
Abstract
Background:
Atrial fibrillation (AF) is the most common sustained supraventricular arrhythmia encountered in clinical practice. Due to the higher prevalence of rheumatic fever in several regions of India, rheumatic heart disease (RHD) is the most common etiological factor of AF.
Aims and Objectives:
The objective of the study was to study clinical features, electrocardiographic (ECG) and echocardiographic (ECHO) findings, complications, and incidence of AF in rheumatic mitral valve disease (R-MVD).
Methods:
It is an observational cross-sectional study of 40 indoor patients in a Tertiary Care Hospital in Vadodara, Gujarat, carried over a period of a year. Clinical data including symptoms, signs, systemic examination, and relevant investigations were studied.
Results:
67.5% (n = 27) of patients having AF were below the age of 50 years with higher incidence among females (72.50%) as compared to males (27.5%). Fifteen (37.5%) had mitral stenosis (MS) and 13 (32.5%) had MS with regurgitation. Most of the patients 35 (87.5%) presented with breathlessness, followed by palpitation 28 (70%). The most commonly heard murmur was mid-diastolic (65%, n = 26), followed by pansystolic murmur (40%, n = 16) at the apex. Out of 40 patients, 15 (37.5%) had evidence of left ventricular hypertrophy on ECG, whereas only 5 (12.5%) had right ventricular hypertrophy. Four out of five patients with the evidence of cardioembolic stroke had left atrium (LA) size >45 mm which suggests an increased risk of embolic stroke with increased LA size. Only 3 (7.5%) patients had a visible LA clot in LA on two-dimensional ECHO, whereas only one patient had vegetation on valves. Twenty-seven out of 30 patients treated with diltiazem show good response. Heart failure was the most common complication affecting 85% (n = 34) of the patients with AF with R-MVD. Four (10%) patients out of 40 expired including 1 (25%) of the four pregnant patients, suggesting higher mortality among pregnant females due to superimposed physiological changes occurring during pregnancy.
Conclusion:
In developing countries like India, RHD is a major cause of AF affecting the younger population and more commonly females. Most of the patients in our study presented with breathlessness and palpitation. LA size was directly proportional to the risk of cardioembolic stroke and most of the patients developed heart failure as a complication.
Keywords
INTRODUCTION
Atrial fibrillation (AF) is the most common sustained supraventricular arrhythmia in clinical practice, where there is no definite coordinated universal atrial contraction or relaxation. Instead, there are irregular dissociated large contractions at about 350–600/min which produces worm-like (fibrillary) quivering of atria without an effective atrial contraction.[1] Community prevalence of AF is 0.5%–5.5% worldwide and 0.1%–1.6% in India in 2022.[2]
AF is caused by cardiovascular as well as noncardiovascular disease. Cardiovascular causes include rheumatic heart disease (RHD), hypertension, coronary artery disease, cardiomyopathy, valvular heart disease (nonrheumatic), and ischemic heart disease (IHD), whereas noncardiovascular causes include chronic obstructive lung disease, pneumonia, pulmonary embolism, hyperthyroidism, hypokalemia, excessive alcohol consumption, and the like.[3-6]
In India, rheumatic fever is still a major menace in certain regions and therefore RHD is the most common etiological factor of AF. Mitral valvular lesions cripple a substantial portion of youth, and superimposed AF leads to serious complications and mortality.[7,8] The risk of heart failure in these patients is 3.4 times higher than in the normal population.[9]
Here, we aim to study demographics, clinical features, electrocardiographic (ECG) findings, radiological features, as well as echocardiographic (ECHO) features and their correlation with complications, correlation of left atria (LA) size with the incidence of AF, the incidence of systemic embolization and other complications, and response to therapeutic measures employed in AF with rheumatic mitral valve disease (R-MVD).
METHODS
An observational cross-sectional study of 40 indoor patients was carried out after getting permission from the Institutional Ethics Committee for Human Research-PG Research (IECHR-PG), a Tertiary Care Hospital in Vadodara, Gujarat, over a period of a year from January 2019 to January 2020. Patients over 18 years of age with two-dimensional ECHO (2D-ECHO) suggestive of R-MVD and presented with AF confirmed by ECG were enrolled. Those who had AF due to causes other than R-MVD and R-MVD not having AF were excluded from the study.
Data were collected in the form of history taking such as demographic data, chief complaints (such as breathlessness, palpitation, chest pain, cough, hemoptysis, and pedal edema), history of rheumatic fever, RHD, hypertension, diabetes, IHD, and cardiovascular complication during pregnancy; family history; and personal history. A thorough general examination comprising pulse, blood pressure, pedal edema, and apex pulse deficit was noted. Cardiovascular system examination including position and nature of apex beat, presence of any thrills and murmurs, and their characteristics such as the site, radiation, and the intensity of heart sound were noted. Respiratory system, per abdomen, and central nervous system examinations were done with special emphasis on the presence of cardiac failure and cerebrovascular complications. Investigations including routine hemogram, renal and liver function tests, and standard 12-lead ECG were taken for each patient. 2D-ECHO was also noted in detail with special emphasis on LA size and mitral valvular involvement. AF was treated with various drugs such as diltiazem, metoprolol, amiodarone, and digoxin as well as direct current (DC) cardioversion. The effectiveness of treatment was noted based on the control of ventricular rate. All the complications of AF in R-MVD were noted in detail.
Statistical analysis
All the data were entered into Microsoft Excel Spreadsheet. Continuous variables were expressed as mean and standard deviation (SD), and categorical variables were expressed as frequency and percentages. Data were analyzed using Epi Info software (version 7.2.5.0, Center for Disease Control and Prevention, U.S. Department of Health and Human services, united states).
RESULTS
A large number of patients (67.5% n = 27) having AF were below the age of 50 years, whereas only three patients were older than 70 years [Table 1]. This finding was suggestive of a higher incidence of AF in R-MVD in the young-to-middle age population.
Age distribution in atrial fibrillation with rheumatic mitral valve disease

Graph 1 shows that the incidence of AF in R-MVD was much higher in females (n = 29) as compared to males (n = 11). Male: female ratio was 0.37:1. There were four pregnant females in the study.
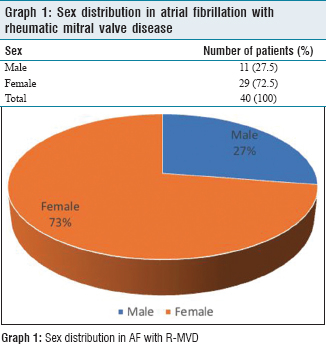
Sex distribution in atrial fibrillation with rheumatic mitral valve disease
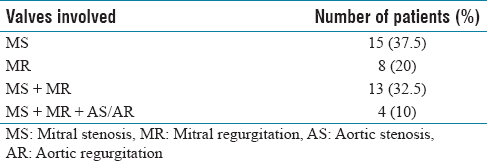
Table 2 shows that mitral stenosis (MS) was the most common valvular affection presenting with AF followed by MS + mitral regurgitation (MR) and MR.
Valvular involvement in atrial fibrillation with rheumatic mitral valve disease
As shown in Graph 2, breathlessness (87.5%) was the most common presenting complaint in our study, followed by palpitation (70%) and cough (50%). None of the patients in the present study were asymptomatic.

Symptoms of atrial fibrillation in rheumatic mitral valve disease
On general examination, pedal edema (50%, n = 20), pallor (50%, n = 20), and raised jugular venous pressure (JVP) (47.5%, n = 19) were the most commonly found signs, whereas icterus and ascites were seen in 15% (n = 6) and 7.5% (n = 3) of patients, respectively. Study participants’ overall mean pulse is 125/min (SD = 21.07), mean pulse in males is 122/min (SD = 21.61), and mean pulse in females is 127/min (SD = 21.11). Apex pulse deficit was present in all the patients (100%, n = 40) presented with AF. All the patients (n = 40) had the variable intensity of first heart sound (S1), out of which only 16 (40%) had loud S1. Only 27.5% (n = 11) of patients had a loud pulmonary component of the 2nd heart sound (P2).
The most commonly heard murmur was mid-diastolic (65%, n = 26) at the apex, followed by pansystolic murmur (40%, n = 16) at the apex. Systolic murmur at the pulmonary area and pansystolic murmur at the tricuspid area are heard in 35% (n = 14) and 20% (n = 8) of patients, respectively. Twenty-four patients (60%) had crepitations over the base of both lungs while only six patients (15%) had rhonchi.
Maximum patients (25%, n = 10) had a ventricular rate between 181 and 200/min, whereas only three patients (7.5%) had a controlled ventricular rate of 100/min [Graph 3].

Heart rate (ventricular rate) of patients presenting with atrial fibrillation in rheumatic mitral valve disease from electrocardiographic
Out of 40 patients, 15 (37.5%) had evidence of left ventricular hypertrophy on ECG, whereas only 5 (12.5%) had right ventricular hypertrophy. The left bundle branch block and the right bundle branch block were present in 12.5% (n = 5) and 5% (n = 2) of patients, respectively. Study participants’ overall mean AF rate is 168/min (SD = 38.56), mean AF rate in males is 162/min (SD = 33.19), and mean AF rate in females is 170/min (SD = 40.75). Ninety per cent (n = 36) of the patients had coarse “f” waves in ECG, which depends on the etiology of AF (rheumatic valve disease) and size of LA (more the size, the “f” waves are coarse), whereas only 10% had fine “f” waves in ECG.
Graph 4 shows that, on 2D-ECHO, LA (90%) was the most common chamber to be enlarged, followed by the right ventricle (RV) (50%).

Chamber enlargement on echocardiography in atrial fibrillation with rheumatic mitral valve disease
Table 3 indicates that an increase in the size of LA was associated with an increased risk of cardioembolic stroke. Study participants’ overall mean LA size is 4.43 cm (SD = 0.56), mean LA size in males is 4.58 cm (SD = 0.52), and mean LA size in females is 4.37 cm (SD = 0.57).
Association between the size of the left atrium on echocardiography and incidence of cardioembolic stroke

The majority of patients (70%, n = 28) had pulmonary artery pressure (PAP) of more than 50 mmHg, out of which 7 (17.5%) had PAP of more than 70 mmHg. Only 3 (7.5%) patients had a clot in LA visible on 2D-ECHO, whereas only one patient had vegetation on valves. Study participants’ overall mean PAP is 57.22 mmHg (SD = 13.63), mean PAP in males is 57.91 mmHg (SD = 11.12), and mean PAP in females is 56.97 mmHg (SD = 14.63).
Diltiazem was the most commonly used drug to control the ventricular rate in our study, used in 30 (75%) patients, out of which 27 showed a good response (90%), whereas 13 (32.5%) patients were given metoprolol, out of which 11 showed a good response (85%). Five patients (12.5%) were given DC shock. Digoxin and amiodarone were used in 15% (n = 6) and 7.5% (n = 3) of patients, respectively. Response to therapy was assessed in the form of control in ventricular rate.
All the patients of AF in R-MVD were initially given low-molecular-weight heparin (LMWH), followed by warfarin in 82.5% of patients as it is contraindicated in pregnancy and conditions with bleeding tendencies.
As shown in Table 4, heart failure was the most common complication affecting 85% of the patients with AF with R-MVD.
Complications of atrial fibrillation in rheumatic mitral valve disease

Of 40 patients with AF with R-MVD, 4 (10%) expired. Out of four pregnant patients who presented with AF with R-MVD, 1 (25%) expired, suggesting higher mortality among pregnant females due to superimposed physiological changes occurring during pregnancy.
DISCUSSION
In developed countries, coronary artery disease is the most common cause of AF, where AF is more common in men than women. However, in developing countries, RHD, specifically MS is the most common cause of AF, where AF is more common in women than men. Overcrowding, poor hygienic conditions, low socioeconomic status, and malnutrition play a major role in acute rheumatic fever and RHD in developing countries.[10] In the Framingham heart study and Cardiovascular Health study, the incidence rates of AF were higher in men than women as well as in the elderly compared to the young.[11-13] However, in our study, the incidence rates of AF were higher in women (72.5%) as compared to men (27.5%) and below the age of 50 years (67.5%) compared to the aged population. These findings are similar to the results of Jyotirmayi Boddu and Srinivas Reddy (68% of patients belonged between 21 and 40 years of age), Sharma and Verma (55% of patients were between 21 and 30 years of age, 56% of women), and Vora et al. (51% were female).[14-16]
From Table 5, it can be seen that breathlessness and palpitation are the most commonly found symptoms in most studies. Chest pain as a symptom of AF was more commonly seen in patients of AF in the Western countries, accounting for additional relative coronary insufficiency.[17-19] Hemiplegia (paralysis) is a manifestation of the most dangerous complication of AF, cardioembolic stroke. The brain is the most common site of systemic embolism in patients with AF. In Morris and Hurst (1980), Anguita et al. (2018), and Prakash and Chugh studies, 8%, 10%, and 6% of patients had paralysis, respectively. In our study, 12.5% of patients developed cardioembolic stroke with subsequent hemiplegia.[17-19]
Comparisons of clinical findings in patients of atrial fibrillation with rheumatic mitral valve disease in the present study with other similar studies

In a study by Radha Krishnan and Srinivas,[20] out of 100 patients with acquired valvular heart disease, the most affected heart valve was the mitral valve (56%), of which 27% had isolated MS, 14% had isolated MR, 17% had MS + MR, and 26% had multivalvular involvement. While in our study, isolated MS is seen in 37.5% of patients, followed by MS + MR (32.5%), isolated MR (20%), and only 10% had multivalvular involvement.
In our study on echocardiography, LA was found to be enlarged in the majority of 90% of patients, whereas 50% had enlarged RV. LA enlargement is attributed to a change in the LA pressure consequent to valvular obstruction in chronic RHD. According to Mrozowska et al.,[21] AF is uncommon when the LA size is <40 mm. 67.5% of patients in our study and 62.7% of patients in the Jyotirmayi Boddu and Srinivas Reddy study had LA sizes >40 mm on 2D-ECHO, respectively.[14] LA enlargement in AF is associated with worsening of functional status, development of pulmonary artery hypertension (PAH), and congestive cardiac failure (CCF). In our study, 7.5% of patients had LA clots visible on 2D-ECHO, whereas in the study by Jyotirmayi Boddu and Srinivas Reddy, 45.3% of total patients had a clot in LA.[14] LA thrombus was also observed in 54% and 56% of patients in the studies related to MS and AF by Karatasakis et al.[22] and Hwang et al.,[23] respectively. Embolic complications such as stroke are more in patients with AF with LA dilatation. In our study, five patients (12.5%) developed cardioembolic stroke, almost all having a LA size of more than 45 mm. This indicates that an increase in the size of LA is associated with an increased risk of cardioembolic stroke. Whereas in the study done by Wolf et al., the incidence of stroke was 31%.[11]
As per our study, 85% of patients of AF with R-MVD had heart failure as a complication, which is similar to the results of the studies by Stewart et al. and Miyasaka et al.[9,24] Mortality was 10% in our study as also observed by Vidaillet et al.[25]
Limitations
It is a single-center descriptive study with limited subjects; hence, in-depth statistical analysis was not possible. A large multicenter study with a more number of subjects may help to understand and analyze various factors of R-MVD contributing to the development of AF and its complication in more detail, a condition which is still causing substantial morbidity and mortality in the young and reproductive age group of India.
Follow-up of the patients with details about the frequency of hospitalization with worsening/aggravating factors would guide us to understand the disease course.
Echocardiography with detailed information on the mitral valve leaflets such as leaflet mobility, valvular thickening, subvalvular thickening, and valvular calcification with the calculation of Wilkins score would be a better marker of prognosis and guide for further treatment. Transesophageal echocardiography was not done in our study.
Newer Direct oral anticoagulants (dabigatran; apixaban, edoxaban, rivaroxaban) and direct factor Xa inhibitors (apixaban, edoxaban, and rivaroxaban) were not given to our patients.
CONCLUSION
In our study, AF was common in those <50 years of age, suggesting early rheumatic affection of the mitral valve in developing countries like India. Females were more affected than males. MS is the most common valvular lesion, followed by combined MS and MR. Breathlessness was the most common presenting symptom, followed by palpitation and cough. Apex pulse deficit was present in all patients with other common signs such as pedal edema, pallor, and raised JVP. Mid-diastolic murmur at the apex was the most commonly heard murmur in our study. The majority of patients had coarse “f” fibrillatory waves in ECG, depending on the etiology of AF and LA size. On 2D-ECHO, the most commonly enlarged chamber was LA followed by RV. More than two-thirds of patients had LA size >40 mm and the majority of patients had severe PAH on 2D-ECHO. The majority of patients were treated with diltiazem or metoprolol for rate control, of which most showed good responses. LMWH was given for anticoagulation to all the patients, whereas 82.5% of patients were given warfarin as it is contraindicated in pregnancy. CCF was the most common complication followed by cardioembolic stroke. An increase in the size of LA is associated with an increased risk of cardioembolic stroke. There is a significant increase in the morbidity and mortality of pregnant patients, thereby reducing their life expectancy. The analysis of the present study gives us insight into the various aspects of valvular involvement in patients with AF with R-MVD. The study emphasizes the need for early detection and early treatment of rheumatic fever and RHD to prevent the progression and development of complications.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
The Institutional Ethics Committee for Human Research-PG Research (IECHR-PG, ECR/85/Inst/GJ/2013/RR-16), a Tertiary Care Hospital in Vadodara, Gujarat, over a period of a year from January 2019 to January 2020.
Funding
Nil.
Author’s contribution
Minal Shastri: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content and final approval of the version to be published, Heti Mistry: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content and final approval of the version to be published, Vishakha Vinod: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content, Vaishnavi Rathod: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content, Abulkalam Sirajwala: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content. Nilay Patel: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content. Riya Dobariya: Concept and design of study or acquisition of data or analysis and interpretation of data, Drafting the article or revising it critically for important intellectual content. The prominent roles of each also included the following Concept and design of study, literature review, drafting and editing the manuscript, clinical analysis and interpretation.