
Abstract
Background:
Cataracts are the most common cause of blindness in the world. This study aims to determine whether cataract surgery has an effect on the progression of macular thickness in nondiabetic and diabetic patients, specifically in the absence of pre-existing diabetic retinopathy (DR) changes.
Methods:
It is a prospective cohort study carried out between January 2022 and September 2022 at Shri Sathya Sai Medical College, which is a Tertiary Health-care Center situated at Chengalpattu district in Tamil Nadu, after obtaining ethical clearance from the Institutional Review Board. A total of 72 patients posted for cataract surgery were divided into two groups each group of 36 patients, Group 1 well-controlled diabetics without DR planned for cataract surgery and Group 2 nondiabetics. The patients underwent cataract surgery by small incision cataract surgery/phacoemulsification method based on the staging of cataract and also the surgeon’s choice and cataract surgery was done by the same surgeon and the patients were implanted with rigid/foldable intraocular lens.
Results:
Out of 72 patients analyzed in both the groups, 37 were male patients and 35 were female patients in the age group commonly 50–65 years. The mean age group in the diabetes group was 57.19 ± 9.18 and the normal group was 61.67 ± 7.73. The mean foveal thickness of the DR group was higher than that of the control group, but the difference was not statistically significant. At the end of the 3rd month, the mean foveal thickness returned to near-normal range.
Conclusion:
The thickness of the fovea is increased after cataract surgery in the 1st week postoperatively in both diabetic and nondiabetic groups and returns to near-normal preoperative value in both the groups at the end of 3 months postoperative period.
INTRODUCTION
Cataracts are the most common cause of blindness in the world. However, complications such as cystoid macular edema (CME) can occur even in uneventful surgeries regardless of whether the patients are diabetic or non-diabetic, thereby compromising the visual outcome of the patient. Now that advancements have been made in cataract surgery through extracapsular cataract surgery, small incision cataract surgery (SICS), and by phacoemulsification method, the chances of postoperative complications have been significantly reduced.[1] Patients with cataracts and diabetes who also have pre-existing diabetic retinopathy (DR) have an increased risk of DR development, especially maculopathy, following cataract surgery. This risk is heightened when DR was present before cataract surgery.[2,3] In addition, there is a possibility of postoperative cystoid macular edema in diabetes patients undergoing straightforward surgery, as was observed in earlier research.[4] Postoperative inflammation may be the cause of macular thickening after cataract surgery. This inflammation can lead to a breakdown of the blood-aqueous barrier and the blood-retinal barrier, which in turn promotes the production of inflammatory mediators such as prostaglandins and vascular endothelial growth factor, which ultimately results in macular edema.
It has been hypothesized that diabetic macular edema, also known as DME, is more likely to occur after cataract surgery in diabetic patients who already have preexisting DR with macular edema, as opposed to diabetic patients who do not have any preexisting DR. However, there are other studies that suggest that the development of macular edema is an independent entity for which preexisting DME does not need to be a prerequisite for the progression of maculopathy. Furthermore, some researchers believed that the progression of DR after cataract surgery is due to the natural course of the disease.[5] On the other hand, these experiments were conducted before the development of optical coherence tomography (OCT). OCT is a noninvasive diagnostic modality that assists in measuring retinal thickness qualitatively and quantitatively. As a result, it is a useful tool for treating clinical and subclinical cases, and, as a result, rapid treatment is possible.[6] Furthermore, OCT can provide detailed measurements of the macula in each of the nine zones, allowing for the case to be diagnosed even before fundus fluorescein angiography (FA) changes are made visible. Previous research seems to indicate that the state of DR before cataract surgery is the most relevant and reliable entity for determining the likelihood of advancement of DR.[6]
This study aims to determine whether cataract surgery has an effect on the progression of macular thickness, which can lead to macular edema, specifically in the absence of preexisting DR changes. We are comparing and evaluating the macular thickness in diabetics and nondiabetics before and after an uncomplicated cataract surgery at the early 1st postoperative week and at the end of 3 months in this study. This is being done to determine whether cataract surgery has an impact on the progression of macular edema.
METHODS
It is a prospective cohort study carried out between January 2022 and September 2022 at Shri Sathya Sai Medical College, which is a tertiary health-care center situated at Chengalpattu district in Tamil Nadu, after obtaining Ethical clearance from the Institutional Review Board. A total of 72 patients posted for cataract surgery were divided into two groups each group of 36 patients, Group 1 diabetic patients without DR changes with good glycaemic control planned for cataract surgery and Group 2 nondiabetics planned for cataract surgery. The patients underwent cataract surgery by SICS/phacoemulsification method based on the staging of cataract and also the surgeons choice and cataract surgery was done by the same surgeon and the patients were implanted with rigid PMMA intraocular lens (IOL) in SICS and foldable acrylic IOL in phacoemulsification method.
Inclusion criteria included patients between 40 and 80 years of both sexes. Cataracts of the moderate density of nuclear sclerosis 2–3, postsubcapsular cataracts in whom preoperatively macular thickness can be measured are included in both the groups. In (Group 1) well-controlled diabetic patients of any duration, either on oral hypoglycemics or insulin with HbA1c <7.5 with normal fundus detected preoperatively under indirect ophthalmoscopy and also under OCT were included in the study. We excluded patients with advanced immature cataracts and mature cataracts from the study and also cases where complications are anticipated such as posterior polar, pseudoexfoliation, and subluxated lens. Patients with preexisting ocular disease, namely uveitis, glaucoma, and patients with preexisting macular disorders were excluded from the study in both the groups.
OCT (3D Maestro; Topcon) was used to measure the preoperative and postoperative macular thickness in 1st week and at the end of 3 months compromising all nine zones, i.e. central 1mm, inner 4 quadrant and outer 4 quadrants and mean macular thickness is also measured.
Statistical analysis
Descriptive statistics were reported as mean (standard deviation) for continuous variables and frequencies (percentage) for categorical variables. Chi-square was used to find the association between categorical variables. Independent t-test was used to find the association between the continuous variables of the two groups. Repeated measure ANOVA to find the significance within the same group. Data were statistically evaluated with IBM SPSS Statistics for Windows, version 26.0., IBM Corp., Chicago, IL, USA.
RESULTS
Out of 72 patients analyzed in both the groups, 37 were male patients and 35 were female patients in the age group commonly 50–65 years. The mean age group in the diabetes group was 57.19 ± 9.18 and normal group was 61.67 ± 7.73.
The mean preoperative foveal thickness and macular thickness in each group are provided in Table 1 and Figure 1. The mean foveal thickness of the DR group was higher than that of the control group, but the difference was not statistically significant. At the end of the 3rd month, the mean foveal thickness returned to close to the normal range. However, in our observation, it was noted that 13 out of 36 patients in the diabetic group had significant thickening in 1st week and four patients continued to have increased foveal thickness higher than preoperative baseline value at the end of 3 months [Table 2]. In the normal group, 11 patients had a significant increase in foveal thickness in 1st week and subsequently returned to near baseline preoperative values at the end of 3 months. There was no significant association between the groups [Table 2]. The average thickness, I-Sup, I-Inf, I-Nasal; and, I-Temp, O-Sup, O-Inf, O-Nasal, and O-Temp of the DR group was higher than that of the control group and the difference was statistically significant. The percent change by group in the 1st week and 3rd month in comparison with the mean preoperative measurements are provided in Table 3.
Changes in macular thickness from baseline to postoperative week 1 and 3 months between the groups

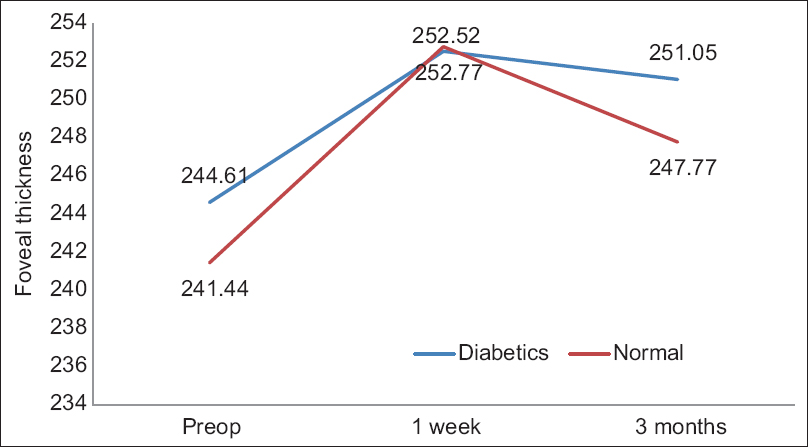
Changes in foveal thickness over time between the two groups
Distribution of increased significant macular thickness among the study participants

Percentage change by group at the 1st week and 3rd month in comparison with the mean preoperative measurements

DISCUSSION
This prospective comparative study was carried out to evaluate the effect of cataract surgery with IOL implantation on macular thickness in participants who were either diabetic or did not have diabetes during the postoperative phase. The central macular thickness (CMT) that was utilized for comparison among the study participants in our research was equivalent to the mean thickness of all points located in the central subfield of the early treatment diabetic retinopathy study (ETDRS) macular subfields that had a diameter of 1 mm. Comparisons were made between the two study groups with respective measurements using OCT to evaluate the CMT preoperatively, as well as at week 1 and 3 months postoperatively. This macular thickness increased postoperatively in all of the participants in both groups, and it did not return to its preoperative levels until the final follow-up, which was at 3 months. According to the findings of this study, the influence of cataract surgery on CMT did not significantly differ in diabetic people from healthy controls after uncomplicated cataract surgery. In other words, diabetics and nondiabetic patients showed comparable thickening of the central macular subfield after cataract surgery at week 1 and at 3 months, and the comparison between the two groups was not statistically significant.
People who have diabetes have a rate of macular edema development that ranges from 31%–81% following cataract surgery at different time intervals.[7] Even after a cataract operation that goes without a hitch, a patient’s retina may experience some very subtle changes, such as subclinical CME. After cataract surgery, these subclinical alterations in macular thickness are easily diagnosable using OCT and FA.[8] Macular edema may occur largely in patients with concomitant preexisting DR involving the center of the macula after cataract surgery in diabetic patients, as has been described by a few studies. On the other hand, some researchers have reported that preexisting DR is not necessary for postoperative macular edema to occur. This contradicts the findings of other researchers. However, these studies were carried out before OCT technology was readily available. In contrast to FA, OCT has a sensitivity of 96% and a specificity of 100% when it comes to identifying CME.[9] Not only can OCT detect macular thickening before any angiographic evidence of macular edema, but also it produces reproducible and consistent quantitative results, making it ideal for follow-up and assessment of the treatment response. OCT can detect macular thickening before any angiographic evidence of macular edema.[10,11] In light of these considerations, we decided to conduct our observational study using OCT as the investigative modality.
OCT provides a noninvasive, real-time, and three-dimensional imaging of the eye, which can be used to accurately measure the thickness of the macula and other retinal layers. This information can be used to monitor for any signs of macular edema, which is a common complication of cataract surgery. OCT can also be used to assess the health of the retina and other structures within the eye, helping to ensure that the patient has a successful outcome from their surgery. Using OCT, we can quickly detect any changes in the retina or macular thickness, allowing them to prompt intervention if necessary. OCT is an important tool for postoperative care of cataract surgery patients and should be utilized to help ensure the best possible outcome.[11]
There is a degree of disagreement between the observations of the many studies that have reported an increase in CMT or the development of macular edema in patients with diabetes who did not have DR after cataract surgery. In a case–control research that was carried out on approximately 4500 diabetics who did not have preoperative macular edema, the incidence of postoperative macular edema was found to be 4%, which was higher than that in the population that did not have diabetes (P < 0.001).[12] These authors also identified a higher risk for the development of macular edema in diabetic people who did not have DR, with a relative risk of 1.80 when compared to patients who did not have diabetes ( Relative risk (RR): 1.17).[13] Chu et al. found an increased macular thickness after uncomplicated cataract surgery in diabetics who did not have DR compared to preoperative values or to a control group of patients at all follow-up up to 12 months after cataract surgery.[12] This was found in diabetics who did not have DR. When compared to the eyes of healthy controls, the eyes of diabetic patients who did not have DR presented a higher CMT and a higher incidence of CME after cataract surgery. This explains why these patients’ visual acuity was unsatisfactory after cataract surgery.[12] On the other hand, a meta-analysis that was just recently carried out on diabetic patients who did not have DR found that there was no statistically significant rise in CMT values after cataract surgery 1, 3, or 6 months after cataract extraction.[14]
According to the findings of our research, the preoperative CMT as evaluated by OCT differs between the two groups. This is consistent with the findings of a study that was carried out by Chung et al., who similarly discovered differences in the macular thickness of diabetic patients and healthy participants.[15]
Our research is restricted with few limitations. To begin, despite being a rapid, non-invasive, non-contact, reproducible, and reliable in-vivo imaging technique, OCT is subject to the influence of a number of factors that might adversely affect its image quality.[16] It is possible that preoperative accurate scans cannot be obtained when there are media opacities present, such as cataract (particularly in the form of cortical and subcapsular forms).[16] We were able to circumvent this challenge by excluding patients who had thick media opacities. Therefore diabetic control and the absence of DR status play an important role in postoperative visual prognosis of patients undergoing uncomplicated cataract surgery, large-scale studies with longer follow-up periods will likely be required.
CONCLUSION
The thickness of the fovea is enhanced after cataract surgery both during the 1st week and 3 months after surgery in diabetic patients as well as healthy participants who do not have diabetes. The discrepancy was notably more pronounced among those suffering from diabetes than in those who were healthy. At the end of the 3rd month, the mean foveal thickness reverted back to near-normal levels. It has been hypothesized that proper management of diabetes is essential to forestall an increase in CMT and postoperative macular edema following cataract surgery that was uneventful. However, to formulate management algorithms that can be used as paradigms, long-term follow-up studies may be required.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
Institutional Ethical committee was obtained (IEC approval no:2022/728).
Funding
Nil.
Author’s contribution
All the authors have significant contributions to this study. MRK: Study design, case selection, manuscript writing and revision. DR: Data collection and statistical analysis. P.S.A: Monitoring of diabetic patients for glycemic control and draft checking. PR: Initial and final draft checking and referral of diabetic patients for retinopathy screening.