
Abstract
Background:
Dementia is a condition of elderly individuals, marked with emotional and cognitive disabilities which are severe enough to impair their routine daily life and its quality. It is mainly a disease affecting elderly population with an approximate prevalence rate of 1% at the age of 60 years and quadruples every 10 years, up to 30%–50% by the age of 85 years. There are about 5.5 crore people suffering with dementia with more than 60% in developing countries.To overcome this, a multipronged strategy with timely diagnosis is the need of the hour.
Materials and Methods:
The present study was conducted at the Department of Radiodiagnosis and Department of Psychiatry of J. N. Medical College and Hospital, Aligarh, over a period of 2 years. Forty-five patients in the age group of more than 55 years who presented with the complaints of cognitive impairment and were referred for magnetic resonance imaging (MRI) head after clinical examination and Mini–Mental State Examination (MMSE) score assessment were included in the study. On MRI images are assessed using the Global Cortical Atrophy (GCA) scale, medial temporal lobe (MTL) atrophy scale, and Fazekas Scale, then findings are correlated with clinical MMSE scores.
Results:
There were 45 patients with the age group of more than 50 years, among 66.67% of patients were males and 33.33% of patients were females. In 60.00% of patients, socioeconomic status was lower middle class, 46.67% of patients were illiterate followed by studied till primary school (22.22%). In 66.67% of patients, mini–mental score examination score was mild. Among the imaging scales, 82.22% of patients showed moderate GCA scale; in 55.56% of patients, interpretation of MTL atrophy scale was widening of choroid fissure and temporal horn of lateral ventricle. 33.33% of patients showed Fazekas 3 Scale with large confluent lesions. All these imaging scales showed a significant negative correlation with MMSE scores.
Conclusion:
MRI plays an important role in the assessment of structural changes in patients presenting with cognitive impairment as well as it points toward the diagnosis of certain type of dementia depending on the involvement of specific areas or lesions and their distribution in the cerebral hemispheres. Visual assessment using various scales has helped in assessing the severity as well as possible type. There has been establishment of significant correlation between the MRI scales of atrophy and clinical MMSE scoring system.
INTRODUCTION
Dementia is a chronic and progressive syndrome which leads to cognitive function deterioration beyond what is usual for that biological age. It affects memory, orientation, thinking, calculation, comprehension, language, judgment, and learning ability. The consciousness is preserved. The cognitive impairment is commonly affected, and occasionally, changes in behavior, emotional control, or mood may precede these changes.[1]
The diagnostic guidelines for dementia include:[2]
Evidence of decrease in memory and thinking which is ample to impair daily living Impairment of memory which typically affects the storage, registration, and new information retrieval with a loss of memory of previously learned and familiar materials in later stages Along with dysmnesia, there will be impairment of thinking and reasoning ability with the reduction of flow ideas Impaired processing of incoming information with increasing difficulty in attending more than one stimulus at a time Evidence of clear consciousness is must for sole diagnosis of dementia The above impairments and symptoms should be evident for at least 6 months for a clear clinical diagnosis of dementia.
Dementia causes of dependency and disability in 5.5 crore older population worldwide, with over 60% in developing countries. This number will rise to more than double by 2050.[1]
As we have mentioned above, Alzheimer’s disease (AD) can manifest either alone or along with associated other illness, accounting for 65%–70% of total cases of dementia. The typical presentation is progressive decline, in memory with 8–10 years of survival rate. AD mainly manifests as short-term memory loss with a cognitive decline. There may be subtle impairment of attention, ability to focus, language impairment, and recall remote events. Language impairment is also seen.[3]
MATERIALS AND METHODS
The present study was conducted at J. N. Medical College and Hospital, AMU, Aligarh, over a period of 2 years from September 2019 to September 2021. The main sources of data for the study are indoor and outdoor 45 patients of both sexes in the age group of more than 55 years who presented with the complaints of cognitive impairment and were referred from inpatient department (IPD)/outpatient department (OPD) of Department of Psychiatry J. N. Medical College and Hospital, Aligarh for magnetic resonance imaging (MRI) head. All elderly patients presenting in OPD/IPD of department of psychiatry with complaints, suggestive of dementia were included in the study. Patients of age group more than 55 years with features of cognitive impairment suggesting dementia were included in the study. The study has excluded treatable causes of dementia and structural brain lesions such as head injury, delirium, seizures, tumors (e.g., meningioma and glioma), subdural hematoma, arteriovenous malformation, hydrocephalous, idiopathic normal pressure hydrocephalous, postoperative cases, patients having a history of claustrophobia, patients with cardiac pacemakers, metallic foreign-body in situ, and in whom MRI is contraindicated. Clinical complaints were noted in all patients with cognitive impairment along with associated comorbidities, and socioeconomic status was decided according to the Modified Kuppuswamy socioeconomic index class, and clinical examination was done to assess the severity of dementia using Mini–Mental State Examination (MMSE).[2] A predetermined standard questionnaire, in vernacular (Hindi) adaption, was administered, and the relevant information was collected by a psychiatrist in a personal interview. Then, patients were subjected to MRI.
Patients were subjected to MRI brain on 1.5T MR Scanner (MAGNETOM Avanto, SIEMENS). Standard head coils were used.
Using a 1.5T MR unit, we obtained:
Axial T1-weighted images with 450/20 TR/TE, ST of 4 mm, an interslice gap of 0.8 mm, a FOV of 187 mm × 231 mm, and a matrix of 208 × 320 T2-weighted SE images with 4940/98 TR/TE, ST of 5 mm, an interslice gap of 0.5 mm, a FOV of 179 × 221, and a matrix of 203 × 384 FLAIR images with 7500/88 TR/TE, slice thickness of 4 mm, a field of view of 202 × 231, and a matrix of 168 × 256 DW images were obtained at b values of 0, 500, and 1000. ADC maps were obtained. We then obtained T1 MPRAGE three-dimensional sequences for the assessment of medial temporal lobe (MTL) in coronal planes We also evaluated susceptibility images to look for microhemorrhages Special sequences such as time of flight (TOF) were used as and when required.
After assessing the structural changes in the entire brain tissue, various scale systems were applied to describe the extent and severity of the atrophy and white matter changes in the brain. Global cortical atrophy (GCA) scale,[4] MTL atrophy scale,[5] and Fazekas scale[6] were used for cortical and white matter changes, respectively. Then, the patient was assessed clinically with MMSE to measure the clinical severity and functional impairment, and final score was assigned based on the performance of the patient in various questions and tasks and categorized as questionably significant, mild, moderate, and severe. All the radiological findings and scores of MMSE were noted down and tabulated, and radiological and clinical findings were compared and correlated.[2]
For statistical analysis, categorical variables were shown in number and percentages. The association of variables was analyzed using Fisher’s exact test, and Spearman’s rank correlation coefficient for MMSE score with GCA, MTA, and Fazekas Scale.
Ethical consideration
Informed consent was obtained individually from the patients/caregivers and the study was approved by Institutional ethics committee.
RESULTS
Among 45 patients, 66.67% were males and 33.33% were females with male-to-female ratio of 2:1. In majority (60.00%) of patients, socioeconomic status was lower middle, followed by upper middle (15.56%), upper lower (13.33%), and lower (8.89%). Socioeconomic status was upper class in only one out of 45 patients (2.22%). The majority (46.67%) of patients were illiterate, followed by studied till primary school (22.22%), high school (15.56%), and middle school (11.11%). Only one out of 45 patients (2.22%) had diploma and professional degree each. The mean value of age (years) of study participants was 67.02 ± 8.2 with median (25th–75th percentile) of 65 [Table 1].
Distribution of sociodemographic characteristics of study participants

In 18 (40.00%) patients, hypertension was present followed by diabetes mellitus (35.56%), Parkinson’s disease (8.89%), obesity (6.67%), and chronic kidney disease (CKD) (4.44%). Depression was present in only one out of 45 patients (2.22%). In the majority (66.67%) of patients, mini–mental score examination score was mild followed by moderate (26.67%) and questionably significant (4.44%). Mini–mental score examination score was severe in only one out of 45 patients (2.22%). The majority (82.22%) of patients showed moderate GCA scale followed by mild (13.33%). GCA scale was severe in only two out of 45 patients (4.44%) [Figure 1].
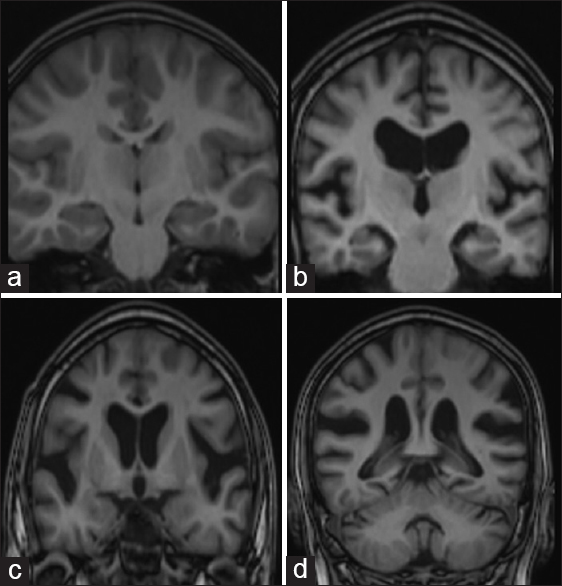
T1-weighted coronal imaging of four different patients showing variable extent of global cortical atrophy (GCA), (a) A 60-year-old patient with no cognitive decline shows normal cortical gyri and sulci with no evidence of atrophy (GCA-0), (b) 62-year-old patient with cognitive decline and Mini–Mental state examination (MMSE) score of 23 shows opening of sulci and GCA-1, (c) 66-year-old patient with MMSE score of 22 showing moderate atrophy with volume loss of gyri (GCA-2), (d) 68-year-old patient with MMSE score of 19 showed severe atrophy (GCA-3)
In the majority (55.56%) of patients, there was widening of choroid fissure and temporal horn of lateral ventricle, followed by moderate loss of hippocampal volume (28.89%) and widening of choroid fissure (8.89%). Interpretation of MTL atrophy scale was severe volume loss of hippocampus in only 3 out of 45 patients (6.67%) [Figure 2].
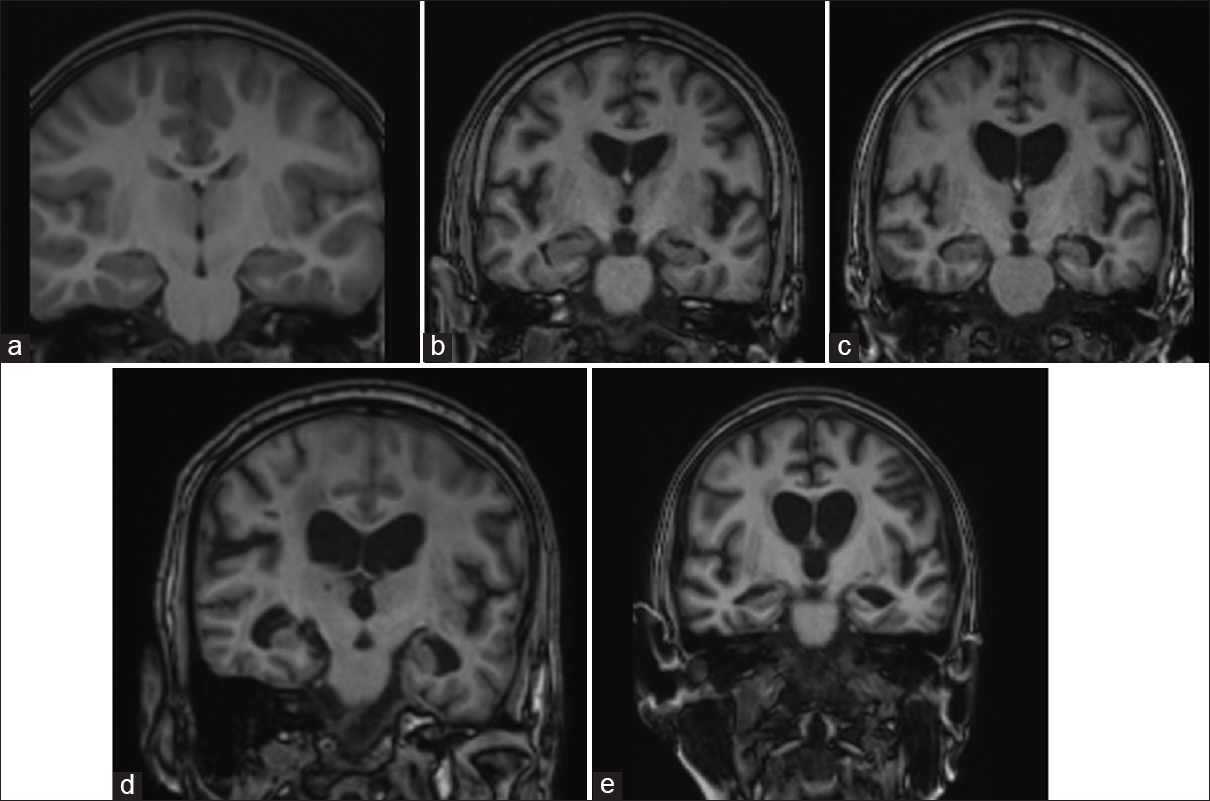
T1-weighted coronal imaging of four different patients showing variable extent of medial temporal lobe (MTL) atrophy, (a) a 60-year-old patient with no cognitive decline shows normal cortical gyri and sulci with no evidence of medial temporal atrophy (MTL-0), (b) a 63-year-old patient with cognitive decline and Mini–Mental state examination (MMSE) score of 22 shows widening of bilateral choroid fissure (MTL-1), (c) a 61-year-old patient with MMSE score of 21 showing widening of bilateral choroid fissure and temporal horns of bilateral lateral ventricle (MTL-2), (d) a 65-year-old patient with MMSE score of 20 showed moderate loss of hippocampal volume with reduced hippocampal height (MTL-3), (e) a 68-year-old patient with MMSE score of 20 showed moderate loss of hippocampal volume with severe hippocampal volume loss (MTL-4)
In33.33% of patients, interpretation of Fazekas scale was large confluent lesions followed by multiple punctate lesions (31.11%). Interpretation of Fazekas scale was none or single punctate white matter lesion and beginning confluency of lesions in only 8 out of 45 patients (17.78%) each [Figure 3].

(a) FLAIR sequence, axial imaging of brain at corona radiata level showing (i) multiple punctate hyperintensities – Fazekas 1 white matter lesions (ii) multiple bridging punctate hyperintensities – Fazekas 2 white matter lesions. (b) Corona radiata level and (c) multiple large confluent hyperintensities – Fazekas 3 white matter lesions
In majority (62.22%) of patients, final diagnosis was AD followed by vascular dementia (VaD) (28.89%), progressive supranuclear palsy (11.11%), and Parkinson’s (dementia with Lewy body) (6.67%). Additional findings were multiple system atrophy dementia and frontotemporal atrophy in only one out of 45 patients (2.22%) each. Distribution of GCA scale was comparable between MMSE score. Proportion of patients with MTL atrophy scale: widening of choroid fissure and temporal horn of lateral ventricle were significantly higher in mild as compared to moderate, severe, and questionably significant MMSE score. Proportion of patients with Fazekas scale: beginning confluency of lesions and large confluent lesions were significantly higher in moderate as compared to mild, severe, and questionably significant. With the Spearman’s coefficient, there was a significant negative correlation was seen between MMSE score with GCA scale, MTL atrophy scale, and Fazekas scale with correlation coefficient of − 0.434, −0.531, and − 0.408, respectively, and P = 0.003, P = 0.0002, and P = 0.006, respectively [Table 2 and Figures 4-6].
Correlation of Mini–Mental State Examination score with global cortical atrophy scale, medial temporal lobe atrophy scale, and fazekas scale

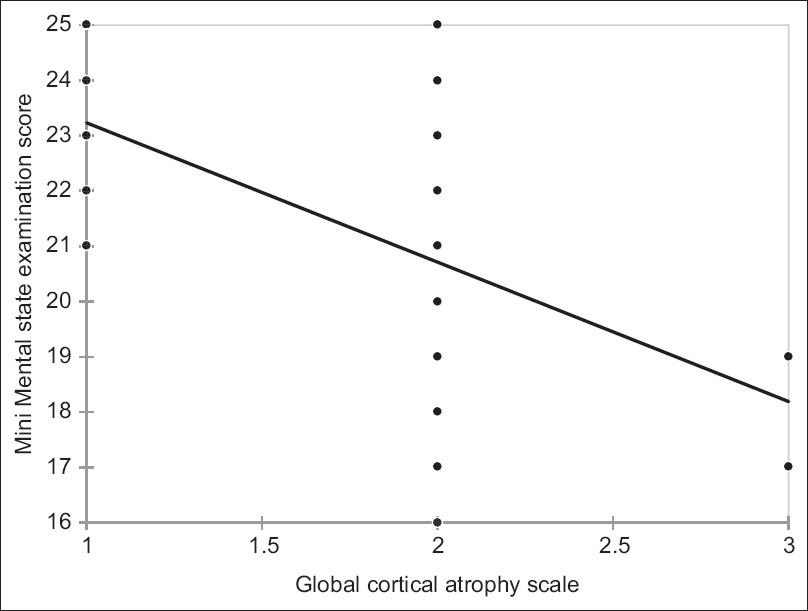
Spearman’s rank correlation coefficient: Correlation of global cortical atrophy scale with Mini–Mental State Examination score

Spearman’s rank correlation coefficient: Correlation of medial temporal lobe atrophy scale with Mini–Mental State Examination score

Spearman’s rank correlation coefficient: Correlation of Fazekas scale with Mini–Mental State Examination Score
DISCUSSION
Dementia is one of the common clinical conditions in the elderly population, and as the population ages, the number of cases will continue to increase. Each patient with cognitive impairment deserves a multimodal assessment and appropriate management. Clinical and neuropsychological assessment is most important for the diagnosis and management of dementia, following this neuroimaging is done to identify the areas of cortical loss and function impairment. Laboratory tests are done to explore the associated comorbidities, risk factors, and treatable cause for dementia.
MRI is the most widely used modality of imaging tool for the evaluation of cognitive impairment as it provides excellent visual assessment of the extent of atrophy.
Forty-five patients with clinically significant cognitive impairment and whose age was more than 50 years were evaluated on conventional magnetic resonance sequences. Findings were correlated with the clinical MMSE scale findings.
Our study included the patients’ age ranging from 50 to 82 years, with a mean of 67.02 years with a median age of 62–73 years. Majority of the patients were in the age group of 60–70 years of age.
Our study showed male predilection (66.67% of males and 33.33% of females) of dementia, whereas many studies have suggested that there is no gender predilection and few suggested that females were more affected than the males. Male-to-female ratio in our study was 2:1. Many studies showed female predilection. This can be explained by the lack of awareness and less availability of primary health-care facilities for women. This might explain the male predilection in our studies. In majority (60.00%) of patients, modified Kuppuswamy socioeconomic index class was lower middle followed by upper middle (15.56%). Saldanha et al., 2010, statistically identified the higher risks for dementia and they were older age, low socioeconomic status, the presence of family history, and low level of education. This study also had used Kuppuswamy’s socioeconomic index for classifying the economical class of the patients with the majority of the patients belonging to lower middle class as in our study.[7,8] The majority (46.67%) of patients in our study were illiterate followed by studied till primary school (22.22%). Many studies such as Sharp and Gatz and Paddick et al., 2014, suggested a strong relationship between the low educational status with dementia. In 40.00% of patients, hypertension was present followed by diabetes mellitus (35.56%), Parkinson’s disease (8.89%), obesity (6.67%), and CKD (4.44%). Depression was present in only one out of 45 patients (2.22%).[9,10] Most common comorbidity in our study was hypertension, especially in AD and VaD. These associations can be due to disorders in the elderly patients affecting blood circulation. Sierra, 2020, has discussed the potential advantage of antihypertensive treatment in preventing cognitive decline.[11] In our study, the most common type of dementia was AD (62.22%), followed by VaD (28.89%), progressive supranuclear palsy (11.11%), and Parkinson’s (Dementia with Lewy body) (6.67%). Ashraf et al., 2016, suggested that AD and VaD, together account for 60%–80% of total dementia cases worldwide and are the most common forms.[12] An Indian study by Das et al., 2012, a review article on dementia in Indian scenario has mentioned a clinical-based study from South India found that AD as most common type (38.3%), followed by VaD (25.4%), frontotemporal lobar dementia (18.7%), and dementia of Lewy body (8.9%).[13]
Our study included various scoring systems assessed on MRI that were correlated with the severity of dementia in clinical MMSE score using Spearman’s correlation coefficient. The majority of the patients, i.e., 25 patients with moderate GCA were having mild category of MMSE score with negative correlation between the GCA and MMSE score, suggesting that high GCA score is seen in patients with low MMSE score, i.e., as the clinical severity increases, GCA score also increases. P <0.05 is considered statistically significant correlation; in our study, the P = 0.003 suggesting a moderate negative correlation between GCA and MMSE scoring system. A similar Indian study by Kaushik et al., 2021, evaluated thirty patients fulfilling DSM 5 criteria for AD and other dementias who were subjected to MRI; subsequently, visual rating scores were correlated with MMSE scale. There was a moderate negative correlation between GCA scores and MMSE scores of all patients. The majority of the patients, i.e., 22 patients with moderate MTL atrophy were having mild category of MMSE score with negative correlation between the GCA and MMSE score, suggesting that high MTL atrophy score is seen in patients with low MMSC score, i.e., as the clinical severity increases, MTL atrophy score also increases.[14] In our study, P value for MTL atrophy and MMSE score correlation was 0.0002, suggesting a strong negative correlation between MTL atrophy scale and MMSE scoring system. In our study, high Fazekas score is seen in patients with low MMSE score with P value for white matter changes, and MMSE score correlation was 0.006, suggesting a moderate negative correlation between Fazekas scale and MMSE scoring system. Tsui-Caldwell et al., 2019, concluded that increased WM findings were significantly associated with the decreased overall MMSE score.[15] In our study, significant negative correlation was seen between MMSE score with GCA scale, MTL atrophy scale, and Fazekas scale with the correlation coefficient of − 0.434, −0.531, and − 0.408, respectively. A similar study by Kaushik et al., 2021, gave similar results as in our studies and concluded that MTL atrophy is a reliable scoring system for detecting and assessing AD and it strongly correlates with clinical memory scores. MTL atrophy and parietal lobe atrophy are specific for AD, whereas symmetric atrophy of frontal and temporal lobe favors frontotemporal dementia.[14]
Another similar Indian study by Chatra et al., 2021, showed statistically significant association between Scheltens et al.’s imaging scores with MMSE. There is a moderately positive linear relationship between the two. There is also evidence that moderate scores of GCA and Fazekas were seen in patients with clinically mild form of dementia, this might indicate that structural changes are seen earlier before the patient presents clinically. This feature can be used as a screening tool in patients with subclinical dementia for early diagnosis and management.[16,17] MRI has many advantages as it is easy to perform, specific features help in diagnosing specific type of dementia which is crucial for the management, whereas molecular studies which are available for the diagnosis of AD are practically not available and cannot be used for the routine diagnosis in all patients because of logistical challenges.[18] MRI gives high resolution with excellent tissue contrast. It is fast, cost-effective, no requirement of contrast material, and can be performed easily on any MRI software. There are many disadvantages of MRI in the assessment of dementia. It is less sensitive as compared to other volumetric-based assessments and is subject to interobserver variations. It was also difficult to differentiate between atrophic changes due to normal aging and those secondary to dementia solely based on MRI imaging findings without the appropriate clinical history.
CONCLUSION
Early detection of dementia on MRI imaging would definitely result in the better management and patient care. It can also be used as a tool for the follow-up of the patients once the treatment has been started to assess the treatment response and the rate of progression of the severity of the condition.
Many researchers have suggested that differentiating MRI features between the atrophic changes due to normal aging process and due to dementia has become challenging and which further needs more sensitive functional imaging modalities, but these advanced modalities are mainly having research significance because of their limited availability and complexity and being not practically possible to use as routine investigation.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
Institutional Ethics Committee of J. N. Medical College, AMU, Aligarh. Certificate NO. D-132/FM/IEC.
Funding
Nil.
Author’s contributions
Conception and design: Shagufta Wahab, Divyashree; (II) Administrative support: Shagufta Wahab, Ibne Ahmad, Deoshree Akhouri; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: Shagufta Wahab, Divyashree; (V) Data analysis and interpretation: All authors; and (VI) Manuscript writing: All authors. All authors have read and agreed to the published version of the manuscript.
Acknowledgements
This article is a part of MD thesis which was supported by NMC, India.