
Abstract
Introduction:
Nonvenereal skin diseases are often confused with sexually transmitted diseases. It is responsible not only for the physician's diagnostic dilemma but also for significant patient concerns. Identifying the cause or aggravating factors can save the patient from distress. Therefore, this study was conducted to determine the clinical pattern and prevalence of nongenital diseases.
Methods:
All males attending the dermatology outpatient department in our hospital are included in the study after getting informed consent. Detailed history, including demographic data, chief complaints related to skin, any symptoms in genitalia, drug history, and history of sexual exposures, was recorded.
Results:
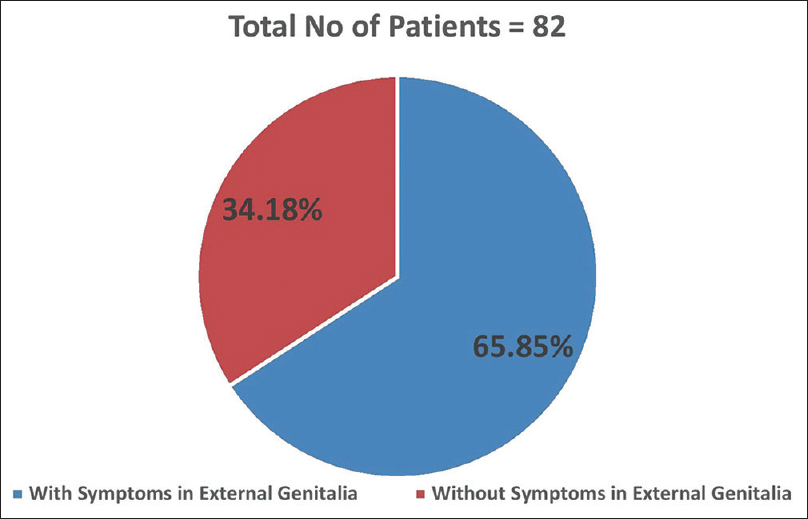
The prevalence of nonvenereal genital lesions during the period was 8.2% of patients attending the dermatology department. A total of 21% of nonvenereal genital dermatoses were studied in 82 patients. The most common ones encountered are pearly penile papules and tinea cruris, contributing 19.5% each. Vitiligo is the following most expected condition, involving 13.4% of patients. Among the total 82 patients with nonvenereal genital dermatoses, 65.8% had symptoms in external genitalia, and the rest of the 34.2% of patients did not have any complaints in genitalia.
Conclusion:
Among the 82 patients with nonvenereal dermatoses, 54 (65.85%) had symptoms in external genitalia. The study helped us understand the pattern and clinical characteristics of various nonvenereal genital dermatoses.
Keywords
Introduction
Nonvenereal skin diseases are often confused with sexually transmitted diseases (STDs). It is responsible for the physician's diagnostic dilemma and significant patient concerns.[1] This study should find patterns of nongenital dermatoses with genital lesions and associate them with different clinical parameters. Contrary to popular belief, not all genital lesions are sexual signs of contagious disease. These nonvenereal diseases are of considerable concern to patients because they cause psychological distress and guilt in those who believe they have STDs.[2]
Nongenital dermatoses often present a diagnostic dilemma for treating physicians who need to treat the condition and reduce its anxiety effectively. Therefore, it is imperative to have a thorough understanding of the various symptoms, their causes, and appropriate management options.[3] Identifying the cause or aggravating factors can save the patient from distress. In addition, nongenital dermatitis will not restrain the genitals. Other mucous membranes and skin may also be affected.[4] Therefore, it was necessary to conduct this study to determine the clinical pattern and prevalence of nongenital diseases.
Methods
We selected 1000 males for the study from the dermatology outpatient department (OPD) at our medical college hospital. Patients with venereal diseases, suspected malignancies, congenital abnormalities, and nonconsenting were excluded from the study. The demographic and epidemiological data were collected. Consent was obtained from the patients before they were included in the study. Detailed history, including demographic data, chief complaints related to skin, any symptoms in genitalia, drug history, and history of sexual exposure, is recorded. Careful examination of 62 external genitalia and dermatological examination of associated skin lesions was to be done. If required, KOH mount, Gram staining, and biopsy were done to confirm the diagnosis. Obtained data are recorded in preformed pro forma. The data were tabulated and analyzed.
Results
The study included 1000 male patients, with 82 nonvenereal dermatoses in genitalia. The prevalence of nonvenereal dermatoses in male genitalia is 8.2% among the male patients attending dermatology OPD [Figure 1].
Prevalence of non-venereal Dermatoses

The age ranges between 2 and 85 years, with a mean age of 30.68 years among the study population. Most patients with nonvenereal dermatoses belong to the 21–30 years age group (26 patients, 31.7%) [Table 1].
Distribution of nonvenereal dermatoses cases according to their age

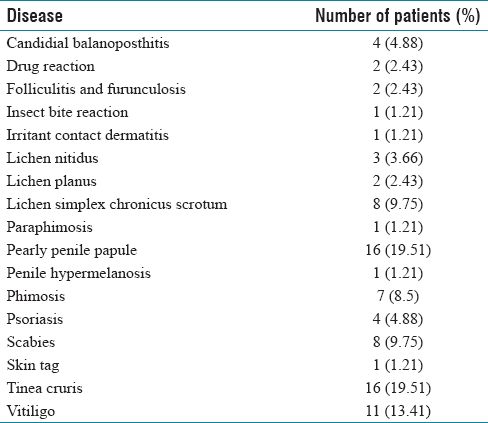
Among the 82 patients with nonvenereal dermatoses, 54 (65.85%) had symptoms in external genitalia. A total of 17 nonvenereal genital dermatoses were observed in 82 patients [Figure 2]. The entire study population belonged to different occupational backgrounds. Patients with nonvenereal dermatoses belonging to a particular occupation are compared with patients without nonvenereal dermatoses belonging to the same profession. It shows the maximum number of patients belonging to the student population followed by laborers [Figure 3]. The most common ones encountered are Pearly penile papules (19.51%) and tinea Cruris (19.51%). The prevalence of other genital dermatoses such as vitiligo has 13.41%, scabies (9.75%), lichen simplex chronicus (LSC) scrotum (9.75%), and phimosis (8.5%) [Table 2]. Other dermatoses included psoriasis, lichen nitidus, drug reaction, folliculitis and furunculosis, insect bite reaction, irritant contact dermatitis FDE, skin tag, and tinea cruris.
Distribution of nonvenereal dermatoses according to their type
Distribution of Non-veneral dermatoses according to symptoms in external genitalia
Association between dermatoses and occupation

Discussion
The nonvenereal genital disorder includes a wide array of diseases with varied etiology. Not many comprehensive studies exist concerning the prevalence and pattern of these diseases. In our study, the majority of nonvenereal dermatoses in male genitalia among male patients attending dermatology OPD is 8.2%, which is very high compared to Karthikeyan et al.'s[5] survey, where it was 14.1 per 10000 (0.14%). The age range of patients having nonvenereal dermatoses in male genitalia ranges from 4 years to 74 years, with a mean age of 30.87 years. In the study by Karthikeyan et al.,[5] the age range among the male population was 9–70 years, with a mean age of 33.7 years, similar to this study. Furthermore, a majority of the patients with nonvenereal dermatoses belong to 21- to 30-year age group (26 patients, 31.7%), which is consistent with the study done by Karthikeyan et al.[5]
Our study shows the maximum number of patients belong to the student population (28, 34.14%), followed by laborers (18, 21.95%). It is similar to the study by Karthikeyan et al.,[5] in which the most affected group belonged to laborers, followed by students and landlords. However, in our research, when the percentage of nonvenereal dermatoses among the total study population following the occupation was considered, lecturers were more affected 5 out of 10 (50%), followed by school teachers six out of 14 (42.86%).
Among the total 82 patients with nonvenereal dermatoses, 54 (65.85%) had symptoms in external genitalia, and the rest of the 28 (34.15%) patients were not having any complaints in genitalia. Other studies did not mention whether the patients came with primary genital complaints or not. In our study, some patients did not notice the lesions, and some hesitated to show genitalia even if they had seen them; this shows the importance of male genitalia examination as a significant population did not complain of lesions in genitalia (34.15%); yet, they had lesions in the genitalia. Among 82 patients with nonvenereal dermatoses studied in this study, 41 had scrotal involvement. The second most common part involved is the coronal margin and shaft of the penis, which involves 20 patients each, which is similar to the study done by Karthikeyan et al.[5]
This study studied various nonvenereal dermatoses, including 17 different dermatoses. In a survey by Karthikeyan et al.,[5] about 25 nonvenereal dermatoses were noted. The most common one mentioned in our study was pearly penile papules and T. cruris, which contributed to 19.25%. In a survey by Khoo and Cheong, 169 which included both venereal and nonvenereal diseases, 14.25% of the patients had pearly penile papules. In the study by Karthikeyan et al.,[5] only 4% of the study population had a pearly penile bump. The most common one they encountered was vitiligo (15.3%), and in our study, vitiligo was noted in 13.41%. In this study, 16 out of 82 patients had pearly penile papules. It contributes to 19.51% of the nonvenereal diseases in male genitalia. Age ranges from 6 to 34 years, with a mean age of 22.19. In the Sonnex and Dockerty[6] study, four among 200 men attending a genitourinary medicine have a 48% prevalence of pearly penile papules. Most men with bumps had only a few <1 mm lesions.
In this study, 16 out of 82 patients had tinea cruris contributing to 19.51% of the nonvenereal dermatoses in male genitalia. Age ranges from 7 to 47 years, with a mean age of 25.87. It commonly affects the laborers (7 out of 16) who work outdoors in humid conditions, followed by students (6 out of 16) who are also prone to excessive sweating. Their only complaint was itching in the groin, and all of them had involvement of the scrotum. In addition, 5 (31.25%) had involvement of the shaft of the penis and the scrotal involvement. A study by Pandey et al.[7] 98 showed penile participation in 19.5% of 261 patients. The same research attributes the association of increased incidence of tinea cruris in laborers with T-shaped cloth (Langota).[8]
Vitiligo is the most typical condition, involving 11 out of 82 patients and contributing to 13.41% of nonvenereal diseases of male genitalia. It follows the study done by Karthikeyan et al.,[5] which shows 15.3%. Another survey by Moses et al.[9] showed the incidence of male genital vitiligo is way <0.3%. Eight out of 82 patients had scabies contributing to 9.75% of the nonvenereal dermatoses involving male genitalia. A study by Karthikeyan et al.[5] showed a similar prevalence rate of 9%. In our study, the mean age of involvement is 10.12 years. It mainly affected the student population. All of them had involvement in the shaft of the penis, and three patients also had scrotum involvement. One patient had a secondary infection in a scabies lesion in other areas.
Lichen simplex chronicus (LSC) scrotum was noted in eight patients, and all complained of itching in the genitalia. The prevalence of 9.75% reported in our study is in contrast with the 2% in a survey done by Karthikeyan et al.[5] Two patients had LSC in the legs, which is consistent with the study done by Karthikeyan et al.[5] The mean age of involvement in our study was 50.75 years, affecting middle and old age people commonly. Furthermore, 7 of 82 patients had phimosis, contributing to 8.5% of the nonvenereal dermatoses in male genitalia. In the Karthikeyan et al.'s[5] study, only two patients have phimosis. In this study, the mean age of involvement is 38.85 years. There were studies on the prevalence of phimosis in school children, but studies in the adult population are lacking. The most typical cause of phimosis in our research is candidal balanoposthitis, being the cause for four patients.
Candidal balanoposthitis affects 4 out of 82 patients contributing to 4.88% of nonvenereal dermatoses. It is similar to the prevalence of 5% in a study by Karthikeyan et al.[5] All four patients have phimosis secondary to candidal balanoposthitis. In addition, 4.88% of nonvenereal dermatoses had psoriasis, which is more when compared to the 1% in the study done by Karthikeyan et al.[5] All four patients had scrotal involvement, and only one patient had a shaft of penis involvement. All four patients had psoriasis involvement in other areas.
In our study, 3.66% of nonvenereal dermatoses patients had Lichen Nitidus. A similar survey by Karthikeyan et al.[5] showed a prevalence of 1%. In all three patients in our study, the lesions were present in the shaft of the penis. Another survey by Lapins et al.,[10] which studied 43 cases of Lichen Nitidus, shows genitalia as one of the authoritative sites of involvement of lichen nitidus. In this study, two patients had lichen planus in male genitalia. In another study by Karthikeyan et al.,[5] they noted only one patient with lichen planus.
In this study, two patients had bullous fixed drug reactions, one for nonsteroidal anti-inflammatory drugs (Diclofenac sodium) and the other for cotrimoxazole. In the study by Karthikeyan et al.,[5] three patients had fixed drug reactions due to cotrimoxazole. Furthermore, in this study, one patient had folliculitis, and one had furunculosis in the scrotum. In another study, Khoo and Cheong[11] reported 1.7% of patients had folliculitis and furunculosis in male genitalia.
One patient had irritant contact dermatitis to the condom. A similar case was reported before as allergic contact dermatitis to additives in condoms. One patient (1.21%) had penile hypomelanosis involving the glans penis. In another study, Khoo and Cheong[11] reported the prevalence of penile hypomelanosis as 2.8%.
One patient had paraphimosis due to masturbation. One patient had a skin tag over the scrotum, probably reported for the first time in this study and one patient with an insect bite reaction over prepuce, causing prepuce swelling and phimosis. There were no reports of phimosis resulting from Insect bite reactions.
Conclusion
The prevalence of nonvenereal genital lesions during the period was 8.2% of patients attending the dermatology department. A total of 20.7% of nonvenereal genital dermatoses were studied in 82 patients. The most common ones encountered are pearly penile papules and tinea cruris, contributing 19.5% each. Vitiligo is the following most expected condition, involving 14.3% of patients. Among the total 82 patients with nonvenereal genital dermatoses, 65.8% had symptoms in external genitalia, and the rest of the 34.2% patients did not have any complaints in genitalia; this shows the importance of thorough examination of the patient, including male external genitalia even if the patient does not have any genital complaints. The study helped us understand the pattern and clinical characteristics of various nonvenereal genital dermatoses.
Footnotes
Acknowledgements
We thank all the participants who consented to the data collection.
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
Ethics Committee approval No: MMCH&RC/IEC/2015.
Funding
Nil.
Author's contribution
The study conception, design, data collection, analysis and interpretation of results and draft manuscript preparation was done by Dr Karthik Raja S and Dr. K S Premlal. All authors reviewed the results and approved the final version of the manuscript.