
Abstract
Introduction:
Fractures of the distal radius account for 14% of all fractures to the extremities and 17% of all fractures treated in emergency departments.
Materials and Methods:
An observational study was done with 62 cases of distal radius fracture from July 2021 to June 2022, where all patients with distal radius fracture more than 18 years of age with the physical fitness of surgery of both genders were included in this study. Patients with neurovascular injury and comatose patients were excluded from the study. All cases were fixed with fragment-specific fixation. The data collection instruments used were Constant–Murley score and QuickDASH score and were followed up for 12 months.
Results:
The mean age of the study participants was 39.90 ± 10.84 years. Around 45.2% were female and 54.8% were male. Around 74.2% had road traffic accident and 25.8% had slip and falls. Mean palmar flexion in degrees was 56.77 ± 3.51, mean dorsiflexion in degrees was 62.90 ± 3.21, mean radial flexion in degrees was 17.39 ± 3.11, and mean ulnar deviation in degrees was 23.77 ± 3.76. Around 71% had excellent results and 29% had good results.
Conclusion:
The use of distal radius plating in the treatment of fractures of the distal radius fractures of the wrist has been established as a good and acceptable treatment option.
Introduction
Fractures of the distal radius account for 14% of all fractures to the extremities and 17% of all fractures treated in emergency departments.[1] It is reasonable to anticipate that the number of distal radius fractures will rise as the average life expectancy of the population rises. There appears to be a bimodal distribution of distal radius fractures, with a younger group that sustains relatively high-energy trauma to the upper extremity and an older group that sustains both high-energy and low-energy injuries. The younger group accounts for the majority of distal radius fractures. More women than men are affected by the condition in those age groups that are older. The majority of fractures in younger populations are the result of collisions with motor vehicles, whereas the majority of fractures in older populations are the result of falls.[1]
Over the course of the previous two decades, more refined methods of internal and external fixation, as well as devices have been created. In particular, the utilization of percutaneous pin fixation, external fixation devices that facilitate distraction and palmar translation, and internal fixation with plates and locking screws have all contributed to an improvement in the management of distal radius fractures.[2]
Fractures of the distal radius are among the most common injuries seen by surgeons who treat the upper extremities. When the stabilization of particular articular segments is necessary, fragment-specific fixation may be utilized as an option for the fixation method. Implants that are custom-made for each unique fragment can be used to stabilize radial styloid, volar rims, dorsal walls, dorsal–ulnar corners, and impacted intra-articular fragments. Although these procedures can be technically demanding, they can be employed either on their own or in combination with other fixation techniques to get accurate reductions and favorable functional effects.[3],[4]
Prolonged immobilization with plaster of paris (POP) causes stiffness of the hand. K wire fixation provides early mobilization but doesnot provide rotational stability. Open reduction internal fixation with plating for distal radius fracture provides accurate reduction, rigid fixation, early mobilization, rotational stability, avoid stiffness, and early rehabilitation. Our study aims to analyze, the functional outcome for fragment-specific fixation of distal radius fracture.
Materials and Methods
After obtaining institutional ethics clearance, an observational study was done from July 2021 to June 2022 with 62 cases of distal radius fractures. All patients with distal radius fracture more than 18 years of age with the physical fitness of surgery of both genders were included in this study. Patients with neurovascular injury and comatose patients were excluded from the study. All cases were fixed with fragment-specific fixation under either general anesthesia or regional block. The data collection instruments used were Constant–Murley score and QuickDASH score and were followed up for 12 months. The data were collected, inputted, and analyzed using SPSS version 26, which was developed by IBM in Chicago, Illinois, in the United States of America. The mean and standard deviation were used to describe continuous variables, whereas the proportion was used to summarize categorical variables such as gender.
Results
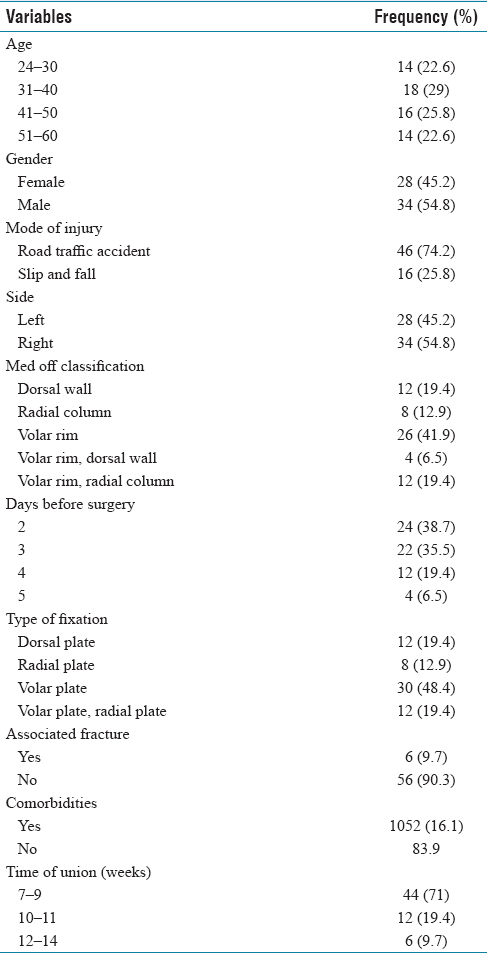
The demographic variables are tabulated in [Table 1], whereas the mean range of wrist movements was tabulated in [Table 2]. Around 71% had excellent results and 29% had good results using Constant–Murley score. The QuickDASH score gives about 75% excellent results and 25% good results, as shown in [Figure 1]. The representative case with distal radius fracture with fragment-specific plate and K wire fixation is depicted in [Figure 2]a, [Figure 2]b, [Figure 2]c.
Distribution of study variables among the study participants (n=62)
Distribution of descriptive variables among the study participants (n=62)

Distribution of results among the study participants (n = 62)

(a) Plain radiographs of right wrist depicting comminuted intra-articular fracture of the distal radius, (b) Immediate postoperative radiograph of right wrist showing fracture fixation with fragment specific fixation with distal radius plate and K wires, (c) 10 weeks postoperative X-ray right wrist after removal of K wires with distal radius plate in situ

Discussion
The necessity of restoring anatomical alignment and articular congruity in the treatment of distal radial fractures is generally recognized and accepted. Malalignment, on the other hand, can lead to lower grip strength, a limited range of motion, and instability. Intra-articular incongruity has been shown to correlate with posttraumatic arthritis.[5],[6]
It is common knowledge that proper restoration of anatomical alignment and articular congruence is essential for the successful repair of distal radial fractures. Malalignment, on the other hand, might result in decreased grip strength, a restricted range of motion, and instability 36. Intra-articular incongruity has been demonstrated to correlate with posttraumatic arthritis. Fractures of the distal radius provide a unique set of fixation concerns that are distinct from those of most other sites. These problems cannot be solved using the same methods as those used for other fractures. Extremely minute and periarticular distal pieces are detected. It is impossible to utilize substantial plates since they would be in close proximity to a thick network of tendons and retinal sheaths. The distal fragments do not have sufficient thickness to ensure adequate thread engagement for bone screws. The objective of the study is to investigate and evaluate the significance of the role those functional outcomes play in the success of fragment-specific repair of distal radius fractures.[7]
Abraham Colles was the first person to ever describe a distal radius fracture, which he did in the year 1814.[8] The distal end radius fracture is the most common type of fracture to occur in the upper extremities, accounting for 17% of all fractures and 75% of all forearm fractures. It is also the most common type of fracture to occur in the lower limbs. It is unfathomable that this particular fracture is one of those that pose the most challenge for the surgeon to treat. The primary objective of treatment for intra-articular fractures is the anatomical reduction of the joint surface, which is then followed by rigid fixation of the fractured area. It has been proven that posttraumatic arthritis can develop over the course of time from residual intra-articular incongruity. As a result of research carried out in recent years, there is now a greater comprehension of the anatomy and function of the wrist, which has led to an expansion of the range of conditions that can be treated surgically. In addition, patients now have higher standards for themselves, which has resulted in a rise in the number of people seeking surgical treatment for medical conditions.
In our research, 22.6% of the participants were between the ages of 24 and 30 years, 29.0% were between the ages of 31 and 40 years, 25.8% were between the ages of 41 and 50 years, and 22.6% were between the ages of 51 and 60 years. The average age of the participants was 39.90 ± 10.84 years old. There were around 45.2% females and 54.8% males in the sample. According to the findings of the research conducted by Paramesha and Bansal,[9] the majority of cases in their study involved younger patients who required surgery as a result of high-energy trauma and road traffic accident (RTA). These findings are comparable to the findings of our investigation. According to our research, approximately 74.2% of people have been involved in car accidents, and 25.8% have been injured in falls.
Medoff[3] developed a hybrid method of percutaneous wire and plate fixation to fix individual fracture pieces by the use of many tiny incisions. This method was named the “Medoff technique.” According to the findings of our research, about 19.4% were classified as having a dorsal wall, 12.9% as having a radial column, 41.9% as having a volar rim, 6.5% as having a volar rim and a dorsal wall, and 19.4% as having a volar rim and a radial column. In a study that was conducted by Jawed et al.,[10] the researchers discovered that 23% of patients developed difficulties. These consequences included malunion, chronic discomfort, stiffness, and paresthesia with tingling. Complications including complex regional pain syndrome, avascular necrosis, distal radioulnar joint syndrome, instability, and paresthesia were documented by Saw et al.[11]
When a conventional volar plate is employed, there is a possibility that up to 13% of lunate facet fractures will no longer reduce.[12] In the event that a volar plate is utilized, it is possible that it will be necessary to position it at a great distance to collect the fragment. As a direct consequence of this, discomfort caused by the hardware is widespread in this region and may be present in as many as 41% of fractures.[13] According to the findings of our research, almost 19.4% of patients had volar plate fixation, 12.9% had radial plate fixation, 48.4% had dorsal plate fixation, and 19.4% had both volar and radial plate fixation.
In a study that was conducted by Paramesha and Bansal,[9] it was shown that 31 patients had fracture union within 3 months, and 30 patients returned to their activity levels before the accident within 6 months. According to our research, 71% of respondents had unions that lasted 7–9 weeks, 19.4% had unions that lasted 10–11 weeks, and 9.7% had unions that lasted 12–14 weeks.
According to the findings of a study conducted by Ganesan and Mohan,[14] the average degree of palmar flexion was found to be 57.1 ± 3.5, dorsiflexion was 63.3 ± 3.2, radial deviation was 17.6 ± 3.0, and ulnar deviation was 24.1 ± 4.4. In our research, the mean palmar flexion was measured in degrees 56.77 ± 3.51, the mean dorsiflexion was measured in degrees 62.90 ± 3.21, the mean radial flexion was measured in degrees 17.39 ± 3.11, and the mean ulnar deviation was measured in degrees 23.77 ± 3.76.
Fractures of the distal radius are a common type of injury seen by surgeons who specialize in the upper extremities. In situations where the stability of specific articular segments is essential, fragment-specific fixation may be utilized as a treatment option. Those fragments of the radial styloid, volar rim, dorsal wall, and dorsal–ulnar corner as well as the intra-articular fragments that have been impacted can be stabilized with implants that have been created individually for each component. In spite of the fact that these procedures might be technically hard, they can be employed on their own or in concert with other fixation techniques to accomplish accurate reductions and yield favorable functional effects.
Conclusion
The minimally invasive and highly efficient treatment for displaced intra- and extra-articular fractures of the distal radius that do not include extensive articular and metaphyseal comminution is called fragment selective fixation of the distal radius. According to the findings of our research, fragment-specific fixation is a versatile method that offers functional outcomes that are superior to those obtained with traditional K wire fixation and comparable to those obtained with volar plating. To provide suggestions for the future, however, additional study with a bigger sample size is necessary.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
TMCH/IEC/2021/046.
Funding
Nil.
Author's contribution
All authors equally contributed for the manuscript.