
Abstract
Objectives:
A hospital-based retrospective study was undertaken among the adult patients presenting to document the incidence of hypertensive urgency (HTN-U) and emergency while the secondary objectives included clinical presentations, disposition from emergency room, and inhospital mortality.
Materials and Methods:
All patients were evaluated by vital signs, clinical examination as well as relevant laboratory tests and radiological tests. Patients with target organ damage were grouped under the hypertensive emergency (HTN-E) group (n = 104) and patients without target organ damage were included under the HTN-U group (n = 52). The data were analyzed using GraphPad Prism (vs. 9.4.1) and MedCalc (vs. 20.118).
Results:
The incidence of HTN-E and HTN-U was 68.4% and 31.6%, respectively. The most common symptom observed in patients with HTN-E was breathlessness (53.8%), followed by chest pain (34.6%) and headache (27.9%). While, in HTN-U patients, most patients reported chest pain (43.8%), headache (39.6%), and epistaxis (22.9%). Majority of the patients in both the groups presented with signs of tachycardia, tachypnea, and hypoxia. The mortality in HTN-E and HTN-U patients was 15.4% and 2.1%, respectively. Among 104 patients with HTN-E, 53.8% each of the patients had acute heart failure and acute pulmonary edema. While, in HTN-U patients, acute pulmonary edema and acute coronary syndrome were observed in 2.1% each of the study subjects.
Conclusion:
Patients at high risk or end-organ damage should be immediately referred to the emergency department from the outpatient settings, as a rapid reduction in blood pressure is essential over minutes to hours, to prevent further organ damage.
INTRODUCTION
Hypertensive crises are defined as “clinical scenarios associated with severe elevations in systolic and diastolic blood pressure, usually above 180/120 mmHg.” Hypertensive crises are further classified as hypertensive emergencies and urgencies. Hypertensive emergency (HTN-E) is characterized by the presence of target organ damage unlike hypertensive urgency (HTN-U).[1] In accordance with estimates in India, at least one in four persons have HTN; however, only 12% of the population have their blood pressure under control.[2] Moreover, HTN is directly responsible for 57% of all stroke deaths and 24% of all coronary heart disease deaths in India.[3] The increase in the prevalence of hypertension cases in India can be attributed to rapid urbanization, unhealthy eating patterns, increase in smoking and alcohol consumption, etc. HTN is the most easily preventable problem, but the main hurdle in the management of HTN is its diagnosis, because it typically has no warning signs or symptoms. A small amount of people may experience symptoms such as dull headaches, vomiting, dizzy spells, and more frequent nosebleeds. These symptoms normally do not appear until blood pressure levels have reached a dangerously high or life-threatening level, necessitating a visit to emergency department (ED).
Patients with poorly controlled HTN need effective and rapid-acting medications administered intravenously to lower the elevated blood pressure safely, protect target organ function, ameliorate symptoms, reduce complications, and improve clinical outcomes. EDs serve as the point of entry into the health-care system for high-risk patient populations, including minority and low-income patients. Thus, ED engagement and early risk assessment/stratification is a feasible innovation to help close health disparity gaps in HTN. Hence, a research study in EDs of Indian demographics should be periodically carried out to put a check on HTN and its implications on target organ damage. This present study was carried out to study the incidence as well as the distinguishing nature of hypertensive emergencies and urgencies such as symptoms, causes, and clinical outcome in terms of overall inhospital mortality of the patients with HTN urgencies presented to ED of a tertiary care hospital in Western India. As the adult population in India is growing, there is a need to have sufficient knowledge about awareness, control, and management of HTN which could guide the development of policies to reduce the burden of HTN in India.
MATERIALS AND METHODS
A hospital-based retrospective study was undertaken among adult patients presenting to the ED of a tertiary care center in Western India over a period from March 2022 to August 2022.
Inclusion criteria
All consecutive patients aged ≥18 years presenting with hypertensive urgencies or related symptoms
Patients who were successfully resuscitated at the scene.
Exclusion criteria
Pregnant patients
Trauma patients
Patients/relatives not willing to participate in the study.
Study procedure
All patient-related information such as age, gender, symptoms and signs at presentation, addiction to smoking, comorbidities, and medical history were recorded on a case record sheet. All patients were evaluated by vital signs, clinical examination as well as relevant laboratory tests (cardiac enzyme test, complete blood count, and lipid profile test), radiological evaluation computed tomography (CT) scan of the head, or cranial magnetic resonance imaging in cases of neurological deficits. The occurrence of microalbuminuria (30–300 mg/dL) as indicated by the spot urine albumin-to-creatinine ratio confirmed renal impairment. To differentiate stroke episodes, CT scan results were examined, while retinal damage was confirmed by fundus examination with the help of ophthalmoscope. The presence of electrocardiographic left ventricular hypertrophy (LVH) was used to define hypertensive damage to the heart. With the help of M-mode and two-dimensional echocardiography, abnormal heart rhythms, wall motions, and tension were noted. Random blood sugar was also tested (low: <60 mg/dL; normal: 60–120 mg/dL; and high: >120 mg/dL). All patients were followed up to discharge or other outcomes whether in the ED or after being transferred to other wards. For the majority of patients, blood pressure was measured in the sitting position and in the supine position for unconscious patients.
Statistical analysis
For detailed analysis, 152 patients studied retrospectively were divided into two groups depending on target organ damage. Patients with target organ damage were grouped under the HTN-E group (n = 104) and patients without target organ damage were included under the HTN-U group (n = 48). The primary outcomes were the prevalence of HTN-U and emergency while the secondary outcomes included clinical presentations, disposition from ED, and inhospital mortality. The baseline patient characteristics are presented as frequencies for the categorical variables and as the means and standard deviations for continuous variables.
After appropriate data filtration, the data sheet was analyzed using GraphPad Prism (vs. 9.4.1) and MedCalc (vs. 20.118). Independent t-test was used as a test of significance to identify the mean difference while Chi-square test was performed to compare categorical data. P <0.05 was considered statistically significant. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval for the study was waived off as there was no intervention that was performed outside the scope and management laid down by the hospital. All necessary precautions outlined in the hospital guidelines were followed throughout the study to protect patient’s confidentiality. Informed consent was obtained from the patients regarding the publication.
RESULTS
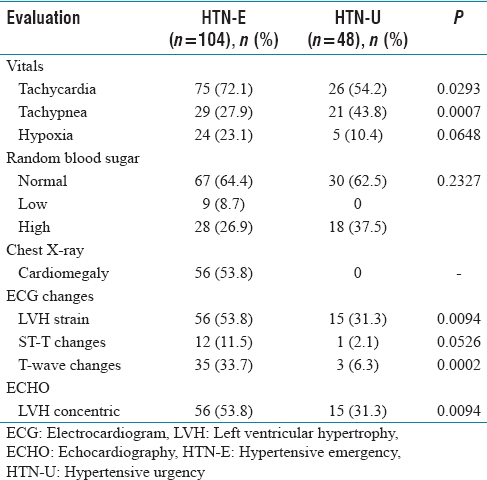
Among 152 study subjects, 93 (61.2%) were males and 59 (38.8%) were females. The incidence of HTN-E and urgency was 68.4% and 31.6%, respectively. Both the HTN groups had a higher incidence in males as compared to females [Table 1]. Majority of the patients with HTN-E were in the fourth decade of life (54.8%) followed by geriatrics (36.5%) and then in the age range of 18–39 years (8.7%), while majority of the patients in HTN-U were geriatrics (47.9%), followed by patients with age 40–59 years (31.3%) and 18–39 years (20.8%). The most common symptom observed in patients with HTN-E was breathlessness (53.8%), followed by chest pain (34.6%) and headache (27.9%). While, in HTN-U patients, most patients reported chest pain (43.8%), headache (39.6%), and epistaxis (22.9%). The most common comorbidity in both the HTN-E and urgency patients was diabetes mellitus (43.3% and 37.5%, respectively) [Table 1]. There was a significant difference in the incidence of tachycardia and tachypnea between the HTN-E and urgency patients, and the incidence was higher among the HTN-E patients (P < 0.05). The incidence of abnormal electrocardiogram (ECG) changes such as LVH strain (P = 0.0094) and T-wave changes (P = 0.0002) was higher among the HTN-E when compared to HTN-U patients [Table 2]. The mean systolic blood pressure, diastolic blood pressure, and mean arterial pressure were higher in HTN-E patients when compared to HTN-U patients [Table 3]. Among the HTN-E patients, majority (77.9%) were admitted to the intensive care unit (ICU). Among HTN-U patients, more than half (58.3%) of the patients were discharged from the emergency room and only 37.5% were admitted to ICU. The mortality rate was higher among HTN-E patients (15.4%) when compared to the HTN-U patients (2.1%) [Table 4]. Acute heart failure and pulmonary edema were commonly observed in HTN-E patients (53.8% each) while unstable angina (20.1%) was commonly observed in HTN-U patients [Table 5]. 39.4% and 89.6% in the patients with HTN-E and HTN-U, respectively, did not require oxygen support. 32.7% of patients with HTN-E required noninvasive oxygen support as compared to only 8.3% of patients with HTN-U, while 27.9% and 2.1% of the patients with HTN-E and HTN-U, respectively, needed invasive support [Table 6].
Baseline characteristics, risk factors, and clinical presentations

Clinical and radiological evaluation
Blood pressure measured at presentation

Disposition from emergency room and mortality in patients with hypertensive crises

Final patient diagnosis

External oxygen support required in patients with hypertensive crises

DISCUSSION
Hypertensive crisis is progressing in India and continues to have a negative impact on the health of the country’s population. This was a retrospective study carried out on 152 patients with hypertensive crises presenting to an ED of a tertiary care hospital. This study comprehends and adds to the existing literature regarding the underlying mechanisms of hypertensive crisis. The incidence of HTN-E and HTN-U was 68.5% and 31.5%, respectively, which is consistent with similar studies by Singh et al. and Shao et al.[1,4] However, the incidence of HTN-U is increasing due to an increase in awareness on HTN and its screening procedures. One of the nonmodifiable risk factors for HTN is age. However, the PURE study demonstrated that the incidence of HTN is even increasing in the younger age.[5] The incidence of HTN was substantially higher in patients with age >50 years when compared to the younger individuals which was very evident from our study as the study population aged more than 50 years represented 66.4% of the total subjects. For people younger than 45 years, the incidence of HTN was more frequent in men when compared to women. Whereas, for people older than 65 years, the incidence of HTN was more frequent in women than men. These observed gender differences in HTN can be attributed to both biological and behavioral factors such as sex hormones, chromosomal variations, and other biological sex differences. Moreover, it is not surprising that the mean age of our female patients was 55.9 years slightly higher than male patients (52.7 years) which may be attributed to the above-discussed factors although the difference in HTN-E and HTN-U in relation to gender was found to be insignificant (P = 0.2278). The overall mean age of all patients was 54.1 years. The incidence of HTN-E was higher in the fourth decade of life (54.8%) while the incidence of HTN-U was frequently noticed beyond the sixth decade of life (47.9%). Martin et al. also reported that the majority of the patients in HTN-E were in the age range of 60–80 years.[6] Out of 93 male subjects, 72.04% of males had HTN-E as compared to 62.7% (37/59) females, which was similarly reported in a study by Dinesh and Krishna (56.1% of males and 48.5% of females). This might be due to the fact that males are highly vulnerable to HTN-related target organ damage.[7] Vitale et al. also stated that females are less susceptible to HTN due to biological determinants.[8]
The interaction between cigarette smoking and blood pressure values has been intensively investigated, either as concerning a causal relationship between smoking habit and incidence of HTN or in terms of smoking-related impact on the prognosis for hypertensive patients. 44.1% of study population had a habit of smoking while 21.7% had a habit of alcohol consumption. There was no significant difference between the HTN-E and HTN-U patients with regards to smoking (p=0.5173) and alcohol consumption (p=0.5475). HTN is known as the “silent killer” as it is typically asymptomatic. The most common clinical symptom observed in HTN-E patients was breathlessness (53.8%), followed by Chest pain (34.6%), headache (27.9%) and epistaxis (23.1%). Twenty-five percent of the patients with HTN-E presented with neurological deficit while chest pain (43.8%), headache (39.6%), and epistaxis (22.9%) were the commonly reported symptoms in HTN-U patients. Dinesh and Krishna and Manjhvar et al. reported neurological deficit (43.9% and 47.22%) and dyspnea (36.3% and 37.5%), respectively, as the common clinical finding among the HTN-E patients while Manjhvar et al. reported headache (44.64%) and giddiness (42.86%) as the common presentations in HTN-U patients.[7,9] Similar to our observations, Dinesh and Krishna also reported headache (44.1%) and epistaxis (32.3%) in HTN-U patients. Comorbidity is a common and notable status concerning the increasing complexity of care associated with it.[7] Out of the 152 respondents, a significant proportion of respondents reported comorbidities such as HTN (63.2%), diabetes mellitus (41.4%), ischemic heart disease (24.3%), chronic kidney disease (17.8%), and chronic obstructive pulmonary disease (18.4%). The prevalence of these comorbidities was relatively higher in patients with HTN-E as compared to HTN-U although the difference was statistically insignificant [P > 0.05; Table 1].
The clinical presentation varied between the HTN-U and emergency patients, and it may be useful for stratifying hypertensive crisis into HTN-E and HTN-U during emergency care. Vital signs play a crucial role to prioritize the patients in the EDs, which guides the management and disposition of the patients. High-acuity patients are identified by cross-tabulating critical important vital signs with presenting complaints. There was a significantly higher number of patients with clinical signs such as tachycardia (P = 0.0293), tachypnea (P = 0.0007), and hypoxia (P = 0.0648) in HTN-E as compared to patients with HTN-U. There was a significant difference in systolic blood pressure (P = 0.0001), diastolic blood pressure (P = 0.0016), and mean arterial pressure (P = 0.0005) recorded at presentation between the patients of HTN-E and HTN-U [Table 3] which is in line with the study by Vinayak et al. but contrary to Manjhvar et al.[9,10] Furthermore, during echocardiography, 53.8% of the patients with HTN-E had LVH concentric as compared to 31.3% of patients with HTN-U (P = 0.0094). ECG changes such as T-wave changes (P = 0.0002), LVH strain (P = 0.0094), and ST-T changes (P = 0.0526) were dominant in patients with HTN-E as compared to HTN-U. Similar observations were reported by Dinesh and Krishna.[7] Among 104 patients with HTN-E, the most frequent final diagnoses were acute heart failure (53.8%) and pulmonary edema (53.8%) followed by acute kidney injury (22.1%), SAH (19.2%), and unstable angina (17.3%). Manjhvar et al. reported retinopathy (66%), cerebral infarction (19%), acute heart failure (18%), and intracerebral hemorrhage and acute coronary syndrome (16% each).[9] Martin et al. reported acute ischemic stroke (39%), left ventricular failure (25%), intracerebral hemorrhage (17%), and acute myocardial infarction (8%) in their patients.[6] Shao et al. reported HTN (37.4%), cerebral vascular accident (31.0%), and renal failure 25 (12.3%) as the top three most frequent final diagnoses. The overall inhospital mortality in patients with HTN-E was 15.4% while the mortality was relatively lower in patients with HTN-U (2.1%).[4] These findings are consistent with the studies by Shao et al. (26.8% and 3.1% for HTN-E and HTN-U, respectively), and it was higher than Dinesh and Krishna study (13.6% and 0% for HTN-E and HTN-U, respectively).[4,7]
Limitations
The present study was a single-center study of retrospective nature with a limited number of hypertensive patients presenting to ED. A multicenter study would be able to enroll a larger number of patients and would generate more significant data, in terms of clinical outcome, length of stay, and occurrence of major adverse cardiovascular events during the follow-up period.
CONCLUSION
The incidence of hypertensive urgencies in the ED was high at 31.6%. Hypertensive crisis is a serious medical condition associated with acute target organ damage with significant morbidity and mortality. The ED plays a vital role in the rapidly identifying, differentiating HTN-E from HTN-U and also the appropriate disposal. Patients at high risk or end-organ damage should be immediately referred to the ED from the outpatient settings, as a rapid reduction in blood pressure is essential over minutes to hours, to prevent further organ damage. A focused but detailed history of present illness should be conducted and signs and symptoms that may represent acute end-organ damage should be assessed. Spreading awareness on high blood pressure, its warning signs, controllable risk factors, and patient management as well as systematic screening campaigns of individuals should be targeted so that the patients are brought within the window period to the hospital.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
As the nature of the study was retrospective, ethical approval for the study was waived off as there was no intervention that was performed outside the scope and management laid down by the hospital. All necessary precautions outlined in the hospital guidelines were followed throughout the study to protect patient’s confidentiality. Also, Informed consent was obtained from the patients regarding the publication.
Funding
Nil.
Author’s contribution
All authors contributed to the study conception and design. Literature search was carried out by BG & VN. Data acquisition was done by BG while data analysis was done by BG & VN. First draft of the manuscript was framed by BG which was later modified as per the suggestions by all the authors. All authors read and approved the final manuscript.