
Abstract
Background:
Laparoscopic cholecystectomy pain is a sensory and emotional experience connected with actual or potential tissue damage. Effective pain control is quite important, with around 70% of patients still complaining of moderate-to-severe pain postoperatively. Uncontrolled perioperative pain may raise patient morbidity and mortality rates. Both gabapentin and clonidine as premeditated can be easily administered have minimal side effects, are easily available at a low price, both them have a sedative effect that can decrease anxiety and they can blunt the stress response. Moreover, both drugs have anti-nociceptive effects that may be beneficial for controlling postoperating pain which is the basis of our current study.
Aims:
This study aims to compare the efficacy of oral clonidine with gabapentin before induction of anesthesia in attenuating hemodynamic stress response to laryngoscopy, intubation, and carbon dioxide pneumoperitoneum in laparoscopic cholecystectomy and to compare the efficacy of oral clonidine with oral gabapentin for postoperative pain control.
Materials and Methods:
Hundred patients undergoing laparoscopic surgery and qualifying inclusion criteria were randomly allocated into two groups each containing 50 patients. Group I patients were given Tab. Clonidine (300 μg) and Group II patients were given tablet Gabapentin (600 mg) orally 60 min before induction of general anesthesia. Hemodynamic changes and the incidence of postoperative pain in both groups were measured and compared.
Results:
Hemodynamic blunting to pressor stress of laryngoscopy and intubation was seen in both groups with better results obtained in the group receiving clonidine in the form of lesser variations in heart rate, systolic blood pressure, and diastolic blood pressure. Postoperative analgesia was achieved in both groups but gabapentin showed a better analgesic profile in the form of lesser Visual Analog Scale scoring and decreased utilization of rescue analgesia.
Conclusion:
Clonidine (300 μg) cause a greater attenuation of intraoperative hemodynamic stress responses, whereas gabapentin (600 mg) provides superior postoperative analgesia.
INTRODUCTION
According to the International Association for the Study of Pain,[1] laparoscopic cholecystectomy pain is an emotional and sensory experience connected with potential tissue damage. Therefore, it is quite important to devise an effective pain control, with around 70% of patients still complaining of moderate-to-severe pain postoperatively.[2] Uncontrolled perioperative pain may raise patient morbidity and mortality rates.
The uncomfortable abdominal surgical incisions cause a reflex increase in abdominal muscle tone during expiration and a loss in diaphragmatic function. As a result, pulmonary compliance decreases and causes muscles spasm, and it becomes difficult to breathe deeply or cough vigorously. Analgesic therapy may have both immediate (such as a reduction in postoperative pain and quicker recovery) and long-term (like a reduction in chronic pain and an improvement in health-related quality of life) advantages for the patient while they are recovering.[2]
Hemodynamic stress reactions, such as tachycardia and hypertension, are brought on by direct laryngoscopy and laparoscopic cholecystectomy. Catecholamine levels in the blood rise[3] and myocardial ischemia and cerebral hemorrhage may also occur.[4] In the past, premedication using calcium channel blockers, adrenergic receptor antagonists,[5] opioids and drugs causing vasodilatation[6] were utilized with varying degrees of success to attenuate these effects.[7,8] Although the latest perioperative ischemic evaluation 2 (POISE 2) study’s findings indicated no decrease in cardiac events or mortality and an increase in clinically significant hypotension and nonfatal cardiac arrest, clonidine has also initially demonstrated promise.[9] Therefore, a clinically significant concern for high-risk surgical patients is the quest for substitute drugs that do not cause such adverse effects.
The effectiveness of gabapentin and clonidine has been demonstrated in lowering surgical pain, reducing opioid consumption, and lowering postoperative nausea and vomiting.[10] Both gabapentin and clonidine, as premeditates, can be easily administered, have minimal side effects, are easily available at a low price and have a sedative effect that can decrease anxiety and stress response. Moreover, both medications contain anti-nociceptive properties that could be useful for reducing pain after surgery. In addition, a recent meta-analysis found that gabapentin reduces preoperative anxiety and persistent pain at the cost of more sedation.[11] Two randomized-controlled trials that were published in the past 10 years suggest that gabapentin may also help reduce the hemodynamic reaction to intubation.[12]
Despite a large number of studies, there is still no consensus on whether gabapentin or clonidine, of the two, is the better drug for postoperative analgesia. Therefore, the present study was conducted to examine the effects of gabapentin and clonidine as premedication on postoperative analgesic needs and intraoperative hemodynamic responses during laparoscopic cholecystectomy, at a tertiary care center.
Gabapentin
In 1993, 1-(aminomethyl) cyclohexane acetic acid, commonly known as gabapentin which is an analog of gamma amino butyric acid was first introduced for partial seizures treatment which was refractory in nature.[13] An anticonvulsant drug called gabapentin was first identified in the 1970s.[1] Originally used to relax muscles and treat spasms, it has now been discovered that it also has the potential to act as an anticonvulsant and a supplement to more effective anticonvulsants.
Other neuropathic pain, postpoliomyelitis neuropathy, reflex sympathetic dystrophy, and diabetic neuropathy can also be effectively treated with it. Along with these other qualities, it possesses properties which allow it to inhibit pain perception, hypersensitivity to pain and allodynia.[14] It has more recently been utilized to lessen the stress reaction to laryngoscopy and intubation.[15]
Clonidine
A selective partial α2-adrenergic receptor agonist was introduced in 1966. Due to its sympatholytic, hypnotic, sedative, anxiolytic, analgesic, and anesthetic-sparing actions without respiratory depression.[16] By lowering the heart rate (HR) and blood vessel dilatation, clonidine significantly reduces blood pressure and improves blood flow throughout the body. The cerebral area that regulates attention and impulsivity may be affected by clonidine extended-release pills, which are used to treat attention deficit hyperactivity disorder (ADHD). Other conditions that can be treated with clonidine include hypertensive crisis, painful menstruation (dysmenorrhea), compulsive repetitive movements (Tourette’s syndrome), withdrawal from narcotics and alcohol, and hot flashes of menopause.
Aim and objectives
To compare the efficacy of oral clonidine with oral gabapentin before induction of anesthesia in attenuating hemodynamic stress response to laryngoscopy, intubation, and carbon dioxide pneumoperitoneum in laparoscopic cholecystectomy
To compare the efficacy of oral clonidine with oral gabapentin for postoperative pain control.
MATERIALS AND METHODS
After permission from the institutional ethics committee, the present randomized study was carried out in the Department of Anaesthesiology, at Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, for 2 years in 100 patients.
Sample size calculation
Analysis was conducted using the power package, G power version 3.1.9.2 (Granz Faul, University Kiel, Germany). Our sample size came out to be 50 subjects per group at a power of 0.99 and with an effect size of 2.78 with a 10% chance of error with alpha = 0.05, beta = 0.20, and a confidence interval of 95%.
Inclusion criteria
American society of anaesthesiologists (ASA) Grade I and II patients undergoing laparoscopic surgery.
Exclusion criteria
Patients with hypertension, ischemic heart disease, rhythm other than sinus, any degree of heart block, diabetes mellitus, chronic obstructive pulmonary disease, bronchial asthma, and peripheral vascular disease
More than 1 attempt for intubation
Patients that had a conversion to open surgery after laparoscopic visualization.
Study procedure
Methods
The study was a prospective, randomized placebo control study. Computer-based randomization was done.
Materials
The patients satisfying the inclusion criteria were randomly allocated into two groups each containing 50 patients.
Pre-anesthetic evaluation was done in the following order:
History Clinical examination Relevant investigations Informed consent from patients Fasting for 8 h.
Pre-anesthetic medication was given with a tablet Pan top 40 mg and tablet clonazepam 0.25 mg the night before surgery and the coming morning. Patients were randomly divided into two groups as follows:
Group I – Was given Tablet Clonidine (300 μg) Group II – Was given Tablet Gabapentin (600 mg).
The tablets were given orally with sips of water 60 min before the induction of general anesthesia. Before administration of oral premedication, each patient’s baseline HR, systemic blood pressure, diastolic blood pressure (DBP), and mean arterial pressure and SpO2 were recorded and IV access was established.
After shifting the patient to the operation table monitors for vitals were attached. The baseline values were recorded. Injection midazolam 0.03 mg/kg and injection glycopyrrolate 0.2 mg i.v., were given and patients were preoxygenated for 3 min. Anesthesia was induced with injection of propofol 2 mg/kg, injection fentanyl 2 microgram/kg and injection vecuronium 0.1 mg/kg. A proper size cuffed poly vinyl chloride (PVC) endotracheal tube was inserted orotracheally. Anesthesia was maintained with nitrous oxide 67%, oxygen 33%, isoflurane 1%, and intermittent doses of injection vecuronium and injection fentanyl. Ventilation was controlled mechanically and was adjusted to keep ETCO2 between 30 and 35 mm of Hg. The intra-abdominal CO2 pressure was kept between 12 and 14 mm of Hg. A ryles tube was inserted and suction was applied to empty the contents of the stomach after intubation and also before extubation.
Hemodynamic instability was defined as “HR and blood pressure fall or rise more than 20% from baseline” and will be treated accordingly. Systemic arterial pressure including the systolic, diastolic, and mean arterial pressure, HR, and SpO2 was recorded.
Preoperative
After induction with propofol
Immediately after endotracheal intubation
One minute after endotracheal intubation
Three minutes after endotracheal intubation
Five minutes after endotracheal intubation
Ten minutes after endotracheal intubation
Fifteen minutes after endotracheal intubation
Thirty minutes after endotracheal intubation.
Reversal of muscle relaxation was done with injection glycopyrrolate 0.01 mg/kg body weight and injection neostigmine 0.05 mg/kg and the patient was extubated.
Postoperatively, all episodes of PONV and drowsiness experienced by the patient during the first 6 h after anesthesia were recorded. Rescue antiemetic (injection of ondansetron 4 mg) was used if the patient had nausea or vomiting and the number of doses required was monitored. Postoperative pain and sedation of the patient were monitored for 6 h using the Visual Analog Scale (VAS) and the Ramsay sedation score, respectively.
Pain quantification was done on a modified VAS score between 0 and 10 (0 = no pain to 10 = worst imaginable pain).
The pain scores and sedation scores were recorded preoperatively, after extubation then at 1, 2, 4, and 6 h.
The following parameters will be assessed:
The hemodynamic parameters HR Systemic blood pressure (systolic, diastolic, and mean arterial pressure) Peripheral oxygen saturation and Any changes in electrocardiogram (ECG) Pain (VAS score) Time to request the first dose of analgesia Total analgesic consumption in 24 h.
Statistical analysis
The test of Chi-square test was solicited for comparing the frequency. The P value is standardized as, <0.05 was considered to be significant and crucial. We used the software SPSS version 25 (Statistical Package for the Social Science SPSS Inc., Chicago, IL, USA) for statistical analysis. T-test was used for comparing the two groups.
OBSERVATION AND RESULTS
The mean age of patients in the clonidine group was 43.72 ± 11.31 years and the mean age of patients in the gabapentin group was 43.98 ± 11.18 years. Our study enrolled 70% female and 15% male patients in the clonidine group and 76% of females and 24% males in gabapentin group.
On analysis [Table 1], the clonidine group showed better control of HR variation intraoperatively than the gabapentin group. The difference was found to be significant after propofol, immediately after laryngoscopy, and at 1, 2, 3, 4, and 5 min.
Comparison of mean heart rate

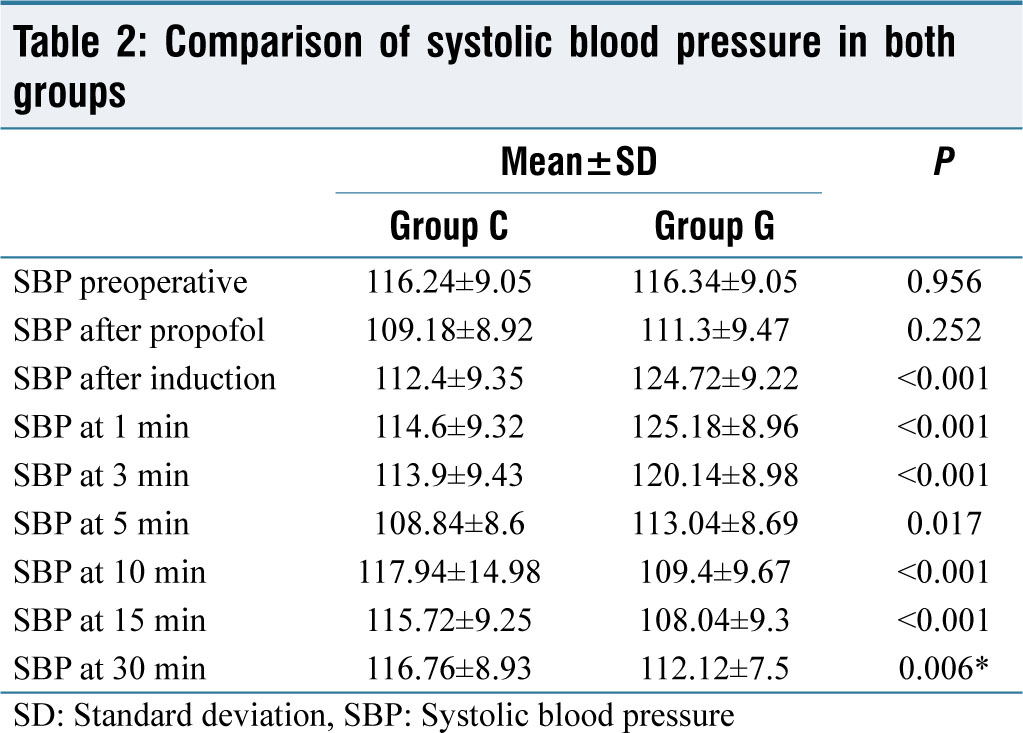
In [Table 2] comparison, fewer changes in systolic blood pressure (SBP) were observed in the clonidine group than gabapentin group. The difference was statistically significant just after induction, at 1, 3, 5, 10, 15, and 30 min.
Comparison of systolic blood pressure in both groups
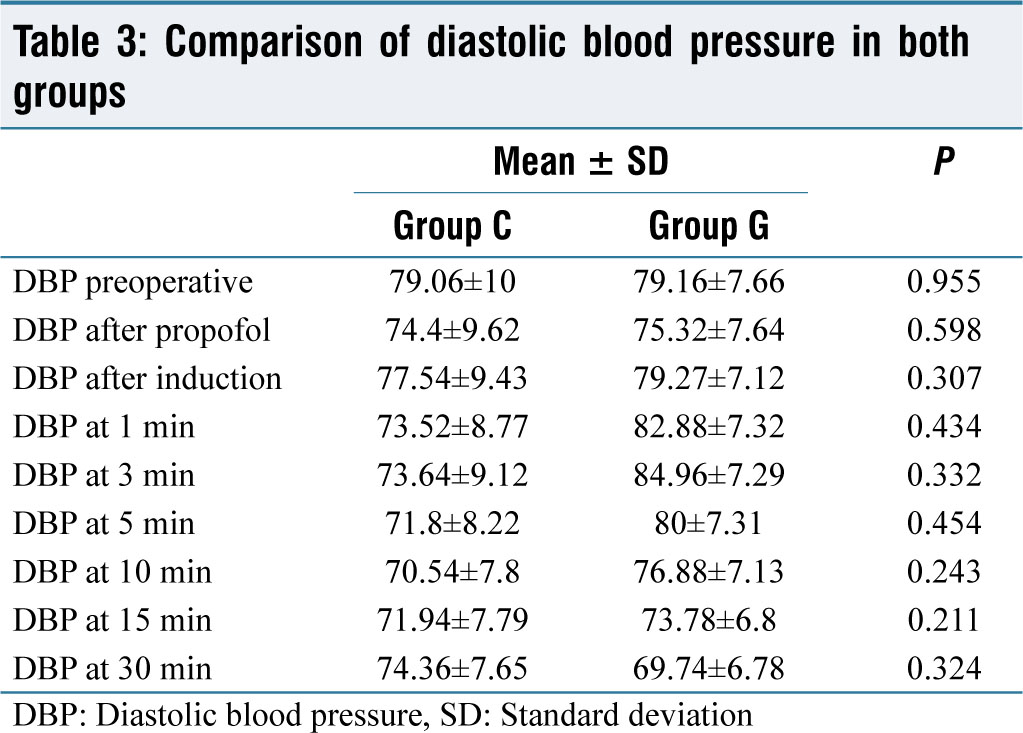
Better control of changes in DBP was observed with the clonidine group [Table 3]. The difference was seen to be significant at 1, 3, 5, and 10 min of induction.
Comparison of diastolic blood pressure in both groups
No significant difference was observed in spO2 between the two groups at any point in time.
The gabapentin group showed a better postoperative analgesic profile than clonidine, which was statistically significant after 6 h of surgery as shown in Table 4.
Comparison of Visual Analogue Scale score in both groups
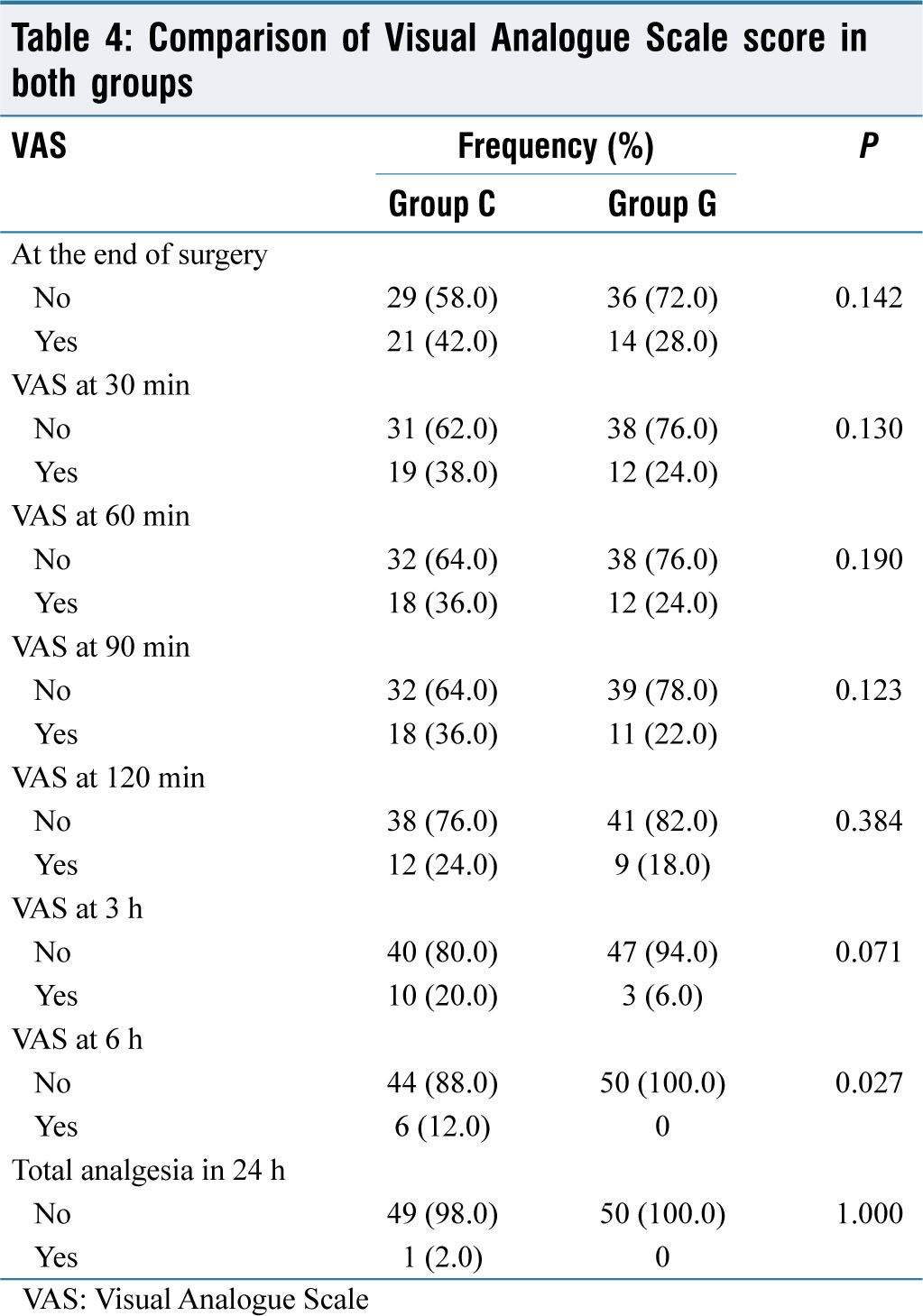
No significant difference was seen in the total analgesic consumption in both groups.
DISCUSSION
In our study, the mean age of patients in the group receiving clonidine was 43.72 ± 11.30 years and the mean age of patients in the group receiving gabapentin was 43.92 ± 11.178 years. There was no statistically significant difference between both groups (P > 0.05). Thus, removing any confounding factor generated by the same.
In our study with 50 patients in each group, it was observed that the group which received clonidine had 35 female patients and 15 male patients. This was similar to the group which was given gabapentin which had 38 female patients and 12 male patients.
In the present study of patients who were posted for elective laparoscopic cholecystectomy all the participants were ASA Grade I or II.
Baseline parameters
In our study, the baseline HR (per minute) in the group that was given clonidine was 79.66 ± 7.32 and in the group receiving gabapentin was 80.78 ± 7,755. The baseline SBP (mmHg) in the group receiving clonidine was 116.24 ± 9.04 and in the group receiving gabapentin was 114.34 ± 9.05. Baseline DBP (mmHg) in the clonidine group was 79.06 ± 9.99 and in the gabapentin group was 79.16 ± 7.65. The difference between the two groups was statistically not significant in all the baseline parameters.
Hemodynamic variations
In contrast to our present study, Fassoulaki et al.[17] demonstrated in their study of 46 participants posted for gynecological procedures, that even at a dose as high as 1600 mg gabapentin failed to show any effect on hemodynamic responses, i.e. HR and mean arterial pressure (MAP). Gabapentin was however found to reduce the variation in systolic and DBP after L and I in comparison to the placebo group patients. However, our study showed delayed attenuation of HR at half the dose of gabapentin. Some possible reasons for this difference in results might be the usage of different drugs for L and I like propofol or not using certain drugs like opioids which might have produced varying hemodynamic responses in HR and pressure effects.
Raval and Mehta,[18] conducted a study on 100 patients who were between the ages 18 and 65 years and were ASA Grade I and II. Patients were divided into three groups namely: group A received tablet Clonidine 4 g/kg, Group B that received tablet diazepam 0.2 mg/kg and Group P received a placebo 90 min before surgery with sips of water. It was inferred in their study that clonidine showed marked sedation and anxiolysis compared to placebo but still, it was lesser than tablet diazepam. Overall clonidine had a superior effect over diazepam due to its effect on blunting hemodynamic response due to stress caused by L and I. This finding was in coherence with our present study where clonidine significantly reduced the incidence of tachycardia and hypertension in response to L and I.
Marashi et al.,[19] studied the effect of 200 μg Clonidine and 900 mg Gabapentin and placebo in three equal groups of 75 participants which were given 2 h before induction. In their study, they noted the hemodynamic variations before L and I and after 1, 3, 5 and 10 min of L and I in all three groups. It was concluded that both clonidine and gabapentin significantly blunted the hemodynamic response of L and I. However at 10 min after L and I clonidine produced lesser variations in hemodynamics. In comparison, in our current study, the attenuation caused by Clonidine was far more significant than that of gabapentin. The reason behind this discrepancy might be the failure to standardize the type of surgical procedure (they included general surgical and orthopedic surgical procedures) and the amount of surgical stimulus in their study in all the study participants up till 10 min of performing L and I. Whereas in our present study, only laparoscopic cholecystectomy patients were included.
A randomized double-blind controlled study of oral gabapentin (900 mg) compared with a placebo given 2 h before surgery was conducted by Kumari and Pathania[20] in 78 study participants. Their study also concluded that obtunding of hemodynamic response to L and I occurs only at 7 min with gabapentin. Furthermore, postoperative analgesia was better in patients receiving gabapentin with almost no adverse effects. These findings are also similar to our study.
Postoperative analgesia
It was also found in our study that patients who were given clonidine and gabapentin had better postoperative analgesia effects. Patients given gabapentin showed better management of postoperative pain in comparison to the group with clonidine. The need for rescue analgesia was also comparatively lower in the group with gabapentin.
In concordance with our study result Mathur et al.,[21] conducted a study in 225 patients posted for abdominal surgeries which were divided into three groups of seventy-five each, and observed that when three hundred milligrams of gabapentin or one hundred and fifty micrograms of clonidine was given 90 min before surgery a significant reduction in postoperative pain and need for rescue analgesia was seen as compared with the group that received placebo. Similar to our current study the effect seen with gabapentin was much more significant as compared to clonidine in their study.
Enhanced recovery programs (ERAS)[22] also known as “fast-track” programs have become important in the perioperative management of many abdominal surgeries such as colorectal surgery, vascular surgery, thoracic surgery, and radical cystectomy. Initiated by Professor Henrik Kehlet, in 1990. These programs aim at the modification of physiological and psychological responses to major surgeries, reducing complications and duration of hospital stay, improving cardiopulmonary function, and earlier resumption of daily activities. The salient features of ERAS protocols include better preoperative counseling, avoidance of long duration of perioperative fasting and loading with carbohydrates upto 2 h preoperatively, standard anesthetic techniques and standard analgesic regimens (epidural and nonopioid analgesia), and early recovery.
One of the major advantages that gabapentin and clonidine demonstrated in our current study was postoperative pain relief which ultimately resulted in enhanced recovery, which is an important component of ERAS protocols facilitating early mobilization and reduced hospital stay for the patients. In our study gabapentin showed a better postoperative analgesic profile than clonidine.
Strengths of this study
A large study population (n = 100) was enrolled with similar age and gender distribution that might help generalize the data to similar populations. The inclusion and exclusion criteria were strictly followed during the entire study. The surgical technique was standardized for all the patients. A thorough preoperative assessment was done of all patients. To avoid compounding outcomes, drugs responsible for the change in intraoperative or postoperative hemodynamics as beta-blockers, and diuretics were avoided and other minor parameters like the rate of fluid transfusion were kept similar for all patients. The research protocol was adhered to completely, from the anesthesia techniques, noting the baseline vitals, use of rescue analgesia, monitoring of hemodynamic vitals and other adverse effects such as nausea and vomiting.
Limitations of the study
First since the stress mediators, i.e., endogenous plasma catecholamines level or cortisol levels are responsible for the hemodynamic response there is no method to measure the same in the perioperative period. Second, the study did not include the elderly population. Third, the postoperative pain measurement done via VAS score is a subjective test and depends majorly on the tolerance of the patient. Fourth, since the consumption and effect of the drug significantly depend on the volume of distribution body mass index of patients was not taken into consideration. Finally, since general anesthesia is given along with multiple drugs and inhalational agents responsible for causing changes in hemodynamic parameters and providing an analgesic effect, it was found difficult to keep the usage constant and respond to the same amount of drug with each patient variable. A larger sample size may help in overcoming these limitations.
Future of the study
ASA I and II patients who were having a laparoscopic cholecystectomy under general anesthesia participated in our study. As a result, our research cannot be generalized to high-risk patients, emergency procedures, or laparoscopic cholecystectomy performed under spinal or segmental anesthesia. To validate the findings of our study, we propose bigger randomized control trials in the Indian community.
CONCLUSION
Clonidine (300 μg) causes a greater attenuation of intraoperative hemodynamic stress responses, whereas gabapentin (600 mg) provides superior postoperative analgesia.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
Institute Ethics Committee MMIMSR - Project no IEC 2038.
Funding
Nil.
Author’s contributions
Dr. Megha Tyagi, Ritu Gupta, and Dr. Ram Nandan Prasad had the concept and design of study or acquisition of data or analysis and interpretation of data, Dr. Ajaydeep Singh did drafting the article or revised it critically for important intellectual content, Dr. Arvinpreet Kour concept and design of study or acquisition of data or analysis and interpretation of data along with did the final approval of the version to be published with all modifications.
Acknowledgements
Department of Anaesthesia.