
Abstract
Objective
The aim of this study is to determine the clinicopathological features of breast cancer in two dedicated cancer treatment centers in north Trinidad. The histological types and stage at presentation were also investigated.
Design and Methods
A retrospective cohort design was used; data were collected from a review of medical records of patients meeting the entry criteria. Clinical and demographic data were extracted.
Results
A total of 640 patients were selected for the study and were available for the analysis. The annual cumulative incidence rate of breast cancer for the calendar years 2010 and 2011 in north Trinidad was 32.4 per 100,000 and 24.6 per 100,000 of the population. The age group between 51–60 years had the highest proportion of cases of breast cancer. There was a significant ethnic disparity in the occurrence of breast cancer, as it was more common in people of African origin than among South East Asians. Surgery and chemotherapy were the major interventions employed.
Conclusion
Breast cancer prevalence continues to be high in Trinidad; we provide evidence of the extent of and the degree of sophistication required to care for patients with breast cancer in a health care system in a small developing country.
Introduction
In the developing world, the epidemiological transition from communicable to noncommunicable diseases (NCDs), such as cardiovascular diseases, diabetes, chronic lung disease, hypertension, and cancer, is now deeply rooted. In response, the United Nations (UN) General Assembly commissioned a special meeting on the prevention and control of NCDs in 2011. Based on the World Health Organization's (WHO) report in 2008, 1 NCDs are the leading causes of death globally, as they are responsible for 36 million deaths (ie, 63% of deaths worldwide). Further, the World Cancer Report of 20082 estimated that there were 12.4 million incidents of cancer in 2008 (6,672,000 cases in men and 5,779,000 in women) and 7.6 million deaths from cancer (4,293,000 in men and 3,300,000 in women), with over half of the incidents occurring in regions with a large proportion of low- and middle-income countries. In women, the most common type of cancer, and the prevalent cause of cancer-related deaths, was breast cancer. In the WHO's comprehensive approach to cancer control, diagnosis and treatment of the advanced stages of the disease are among the several components of care. For this reason, component surveillance should be conducted to identify a need for interventions based on the current and future burden of the disease, and to provide the evidentiary basis to formulate future plans and priorities.
Data collected by the National Cancer Registry (NCR) in Trinidad3,4 revealed that between 1995 and 1999, there were 7,834 new cases of cancer and 4,426 cancer-related deaths. For the period between 2000 and 2002, there were 5,222 new cases of cancer and 3,596 cancer-related deaths. The cancer registry further reported that in comparison to the 1995–1999 data, the 2000–2002 data reflected that the average number of new cases per year increased by 11%, and there was a 35% increase in the average number of cancer-related deaths per year in Trinidad and Tobago. Breast cancer is the second leading cancer overall in Trinidad and Tobago; in the 5-year interval from 1995–1999, there were 1,176 cases of breast cancer, accounting for 15.2% of all cancers recorded. Similarly in the 3-year period from 2000–2002, there were 756 cases of breast cancer. Overall, infiltrating duct carcinoma (n = 557; 47.4%) was the predominant histological type. While these statistics provide some evidence of the increasing burden of breast cancer, there has been incomplete collection of data by the NCR. Specifically, accurate statistics on hospitalized patients are lacking, particularly with respect to clinicopathological correlations and advanced disease statistics, which were identified by the WHO framework as equally important components in developing and implementing cancer control initiatives.
Against this background, the need for countries to develop a coordinated, comprehensive, and integrated approach to cancer control based on all available evidence is imperative. A framework to develop comprehensive cancer control plans, so as to identify their goals and to prioritize their strategies, must be evidence-based and informed by accurate data. 5 Using this conceptual model, we propose to measure the number of breast cancer patients who were admitted to and treated at tertiary health institutions in the northern half of the island.
The aim of this study is to determine the clinicopathological features of breast cancer in two dedicated cancer treatment centers in north Trinidad. The histological types and cancer stage at presentation were also investigated.
Methods
We used a clinical case series design. The starting point for this study was to identify all patients with an established diagnosis of breast cancer treated at major public tertiary institutions that were offering care for patients with breast cancer in northern Trinidad. In Trinidad and Tobago, there is a two-tiered system of health care that consists of a public health care system – which is funded by the state and where all services are free for clients – and a private health care system, which adopts a fee-for-service model. The latter tier is expensive and the client is entirely responsible for all associated costs; hence, this system attracts fewer clients and is logistically difficult to study. Therefore, patients who were selected for this study were confined to public health care facilities. For entry into the study, the following criteria were used: a physician should have diagnosis the patient with breast cancer; there must have been laboratory confirmation; and treatment must have been initiated. In other words, if the patient was currently suspected of having breast cancer, but there was no firm evidence of breast cancer, or if the patient was receiving no treatment for breast cancer, he or she was excluded from the study. Other exclusion criteria included patients who were children (0–12 years), adolescents (13–19 years), pregnant women, and men with breast cancer.
The medical records of all patients diagnosed with breast cancer were reviewed. The first medical records review was performed to identify a physician's diagnosis and to validate laboratory confirmation of breast cancer and current treatment. All patients who satisfied these criteria were selected for the study. Data based on age, date of diagnosis, histological type, stage, and interventions were abstracted from the medical records. Breast cancer staging was based on the TNM system, as defined by the American Joint Committee on Cancer, which takes into account tumor size (T), the extent of regional lymph node (N) involvement, and the presence or absence of metastasis (M) beyond the regional lymph nodes. 6
The Human Development Index (HDI) published by the UN Development Programme (UNDP) is a surrogate marker of development; we used this index to compare cancer incidence in Trinidad with that of other countries. 7 HDI is a summary of human development based on a healthy lifestyle, access to knowledge, and standards of living. The HDI categories can vary from very high (0.793–0.943), to high (0.783–0.698), to medium (0.698–0.522), and to low (0.510–0.286).
Operating rooms (ORs) are among the most expensive surgical resources in hospitals. 8 The average procedure time (including anesthesia and surgery) is defined as the amount of time that includes entry into the operating suite and extends until the time when the patient leaves the OR; this was measured for a unilateral mastectomy procedure. We used this measure to calculate the amount of time consumed in surgical procedures in the management of breast cancer.
All of the data collected for the study were stored, retrieved, and analyzed using SPSS version 16 (IBM, Armonk, NY, USA). We reported the proportions and cumulative incidence rate (CIR), and used a
Results
A total of 640 patients who met the entry criteria were recruited into the study, and while all cases were available for analysis, all of the data from each patient were unavailable. In fact, in only 468 cases was age at diagnosis recorded. The age group ranging from 51–60 years had the highest proportion of breast cancer cases (Table 1). A cut-off point of ≥ 50 years was used to categorize cases into premenopause and postmenopause. There were more women in the postmenopausal age group (n = 291; 62.2%) compared with women in the premenopausal group. However, in the premenopausal group, the rate of the disease increased with age and peaked at 50–61 years, while in the postmenopausal age group, the disease incidence declined with age (Fig. 1). Breast cancer was more common in women of the African Diaspora than women of South East Asian origin, and more common among married women (47%) compared to single women (21.7%). In addition, the incidence of breast cancer was highest among the unemployed. Stage 2A breast cancer was the most common presenting stage (n = 154; 24%), while invasive ductal carcinoma was the most common histological type (n = 429; 67%) (Table 2).
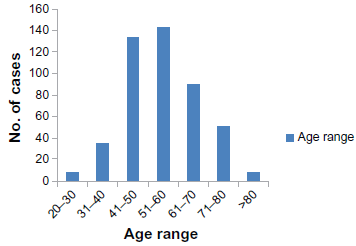
The distribution of breast cancer cases by age at tertiary health care centers in North Trinidad, 2010–2011.
Demographic characteristics of breast cancer treated at tertiary health care facilities in North Trinidad.

Histological types and stages of breast cancer.

A surgical procedure was the most common approach used in the management of breast cancer (n = 459; 71.7%), with 41 (6.4%) patients having surgery as the only intervention (Table 3). All of the other patients who had surgery also had chemotherapy, radiotherapy, and hormone therapy in various combinations; the combination of surgery and chemotherapy was the most common (n = 151; 23.6%). The most frequent surgical procedure was unilateral mastectomy (n = 321) which, in some cases, was combined with axillary node clearance (ANC), wide local excision, or both. The average time utilized in performing a unilateral mastectomy was 2 hours and 21 minutes, which is approximately half the time of a 4-hour (8:00 am–12:00 pm) elective surgical session.
Various approaches to treating breast cancer.

The proportion of women who had a diagnostic mammography was 6.8%; no patient in the study had a cancer detected bt mamography. Several other methods were employed when confirming the diagnosis, including needle core biopsy, computed tomography and trucut biopsy, ultrasound-guided trucut biopsy, and fine-needle aspiration biopsy. It should be noted that there are only four licensed oncologists with the local registration body to serve a population of approximately 1.3 million (ie, one oncologist per 325,000 individuals).
Discussion
The annual CIR of breast cancer, as determined by this study for the calendar years 2010 and 2011, in north Trinidad was 32.4 per 100,000 and 24.6 per 100,000, respectively. These findings are consistent with rates reported by the NCR, indicating that Trinidad continues to sustain a high incidence of breast cancer. This falls against a background where global breast cancer incidence rates have increased by about 0.5% annually since 1990. 9 Cancer registries in China are recording annual increases in breast cancer incidence of 3%–4%, with urban registries documenting 20%–30% increases in the past decade alone; 10 this is accompanied by an absence of a population-based breast cancer screening strategy. In addition, in Asian countries that have the most developed data registries (such as in Japan, Singapore, and Korea), breast cancer rates have doubled or tripled in the past 40 years. 10 In the urban areas of India, cervical cancer had the highest incidence rates among cancers in women 15 years ago, but it has now been overtaken by breast cancer as the most commonly diagnosed cancer among women. 11 Therefore, in the developing world, breast remains a critical public health challenge.
The HDI, published by the UNDP, is a summary of human development based on a healthy lifestyle, one's access to knowledge, and one's standard of living. The HDI is categorized by scores that can vary from very high (0.793–0.943), high (0.783–0.698), medium (0.698–0.522), and low (0.510–0.286). Trinidad and Tobago is ranked 62nd in the world in terms of HDI score (HDI = 0.76; high), and tenth in the regions of Latin America and the Caribbean. Countries with a similar HDI to Trinidad and Tobago reported CIR for breast cancer of 38 per 100,000 population. Bray et al 12 reported in 2012 that countries with a high HDI was associated with high incidence rates of female breast cancer, as well as prostate, and colorectal cancers; our findings are consistent with theirs.
We used occupation as a surrogate marker for socioeconomic status (SEC). Among the women with breast cancer, 60% were unemployed compared to women who were employed (36%), and hence, breast cancer was more common in lower socioeconomic groups. This is in contrast to the developed world where breast cancer is more common in higher socioeconomic groups. 13 Socioeconomic variations in breast cancer incidence have been attributed to the environment, 14 lifestyle,15,16 biological effects, 17 access to health care,18–24 and health-seeking behavior,25–28 all of which are applicable in our setting. Therefore, we provide evidence that in a developing country such as Trinidad, which enjoys a high standard of living based on the HDI, it still remains that the lower SEC groups carry the burden of disease in contrast to those in the developed world.
There were no cases of breast cancer among those younger than 15 years of age, while the occurrence was very low among women at the two extremes of life (20–30 years and 71–80 years; Figure 1). The Centers for Disease Control and Prevention in 2010 confirmed that the risk of breast cancer increases with age. 29 In the United States, during 2006–2010, the incidence of breast cancer was 9.6% among those between 35 and 44 years of age; 22.2% among those who were between 45 and 54 years of age; 25.2% among those who were between 55 and 64 years of age; 20.7% among those who were between 65 and 74 years of age; 14.8% among those who were between 75 and 84 years of age; and 5.7% among women 85+ years of age. 29 Our findings indicated that breast cancer increased 17-fold between those who were 20–30 years and those who were 41–50 years, with 5.5% of the cancers occurring in women under the age of 40 years. In contrast, in the postmenopausal period, breast cancer occurrence declined sharply with increasing age (Fig. 1). This is occurring during a period that is characterized by a lack of influence of estrogens and progesterone from the ovaries. This finding, therefore, supports the role of endogenous hormones in the etiology or development of breast cancer. However, this role has yet to be clearly defined. On the one hand, there is evidence that strengthens the association between endogenous sex steroids and breast cancer: early age of menarche, late age of menopause, and the use of hormone replacement therapy in postmenopausal women have all been repeatedly associated with an increase in breast cancer risk. 30 Similarly, at an early age at first pregnancy, high parity and prolonged breastfeeding have been associated with decreased risk of breast cancer, 30 which is mainly explained by the differentiation of mammary tissue induced by pregnancy-related hormones. Yet, we found that the number of cases of breast cancer was higher in married women who are more likely to become pregnant. In fact, there were twice as many married women with breast cancer than any other group. Several studies have shown that married women have a higher incidence of breast cancer than single women. 31 In addition, large-scale prospective epidemiological studies have confirmed the role of endogenous sex steroids in the onset of breast cancer in postmenopausal women. 32 Results from these studies showed that women with elevated serum estrogen (estradiol, estrone, and free estradiol) and androgen (testosterone, free testosterone, androstenedione, and dehydrepiandrosterone) concentrations in the upper quintile of the hormones examined were at about a twofold increase for breast cancer risk compared to women in the lowest quintile. A number of case control studies nested within large cohorts have suggested a positive association between breast cancer incidence and prolactin levels, although results have been more consistent in postmenopausal women than in premenopausal women. 33 Several epidemiological studies have been published on the relationship between circulating insulin-like growth factor-I (IGF-I) to breast cancer risk, with different results: preliminary studies reported an overall twofold increase in risk with increasing circulating IGF-I levels, but only in women who had a diagnosis of breast cancer at a relatively young age (before 50 years of age), 34 while more recent studies reported a moderate increase in risk of about 30% in women who had a diagnosis of breast cancer when older than 50 years.35,36
Methods of diagnosis for breast cancer.

In Trinidad, there are two major diasporas: people of African origin and people of South East Asian origin, both representing approximately 44% of the population. We found a significant ethnic disparity in the occurrence of breast cancer in these two ethnic groups. Breast cancer was significantly (
The majority of women in the study (72%) had received a surgical intervention. We provide additional evidence that in developing countries, surgical services (though grossly inadequate) remain the most widely used treatment for solid tumors, as suggested by Ozgediz and Riviello. 46 Chemotherapy was also commonly used (69.5%). In fact, surgery with chemotherapy was the most common combination used out of an array of combinations with radiotherapy and hormone therapy. Unilateral mastectomy and ANC was the procedure used for 34.5% of the patients. The majority of women receiving chemotherapy and surgery had stage 2A breast cancer (23.1%). This group of women had the most unilateral mastectomies, as well as the most unilateral mastectomy and axillary clearance combined. As far back as 1988, Daisley et al 47 showed that 48% of patients with breast cancer in Trinidad and Tobago were diagnosed with stage 2A breast cancer, and that mastectomy with axillary clearance was the preferred surgical procedure. 47 In 2012, nearly 25 years later, the pattern of disease or surgical intervention has not changed. Furthermore, the predominant histological type (invasive ductal carcinoma) remains the most common histologically type reported (n = 429; 67.0%).
Only 36.2% of patients received radiotherapy as part of their treatment. Radiotherapy is now a clinically essential part of the armamentarium against cancer. In fact, about 70%–83% of breast cancer patients would be expected to undergo radiotherapy. 48 The WHO, in its world cancer report, has also clearly articulated the role for radiotherapy as part of the multimodality and multidisciplinary management of patients with cancer. The report states, “… it is essential for good cancer care: chemotherapy and surgery cannot effectively replace it. Where it is not available 50% of cancer patients are being denied appropriate care.” 2
The mammogram as a diagnostic tool was used in less than 7% of patients and none of the women had prior screening. Mammography is still the most effective and widely used imaging modality for breast cancer screening. Several large randomized clinical trials have shown that mammography reduces mortality from breast cancer.49–52 We join with others in advocating the use of mammography to promote earlier diagnosis, together with effective treatments, to reduce the mortality rates associated with breast cancer in Trinidad and, by extension, the wider developing world. 53 This position is, however, tempered by the prevailing discordance – especially in the Unites States – among the recommendations for screening mammography by various guidelines.
The major limitation in the present study was lack of information on some of the variables examined. Medical records are handwritten and often incomprehensible, poorly stored in bulky folders, making retrieval difficult and capture of all the data challenging. Only patients who attended public health facilities were entered into the study. Patients seen and treated using private health care facilities would have been logistically difficult to access. These factors notwithstanding, this sector is considerably smaller due to the high cost of private health care services.
In conclusion, breast cancer prevalence continues to be high in Trinidad. We provide evidence of the extent of, and levels of care currently administered to, patients with breast cancer by a public health care system in a small developing country. Several challenges emerged; for example, suboptimum delivery of health care can contribute to late diagnosis and poor survival. Essential screening programs are absent. The key challenges, however, revolve around human capacity and training, subspecialization of services, and the need for earlier diagnosis and awareness in the population. These needs have to be tempered against competing interests for small budgetary allocations to health care. Nevertheless, depending on the resources available and any competing health priorities, all steps must be taken to prevent those cancers that are preventable, to treat those cancers that are treatable, to cure those cancers that are curable, and to provide palliation and supportive care to patients throughout their cancer trajectory. This has important implications for public health as well as other elements of health services in the developing world. There will be a need for more medical, nursing, and related staff to treat these patients, as well as a need for more hospitals. The implications for planning are that cancer control programs will need to be formulated and implemented to help reduce the mortality burden. Low-resource countries face numerous challenges in designing and implementing programs to improve cancer care, such as a lack of scientific and epidemiological information to guide resource planning, a shortage of trained professionals to provide necessary clinical care, competing health care crises, political insecurity or wars, or combinations thereof that divert attention from long-term health care issues, as well as social and cultural factors that obstruct the timely and effective delivery of care.
Author Contributions
Conceived and designed the experiments: KM. Analyzed the data: KM, WAC, MG, ND, LM, JR, MS. Wrote the first draft of the manuscript: KM, JR, SA, ND, MG. Agree with manuscript results and conclusions: KM, JR, WAC, SA, ND, MG, LM, VM, JR, MS. Jointly developed the structure and arguments for the paper: KM, JR, WAC, SA, ND, MG, LM, VM, JR, MS. Made critical revisions and approved final version: KM, JR, WAC, SA, ND, MG, LM, VM, JR, MS. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.