
Abstract
Objectives:
The objectives of the study are to assess the prevalence and type of sexual dysfunction (SD) in males and females living with diabetes mellitus and to further assess erectile dysfunction in males who score more than 10 points in the Arizona Sexual Experience (ASEX) scale with help of the International Index of Erectile Function-5 (IIEF-5) scale.
Materials and Methods:
An observational cohort study was conducted on 153 diabetic patients visiting SGRDIMSR hospital, Vallah, Sri Amritsar in the Punjab region of North India. Patients aged between 18 and 50 years who were sexually active and in a healthy sexual relationship with their partner were included in the study after an informed consent. ASEX score was used for the assessment of SD and males who score more than 10 points were further assessed for erectile dysfunction with the help of IIEF-5 scale. SPSS Statistics for Windows, Version 23.0. Armonk, NY, USA: IBM Corp., Chicago, was used for data analysis.
Results:
SD was prevalent in 64.05% (n = 98) of study participants overall, 65.9% (n = 5) in female and 61.5% (n = 40) in male groups, respectively. Mean scores of each sexual domain were drive (3.85 ± 1.10) > overall satisfaction (3.34 ± 1.06) > orgasm (3.14 ± 0.96) > arousal (3.11 ± 0.84) > erection/lubrication (2.65 ± 0.82) in that order. 69.84% of male diabetic had some degree of erectile dysfunction as assessed further by IIEF-5 score. The prevalence of SD was found to be higher in patients belonging to elderly age group (P = 0.001), longer duration of diabetes (P = 0.001), and deteriorating glycemic control (P = 0.001).
Conclusion:
Diabetes-related SD is quite prevalent in diabetic patients with 6 out of every 10 patients experiencing this problem. Thus, sexuality needs to be discussed frequently and openly with diabetic patients. In our study, factors such as elderly age of the patient, longer duration of diabetes, and worsening glycemic control of the patient are found to increase the prevalence of SD. Furthermore, the prevalence is higher in patients who already have existing complications of diabetes such as neuropathy, retinopathy, or albuminuria.
Introduction
Diabetes mellitus is a clinical syndrome that consists of metabolic defects characterized by hyperglycemia which results from decreased secretion of insulin, its actions, or both.[1] On an estimate, 537 million adults between 20 and 79 years of age are currently living with diabetes in the world. The world burden of diabetes is expected to rise up to 643 million (11.3%) by 2030 and to 783 million (12.2%) by 2045.[2] The deleterious effects of chronic hyperglycemia manifest in the form of well-known microvascular and macrovascular complications such as neuropathy, nephropathy, retinopathy, coronary artery disease, and stroke. However, the disease of diabetes is not merely limited to these complications and has a lot more to it.[3] The American Diabetes Association states that the Standards of Medical care in Diabetes Mellitus should include evaluation of diabetic patients for sexual dysfunction (SD) also.[1]
Sexuality is a complicated process and a multidimensional phenomenon in which multiple, psychological, interpersonal, biological, and behavioral aspects are involved.[4] The sexual response cycle can be divided into five interrelated events that follow one another in a standard continued sequence. The five sequential events are desire/libido, erection/lubrication, ejaculation, orgasm, and detumescence.[5] The World Health Organization defines the term SD as the various ways in which an individual is unable to participate in a sexual relationship as he/she would wish.[6]
Multiple pathogenic mechanisms can explain SD brought on by diabetes. These include vascular microangiopathy, endothelial dysfunction, hormonal imbalance, and hyperglycemia-mediated neurological damage due to production of advanced glycation end products and reactive oxygen species leading to oxidative stress.[7] In males, major factors responsible for SD are neuropathy, macroangiopathy, and microangiopathy. On the other hand, in females, major factors responsible for SD include hypogonadism, hypoactive desire, dyspareunia, infections, vascular, neurological, and psychological diseases.[8]
SD in diabetes is often unattended by the patients themselves and their physicians. In addition to societal barriers, lack of availability of complaint channels and treatment options for the patients, one major factor is inadequate attention of health-care personnel on sexual health of their diabetic patients.[9]
Materials and Methods
This observational cross-sectional study was conducted in Department of Medicine, SGRDIMSR, Vallah, Sri Amritsar from April 2021 to July 2022. Plan of study was approved by Academic Council in its meeting held on 07-06-2021 with Ref no. SGRDU/Cont/thesis/21-520. Project was approved by ethical committee after scrutiny with Ref no. Ant/69/2021. Patients of diabetes mellitus were diagnosed according to the American Diabetes Association criteria and included in the study after taking an informed consent. Patients in the study were recruited from both outpatient and inpatient departments of the hospital. Only sexually active patients between 18 and 50 years of age, having history of diabetes mellitus from at least 6 months, and having normal emotional relationship with their partner were included in the study. Patients with history of spinal trauma/surgery, thyroid disorder, end-stage renal disease or liver disease, psychiatric illness, or on medications that may cause hypogonadism (beta blockers, SSRI, testosterone, steroids, etc.) were excluded from the study.
The study participants were assessed for SD with help of the Arizona Sexual Experience (ASEX) score. The males who scored more than 10 points on ASEX scale were further assessed for erectile dysfunction with help of the International Index of Erectile Function-5 (IIEF-5) scale. ASEX scale and IIEF-5 scale were translated in Punjabi and Hindi languages and their content and face validity were maintained. Relevant clinical history and examination for neuropathy, retinopathy, and investigation for nephropathy were also done of all the study participants. SPSS Statistics for Windows, Version 23.0. Armonk, NY, USA: IBM Corp., Chicago, were used for data analysis.
Results
In study population, SD was found in 64.05% participants with the prevalence of 65.9% in females and 61.5% in males.[Table 1].
Prevalence of sexual dysfunction among diabetics

The prevalence of SD in higher (41–50 years) age group was 75.26% among females, 67.27% among males, and 71.21% among overall study population.
This was significantly higher as compared to the prevalence in lower age groups.
The prevalence of SD in higher (41–50 years) age group was 75.26% among females, 67.27% among males, and 71.21% among overall study population [Figure 1] and [Table 2].
Age-wise prevalence of sexual dysfunction
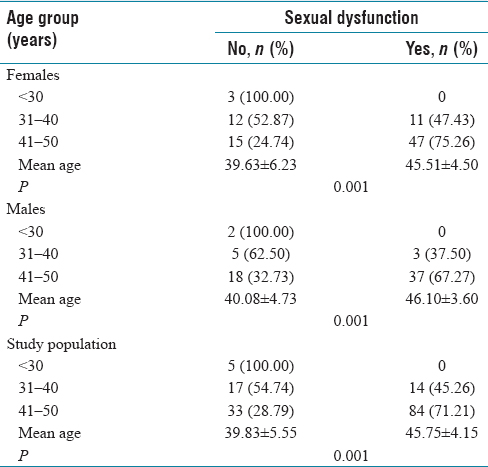
Prevalence percentage of sexual dysfunction in each age group

This was significantly higher as compared to the prevalence in lower age groups.
The prevalence of SD in participants with longer duration (>10 years) of diabetes was 88.00% among females, 91.70% among males, and 89.30% among overall study population. [Figure 2] and [Table 3].
Prevalence of sexual dysfunction according to duration of diabetes

Prevalence percentage of sexual dysfunction according to duration of diabetes

This was significantly higher as compared to the prevalence in lower age groups.
The prevalence of SD was higher in patients with longer duration of diabetes and also the mean duration of diabetes was higher in SD group as compared with no dysfunction.
Among the 67 patients found with neuropathy in our 153 participants, majority 92.54% (62 out of 67) had coexisting SD with significant correlation between neuropathy and SD (P = 0.001) [Table 4].
Prevalence of sexual dysfunction in patients with complications of diabetes

54 patients out of 153 in our study were diagnosed with retinopathy. Among them, majority 85.75% (46 out of 54) had coexisting SD with significant correlation between retinopathy and SD (P = 0.001) [Table 4].
The prevalence of SD among participants in KDIGO A3 was 86.66% (26 out of 30) as compared to 68.75% (33 out of 48) in KDIGO A2 and 52.00% (39 out of 75) in KDIGO A3. Significant correlation was present between SD and albuminuria with P value 0.003.
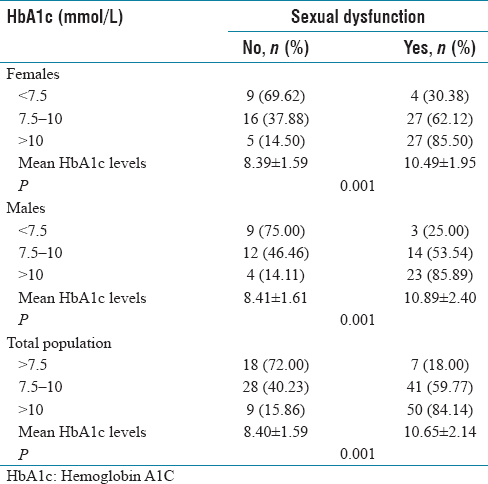
The prevalence of SD in participants with uncontrolled diabetes with higher (>10 mmol/L) Hemoglobin A1C (Hba1c) levels was 85.50% among females, 85.89% in males, and 84.14% among overall study population. This was significantly higher as compared to the prevalence in better control of diabetes (lower Hba1c groups) [Figure 3].
Percentage prevalence of sexual dysfunction in various hemoglobin A1C groups

The prevalence of SD among female with uncontrolled diabetes (HbA1c>10%) was higher as compared to poorly controlled diabetes group (HbA1c 5%–10%) and fair glycemic control group [Table 5].
Percentage prevalence of sexual dysfunction in various glycated hemoglobin groups
Overall mean score was highest for drive domain which was 3.92 in females, 3.84 in males, and 3.85 in overall population.Hence, drive was most affected domain [Figure 4]. Other domains had scores, as shown in [Table 6].
Mean scores of various domains of sexual cycle
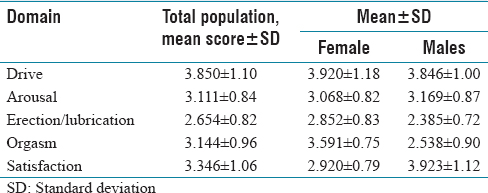
Mean scores of various domains of sexual cycle

Drive>overall satisfaction>orgasm>arousal>erection/lubrication was type of SD in study participants prevalent in that order. Drive>orgasm>arousal>overall satisfaction>lubrication was type of SD among female. Satisfaction>drive>arousal> erection>orgasm is type of SD among male [Figure 4].
Males with severe erectile dysfunction belonged to older age group and had higher mean age 49.66 ± 0.57 as compared to males with less severe degree or no erectile dysfunction who belonged to younger age groups and had lower mean age and there was significant correlation between age and degree of erectile dysfunction (P = 0.001). Longer the duration of diabetes, more severe was the degree of erectile dysfunction among males with significant correlation between duration of diabetes and degree of erectile dysfunction (P = 0.001). Poorer glycemic control was also associated with severe degree of erectile dysfunction and fair glycemic control was associated with less severe SD with significant correlation between severity of erectile dysfunction and Hba1c levels (P = 0.037) [Table 7].
Erectile dysfunction evaluated using the International Index of Erectile Function-5 score

Discussion
SD is a frequently experienced health problem worldwide with diabetes being one of its causes. However, unfortunately, this aspect of diabetes-related complications is frequently overlooked and ignored. Hence, this study was conducted to make assessment of sexual health problems in diabetic patients in our region. Among female group, our study observed 65.9% prevalence of SD which is almost similar to an Indian study by Nagpal and Jangid,[10] who studied 100 diabetic women and found 62% prevalence and also in alignment to a recent foreign study by Paningbatan et al.[11] with 72% prevalence. Comparable to 61.5% prevalence of SD among men in our study, Getie Mekonnen et al.[12] found it to be 69.5% in their study. However, contradictory to our observation, the study conducted by Dan et al.[13] showed a lower prevalence of 39%. The reason behind varied results may be due to different study designs and the variation in the methodology adopted by these studies and also the influence of multiple locoregional, societal, geographical, and dietary factors on the result.
In our study, the prevalence of SD was 75.26% among female and 67.27% among male in elderly (41–50 years) age group as compared to 47.43% among females and 37.50 among males in 31–40-year age group. Mean age of participants with SD was also higher, 46.14 ± 3.78 years, as compared to 41.12 ± 5.19 years in participants with no SD. Similar to our study, Bellad and Sahu[14] concluded that mean age in patients with SD was significantly high (58.40 ± 10.96 years) as compared to those without SD (51.00 ± 11.16 years). Our observation was also consistent with studies of Rutte et al.[15] and Tuncel et al.[16]
The prevalence of SD among female group and male group with longer (>10 years) duration of diabetes was 88% and 91.7%, respectively, as compared to 70.35% and 58.97%, respectively, in 5–10-year duration group and 31.09% and 23.25%, respectively, in < 5-year duration group. Similarly, Hurisa et al.[17] in their study of 350 male diabetic patients found that SD was significantly associated with longer duration of diabetes (adjusted odds ratio [AOR]: 3.5; 95% confidence interval [CI]: [2.12–5.70]; P < 0.001).
Age and duration of diabetes are, however, nonmodifiable risk factors of SD and are not amenable to medical intervention.
SD among participants with poorer glycemic control as estimated by Hba1c levels of > 10% was as high as 85.50% and 85.89%, respectively, among female and male groups as compared to as low as 30.38% and 25% among female and male groups, respectively, in fair glycemic control group (HbA1c of 5%–10%) [Table 5]. Our observations were consistent with results of various previous studies like that of Kaya et al.[18] and were also enforced by Ozcan et al.[19] who stated that an one unit increase in HbA1c value caused 19.1% of increase in SD, 23.2% on drive, 20.7% on satisfaction, and 17.5% on orgasm.
Our study observed high prevalence of SD among diabetic patients who were already living with any form of complication of diabetes such as diabetic nephropathy, neuropathy, or retinopathy, and our observations are well supported by the findings of various previous studies of Gandhi et al.,[8] Vafaeimanesh et al.,[20] Binmoammar et al.,[21] Ugwu et al.,[22] Alshehri et al.,[23] and Gupta et al.[24]
Drive > overall satisfaction > arousal > orgasm > erection was type of SD among males and drive > orgasm > arousal > overall satisfaction > lubrication was type of SD among females in our study. However, contrary to our study, orgasm disorder and arousal were domains most affected in study by Getie Mekonnen et al.[12] whereas lubrication and orgasm were domains most affected in study by James Paningbatan et al.[11] With similarity to our study, drive, arousal, lubrication, satisfaction, and orgasm were domains affected in that order in study of Rahmanian et al.[25] These differences may be due to various locoregional influences, intricating and difficult to understand definitions of various components of sexual cycle.
In our study, on assessing erectile dysfunction using IIEF-5 score, it was found in as many as 69.84% of male diabetic subjects. Our study findings were consistent with that of Tamrakar et al.[26] who found 76.87% of ED and Ghanem et al.[27] who found 80% of ED.
Our study showed that males with severe erectile dysfunction had a higher mean age of 49.66 ± 0.57 years as compared to males with a less severe degree or no erectile dysfunction, with a significant correlation between age and degree of erectile dysfunction (P = 0.001). These findings were in agreement with the study of Bahar et al.[28] who say that ED was 11.21 times more prevalent in above 50 year group as compared with those below 50 years of age. Previous studies of Shakya et al.,[29] Zeleke et al.,[30] and Parmar et al.[31] all supported our result.
The duration of diabetes significantly influences (P = 0.001) erectile dysfunction in our study. This is in line with conclusion of Hurisa and Negera[17] who found that longer duration of diabetes was related to SD (AOR: 3.5; 95% CI: [2.12–5.70]; P < 0.001) and it was independent predictor of ED. Many other recent studies such as Bal et al.[32] and Ugwu et al.[22] had similar conclusions.
Another important finding of our study was that the patients with higher Hba1c levels (uncontrolled diabetes) had severe erectile dysfunction with lower mean IIEF-5 score as compared to those with relatively better glycemic control [Table 7]. Binmoammar et al.[21] in his study looked at the relationship between type 2 diabetic men's glycemic control and ED and reported that the mean HBA1c was greater among individuals with ED than those without ED. Another study by Ramanathan[33] supports this association.
Conclusion
We would like to conclude that in our study, SD as assessed by ASEX score was prevalent in significant proportion of diabetic patients and it was found to affect 6–7 out of every 10 diabetic patients. There was significant association of SD with age, duration of diabetes, and the level of glycemic control as participants in elderly age group (41–50 years), longer duration of diabetes (>10 years), and uncontrolled diabetes (HbA1c > 10%) were found to have higher prevalence of SD. Age and duration of diabetes are nonmodifiable risk factors. On the other hand, glycemic control is the factor that is modifiable and may help to reduce the prevalence or at least delay this complication related to diabetes. In our study, diabetics with already existing complications such as nephropathy, neuropathy, or retinopathy were observed to have significantly higher prevalence of SD also. As far as domains of sex are concerned, drive was the most affected domain and it was equally affected among both male and female groups. Problem of lubrication among females was more obvious than the problem of erection among males. Inability to reach orgasm was complaint of females as compared to males. Overall, satisfaction was problem among males. ED, when assessed by IIEF-5 scale, was prevalent in almost 70% males and it was also associated significantly with age, duration of diabetes, and glycemic control. Hence, a multidisciplinary approach should be followed to reach the ultimate goal of comprehensive diabetic care and referral to gynecologists, psychiatrists, and sexologists should also be considered for diabetic patients.
Footnotes
Acknowledgements
First of all, thanks to my genius mentor, guiding light, Dr. Gurinder Mohan without whom not a part of the study could have been possible. Also thanks to Dr. Tejinder Sikri who guided the study. Special thanks to my parents and friends Dr. Pardeep Kumar, Dr. Kapeesh Khanna, Dr. Simranpreet Kaur, and Dr. Guramrit Singh.
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
Plan of study was approved by Academic Council in its meeting held on 07-06-2021 with Ref no. SGRDU/Cont/thesis/21-520.
Project was approved by ethical committee after scrutiny with Ref no. Ant/69/2021.
Funding
Nil.
Author's contribution
Dr. Gurbir Singh Mann: Critical revision of the article and final approval of version to be published.
Dr. Gurinder Mohan: Conception of the idea, drafting the article, critical revision of the article.
Dr. Tejinder Sikri: Revision of article.