
Abstract
Aims and Objectives
Breast positioning is the key factor affecting a mammogram. If care is taken during positioning, it maximizes the amount of breast tissue being imaged, eliminates most of the artifacts, and increases sensitivity of the mammogram. This retrospective study was carried out in our department to assess correctness, and also the incorrectness of breast positioning, which need to be avoided to obtain an ideal mammogram.
Material and Methods
A total of 1369 female patients were included in this study. Mammography was performed on full field detector digital mammography equipment. Craniocaudal (CC) view and mediolateral oblique (MLO) view were carried out for each breast. Four views were done for 1322 patients. The remaining 47 patients had undergone a mastectomy and underwent two views for the other breast. Mistakes in improperly positioned mammogram were assessed with respect to proper visualization of nipple, position of pectoralis major, pectoral–nipple distance (PND), inframammary fold, and adequate coverage of all breast quadrants.
Results
As per prescribed guidelines, mistakes in positioning were recognized in 2.879% of total mammograms. Improper positioning of the nipple was the commonest problem, seen in 3.827% of mammograms, CC view. On MLO view, bilaterally, pectoralis shadow was not seen in 0.520% mammograms, its margin was not straight/convex in 0.706%, lower edge of pectoralis was above pectoralis–nipple line in 2.081%, and inframammary fold was not seen in 1.189%. There was inadequate coverage of lower quadrants in 2.787%, and mismatch in PND was seen in 3.864%. In few of the patients, the shortcomings as a result of improper positioning were noted on one view, the rest being normal.
Conclusion
Positioning is the most important factor affecting the resultant mammography image. During mammography, many cases are improperly positioned and as a result the examination is inconclusive, which reduces the sensitivity of mammography.
Keywords
Introduction
The aim of mammography is to obtain an optimum image along with maximum breast tissue visualization. 1 There should be minimum discomfort to the patient. There are a number of factors that affect the clinical image quality of a mammogram. 2 These are positioning of the breast, compression, optimum exposure, sharpness, noise, and contrast. The quality of mammograms has improved remarkably after the introduction of digital mammography system. Also, strict quality assurance monitoring is being followed at present. With advancements in hardware and software, factors affecting image quality such as exposure, sharpness, noise, and contrast are being taken care of. The two factors that still affect the image quality are positioning and compression, both still being monitored by the operator.
Breast positioning is a key factor affecting a mammogram.3–5 Careful attention during patient positioning can eliminate most mammographic artifacts and increase the performance of mammography. Optimal positioning maximizes the amount of breast tissue seen on image. It has to be kept in mind that while positioning the patient, one has to position the whole of the body and not just the breast of the patient. Body habitus of each patient is different. It has to be assessed and adjustments made for maximum tissue visualization. Proper and adequate turning of the head of the patient for craniocaudal (CC) view and raising the arm for mediolateral oblique (MLO) view is very important. Care also has to be taken to prevent injury to the shoulder and the arm.
Another important factor that affects image quality of mammogram is compression. 1 Adequate compression separates overlapping structures. It improves the quality and details of a questionable pathology.
Failures in optimal positioning and appropriate compression are operator dependent. They can be avoided. Image quality can be improved by training and knowledge.
This retrospective study was carried out to evaluate the mistakes of improperly positioned mammograms that need to be avoided in order to ensure a high quality mammogram. The requirement for approval was waived by the local ethics committee due to the retrospective nature of the study.
Material and Methods
A total of 1369 female patients, who underwent mammography between January 2011 and December 2013 in our department, were included in this study. The patients with retraction of nipple, as mentioned on their history sheet, and post-operative mutilated breast were excluded.
We analyzed all mammograms irrespective of the indication for mammography, whether screening or diagnostic. In patients with history of mastectomy, mammogram of the other side was studied.
Mammography was performed on full field detector digital mammography equipment, Lorad Selenia by Hologic. CC and MLO views were carried out for each breast. Four views were done for 1322 females. The remaining 47 patients had undergone mastectomy and underwent two views for the breast on the other side. A total of 2691 CC and an equal number of MLO views were assessed. Mistakes in improperly positioned mammogram were assessed with respect to proper visualization of nipple, position of pectoralis major, pectoral–nipple distance (PND), inframammary fold, and adequate coverage of all breast quadrants.
A CC view should ideally demonstrate maximum tissue on both medial and lateral aspects of the breast with the retromammary space and some pectoral muscle (Fig. 1). The following points were analyzed on CC view: (a) nipple should be in profile; (b) nipple should point straight and should not be pointing lateral or medial (Fig. 2); and (c) PND (Fig. 3) must be within 1 cm of the same measurement of the MLO view.

An ideal CC view with retromammary space and pectoralis muscle (

Position of the nipple (A) in profile, (B) pointing medially, and (C) pointing laterally.

Pectoralis–nipple line on (A) CC view and (B) MLO view.
An MLO view should demonstrate axilla, axillary tail, and inframammary fold with all the breast tissue (Fig. 4). On an ideal MLO view (a) breast should be pulled out with nipple in profile; (b) the pectoralis muscle margin should be well visualized; (c) the lower edge of pectoralis muscle should be at the level of pectoralis–nipple line (PNL) or below; and (d) PND must be within 1 cm of the same measurement of the MLO view. When MLO image of both breasts are viewed as mirror images, pectoralis muscle should meet in the midline and form a “V” (Fig. 5).

An ideal MLO view (i) nipple in profile, (ii) pectoralis muscle margin well visualized, (iii) edge of pectoralis muscle below the level of PNL, and (iv) inframammary angle (

Bilateral MLO: pectoralis muscle forming “V,” when viewed as mirror images.
Mammographic views were reviewed side by side: right CC with left CC and right MLO with left MLO, as if they were mirror images of each other. A note was made of the nipple profile and if all the quadrants of the breast were adequately visualized. PND was measured on both the views.
Results
Mammograms were evaluated and note of the mistakes were documented (Table 1). Prescribed guidelines 1 for evaluation of mammograms were followed.
Mistakes in positioning were recognized in 155 of 5382 (2.88%) mammograms. On CC view, nipple was not in profile bilaterally in 23 mammograms and pointing medially or laterally in 80 mammograms (Fig. 2). The unilateral mal-positioning, right or left, was much higher. Abnormal positioning of the nipple was also noted in MLO view (Fig. 6A). Bilaterally, pectoralis was not visualized on MLO view in 14 (Fig. 6B). The edge of the pectoralis muscle was not well defined (straight or convex) in 09 (Fig. 6C) and lower edge of pectoralis was above PNL in 56 mammograms (Fig. 6D). There was inadequate coverage of lower quadrant on MLO view of the right breast in 83, the left breast in 87, and bilaterally in 75 mammograms (Fig. 6E). Mismatch in PND measured on CC view and MLO view was documented in 104 mammograms. Inframammary fold was not visualized in 71 right side, 79 left side, and 32 paired mammograms (Fig. 6F). During the evaluation, in many of the mammograms, more than one pitfall in positioning was noted (Fig. 7).

Mistakes (

Discussion
Breast is a mobile organ variable in size and morphology depending on the body form of the patient. It is relatively fixed in its medial and superior aspect, and relatively mobile in the lateral and inferior aspect. During mammography, the breast has to be pulled away from the chest wall. It has to be moved from the mobile margin to immobile margin for inclusion of maximum tissue. It needs to be adequately compressed and has to be stabilized before imaging.
Breast positioning is the key factor affecting a mammogram.1–5 During mammography, many cases are improperly positioned and inconclusive mammographic results are obtained.6,7 Lesion may be identified only on one mammographic view (Fig. 8). So tailoring of mammography imaging to the specific needs of individual patient is very important. Proper compression helps in spreading of the breast tissue and avoids distortion of the breast parenchyma. It also places pectoralis muscle and nipple at the same level. Compression is also helpful in differentiating between a lesion and superimposed normal structure as it spreads apart overlying islands of dense tissue.

(A) A well-defined lesion seen on CC view. Not well appreciated on an MLO view and (B) a cystic space occupying lesion seen on ultrasound.
Mistakes documented on mammography images.

Sometimes, a spot compression device is used, with or without magnification, to better delineate the area of interest 8 (Fig. 9).
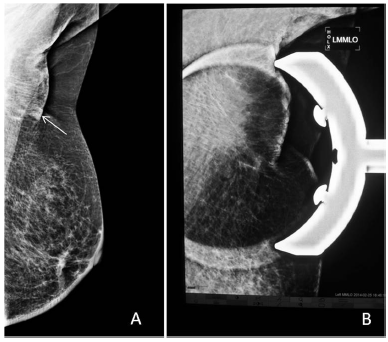
MLO view: (A) a doubtful lesion seen and (B) spot compression with magnification shows normal parenchyma.
During CC view, positioning of patient is done so that the nipple lies approximately in the middle of the detector. The detector has to be adjusted as per the patient habitus. If it is low, the breast would hang down and the nipple will roll inferiorly Also skin folds will be formed. If placed high, considerable postero-inferior portion of the breast would be missed. The patient is made to lean forward toward the machine to bring the breast closer to the detector. This results in forward stretching of the breast and inclusion of the superior posterior breast portion in mammogram. The bottom of the breast has to be supported and pulled up so that the deeper and also the lower most tissues are included on the CC view. Shoulder, of the side that is being imaged, is pushed inferiorly to relax the pectoralis muscle so as to include the breast tissue in the outer quadrant. Visualization of the pectoralis muscle on CC view implies that no tissue along the chest wall has been excluded (Fig. 1).
During the MLO view too, the patient is made to lean toward the equipment for maximum tissue visualization. C-arm of mammography machine is rotated to 45° in order to demonstrate maximum amount of breast tissue and pectoral muscle. Sometimes, angle is individualized as per size of the breast (± 10°). The patient is asked to relax and effort is made to include maximum of the breast tissue including axilla, axillary tail, and inframammary fold. The other non-imaging breast of the patient is gently pressed against the body and kept out of the way.
All these maneuvers during mammography positioning require a dedicated radiographer. We have found that having a female helper assisting in positioning is a big help. We also explained to the patient the imaging procedure to be carried out and about the breast compression. This helps and patients are ready to undergo the discomfort of breast compression and cooperate during the procedure. Careful attention during the imaging can eliminate most mammographic artifacts and increases the performance of mammography. 9 Positioning artifacts are operator dependent and can be improved by training.10–12 Occasionally, if there are multiple shortcomings on the resultant mammogram, we either repeat the mammography or do an ultrasound of the respective breast if needed.
In our study, we found that mal-positioning of nipple was very common. Incorrect nipple positioning can sometimes be due to anatomical or pathological (retraction) reasons and not due to improper positioning. Clinical examination of the patient prior to mammography helps in avoiding fallacies. In obese patients, when compression is inadequate, the nipple tends to roll inferiorly. Also when the patient is not comfortable and moves slightly, the same happens. This can appear as a doubtful mass lesion on the resultant mammogram. A repeat mammography study may sometimes have to be carried out which results into increased radiation exposure to the patient. In addition, an ultrasound may be necessary to rule out the fallacy (Fig. 10). This results into increased workup for both the patient and the radiologist. Also, extra time and money consumed unnecessarily.
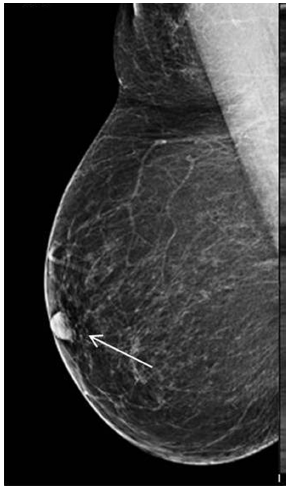
Rolled on nipple appearing as a space occupying lesion on an MLO view of the right breast. Ultrasound breast was normal.
In considerable number of mammograms, we also found that there were fallacies regarding positioning of the pectoralis muscle. Previous studies13–16 have indicated that accepting even borderline positioning that reduces the visualization of pectoralis muscle or the nipple may increase the likelihood of missing an invasive breast cancer and reduce the sensitivity of mammography. An effort should be made to obtain the ideal MLO view as explained above.
To conclude, early detection of breast cancer depends on high quality imaging technique. Positioning is the most important factor affecting the resultant mammographic image. During mammography, many cases are improperly positioned, and as a result, mammographic examination is inconclusive. Improper positioning can also lead to various artifacts and breast pathology can be missed. To avoid all these fallacies, examination has to be tailored as per specific needs of the individual patient. Compromising with even borderline mistakes in positioning increases the likelihood of missing breast cancer and reduces sensitivity of mammography.
Author Contributions
Conceived and designed the experiments: MBP, RT, MN, HK. Analyzed the data: MBP, RT. Wrote the first draft of the manuscript: MBP, RT. Contributed to the writing of the manuscript: MN, HK. Agree with manuscript results and conclusions: MBP, RT, MN, HK. Jointly developed the structure and arguments for the paper: MBP, RT. Made critical revisions and approved final version: MBP, RT, MN, HK. All authors reviewed and approved of the final manuscript.