. Bilateral breast MRI detected contralateral breast cancer in 2/32 (6%) patients that were not detected by conventional imaging.
Discussion
This study confirms our original hypothesis that preoperative bilateral breast MRI in young women with breast cancer alters surgical management in a significant proportion of patients. This finding is in agreement with several other retrospective and prospective studies evaluating the use of preoperative breast MRI in patients with newly diagnosed breast cancer;13–19 however, this is one of the first studies to specifically evaluate a younger patient population.
Houssami et al 20 have previously published a systematic review and a meta-analysis including 2160 women from 19 studies evaluating the accuracy and surgical impact of preoperative breast MRI on breast cancer patients of all ages. In this study, the proportion of patients undergoing a change in surgical management from breast-conserving surgery to modified radical mastectomy was 11.3% (95% confidence interval, 6.8–18.3). The median age of patients in each study included in the meta-analysis ranged from 49 to 60 years, with the majority of patients being over the age of 50 years. Additional tumor foci in the ipsilateral breast were found in 11%–31% of patients, and contralateral breast cancers were identified in 3%–6% of patients. 20
Despite the apparent benefits of performing preoperative breast MRI, there are also several potential limitations that should be considered. While breast MRI has been shown to be highly sensitive (>90%) in the detection of invasive breast cancer, its relatively low specificity (72%) can lead to diagnostic ambiguity in the preoperative setting.8,21,22 Abnormalities detected on preoperative breast MRI that are not detected on mammogram or breast ultrasound often need to be biopsied prior to surgery. One recent prospective study found that up to 10% of patients having a preoperative breast MRI will undergo a breast biopsy for benign disease. 23 Preoperative breast MRI and biopsies of additional lesions not found on routine preoperative mammography can result in delays to definitive breast cancer surgery. In addition, breast MRI is a costly diagnostic technique and a limited resource. It has been suggested that preoperative breast MRI might be leading the surgeons to perform more extensive breast cancer operations without any improvement in overall survival and no proven benefit in reducing the positive margin or local recurrence rates. 24
There is little debate that preoperative breast MRI leads to an increased detection of additional foci of occult cancer in the ipsilateral breast. However, there is a general lack of evidence demonstrating that it leads to improvements in either short- or long-term clinical outcomes, such as reoperation rate, local recurrence, or overall survival. 24 To date, the Comparative Effectiveness of MRI in Breast Cancer trial is the only randomized controlled trial that has compared outcomes in patients receiving preoperative breast MRI with those who did not. 25 This trial found no difference in the primary endpoint of re-excision rates, and disease-free survival was similar in both study arms with three years of follow-up. 25 However, longer follow-up will be necessary before making any definitive conclusions regarding the effect of preoperative breast MRI on local recurrence rate and other long-term outcomes. Another randomized controlled trial, MRI mammography of nonpalpable breast tumors examined whether MRI in addition to mammography and/or ultrasound would reduce the number of surgical procedures or core needle biopsies in patients with suspicious breast lesions. This study had a sample size of 418 patients and found that the addition of breast MRI to routine clinical care in patients with nonpalpable breast cancer was paradoxically associated with an increased re-excision rate due to the positive resection margins following breast-conserving surgery. 24 The authors concluded that breast MRI should not be used in the routine preoperative work-up of women with early-stage nonpalpable breast cancer. 24 This study, however, included women who were both pre- and postmenopausal.
Previously published data suggest that preoperative breast MRI increases the mastectomy rate by approximately 15%–20% in patients of all ages.20,26 Our study suggests that this rate could be even higher in younger patients. Although only two breast cancer surgeons took part in our small retrospective study, 28% and 47% of patients in our study had their surgical recommendation changed from breast-conserving surgery to mastectomy, which is significantly higher than what was originally anticipated. The percentage of patients whose surgical recommendation was changed from breast-conserving surgery to mastectomy was higher in our retrospective study evaluating younger women with breast cancer compared to other studies that focused mainly on women over the age of 50 years. However, our finding at this stage is hypothesis generating, and we hope to study this further in a prospective study of preoperative breast MRI in younger women. From a biological plausibility perspective, it does seem logical that breast MRI might have more of an impact in younger women with dense breast tissue compared to postmenopausal women who are more likely to have less dense breast tissue. Mammography is clearly beneficial in women over the age of 50 years, and it is quite possible that breast MRI might be able to identify more occult foci of disease in a younger patient with dense breasts than mammography and breast ultrasound.
A retrospective study by Godinez et al 27 evaluated the role of breast MRI in 79 women with early-stage breast cancer to determine the likelihood of finding additional disease in the same or other quadrants of the breast. The median age of patients in this study was 48 years. Of the 79 women in this study, 28 women were 40 years of age or younger. In these patients, the likelihood of finding additional disease in the breast was 50%, and 14.3% of these patients had disease in a separate quadrant of the breast compared to the original primary tumor. Another retrospective study by Petrillo et al 28 evaluated the role of preoperative breast MRI in 246 women less than 40 years of age. They found that patients who underwent a preoperative breast MRI had a 15% higher mastectomy rate compared to the patients who underwent conventional imaging alone (53% MRI group versus 38% non-MRI group). These studies are intriguing and suggest that further studies are warranted in premenopausal women regarding the role of preoperative breast MRI compared to conventional imaging alone. Our study has several limitations that need to be considered. Our sample size was small, and only two surgeons were included in our study. In addition, there could have been recall bias where surgeons participating in the study may have recalled their previous surgical recommendation in a particular patient based on the physical examination and radiological reports provided. Another limitation is the retrospective nature of our study that would prevent us from making causal inferences about the impact of preoperative breast MRI in premenopausal women with early-stage breast cancer on surgical decision-making. Instead, the results must be interpreted more as hypothesis generating.
Further prospective studies evaluating the role of preoperative breast MRI specifically in younger patients with breast cancer are recommended. Targeting this younger patient population is more likely to define a specific subgroup of patients who could benefit from such imaging prior to undergoing breast cancer surgery.
Author Contributions
Conceived and designed the experiments: SDM, NH. Analyzed the data: SDM, SC. Wrote the first draft of the manuscript: SDM, SC. Contributed to the writing of the manuscript: SDM, NH, PJL, KD, TM, SC, and JS. Agree with manuscript results and conclusions: SDM, NH, PJL, KD, TM, SC, and JS. Jointly developed the structure and arguments for the paper: SDM, NH, PJL, KD, TM, SC, and JS. Made critical revisions and approved final version: SDM, NH, PJL, KD, TM, SC, and JS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
This work has been presented in part at the San Antonio Breast Cancer Symposium (Mukherjee et al 2008, abstract # 1406).