
Abstract
Aimand Objectives:
The present study was undertaken to evaluate whether patients that are administered analgesics depending on their initial pain severity are more satisfied with their treatment than those who are given analgesics in accordance with the WHO pain ladder management protocol.
Materials and Methods:
First consecutive 100 patients (Group I) with abdominal pain were treated with WHO pain ladder management and for the next 100 patients (Group II), the pain management was done based on their intensity of pain. All patients were assessed for relief of pain every 15 min based on visual analog scale (VAS).
Results:
The visual analog pain score started decreasing after the administration of analgesics in both groups. The VAS was monitored once every 15 min for 60 min and in each measurement, the score was slightly lower in Group II in comparison to Group I (P > 0.05). At the end of 60 min, the mean score was <4 in both groups. Eighty-six percentage of the patients in Group II and 79% of the patients in Group I were satisfied with their pain relief. Although the satisfaction level of patients was higher in Group II, it was not found to be statistically significant (P = 0.282).
Conclusion:
The usage of analgesics for pain management can be decided based on the severity of the pain instead of following the pain ladder management proposed by WHO. This can prevent the unnecessary usage of analgesics such as paracetamol and certain side effects due to that.
INTRODUCTION
Abdominal pain is traditionally defined as pain of nontraumatic origin with a maximum duration of 5 days and is the frequent etiology for the arrival to the emergency department (ED), attributing for eight million (7%) among 119 million ED visits in 2006.[1,2] The patient will typically present with severe abdominal pain, accompanied with nausea and vomiting.[3] The poorly managed abdominal pain led to catastrophic events such as patient discontentment, poor outcomes of the acute incident, impede healing, and escalated risk of progressing to chronic pain.[4] Acute abdominal pain is mainly due to infection, inflammation, vascular occlusion, or obstruction and the underlying pathologies gamut from intra-abdominal to extra-abdominal, metabolic diseases.[3] In spite of the fact that abdominal pain is a common symptom, it is important to be treated seriously, as it may signal serious disease. Hence, the physician practicing emergency medicine should be proficient in assessing abdominal pain. Although diagnostic and therapeutic advances have made it easier to diagnose (computed tomography, ultrasonography, and laparoscopy), the misdiagnosis rate has not changed much.
The usage of pharmacological medications is the mainstay of acute pain management. In ED, the management of pain relies on choosing an appropriate agent based on the severity of pain, quick onset of action, easy to administer, safe, and efficacious. Drugs such as nonsteroidal anti-inflammatory drugs (NSAIDS) should be administered for mild-to-moderate pain and systemic opioids for moderate-to-severe pain.[5] NSAIDs, including aspirin, naproxen, indomethacin, ibuprofen, and ketorolac, are excellent analgesics and anti-inflammatory agents. As analgesics, NSAIDs bind to induced cyclooxygenase 2 receptors in the dorsal horn of the spinal cord. NSAIDs exert anti-inflammatory activity by inhibiting the release of inflammatory peptides generated through prostanoids and arachidonic acid at the injured site.[6] WHO analgesic ladder that comprises three steps was initially proposed in 1986 for the management of pain in cancer patients [Figure 1].[7] It manages patients based on the intensity of the pain, varying simple analgesics for mild pain to opioid analgesics for moderate and severe pain. In case of persistent pain, it is recommended to move one step ahead. If toxicity or any serious adverse effects are observed, then, the dosage of the medicine has to be decreased or come down one step. The ladder offers five easy guidelines for analgesic administration: by mouth, by clock, by ladder, by individual, and attention to detail.[8]

The World Health Organization analgesic ladder
The pitfalls of the ladder:
While 70%–90% of patients treated in accordance to the three-step ladder were relieved from the pain and in the rest, 10%–30% analgesia is not accomplished Early use of invasive interventions may lead to effective analgesia with minimum adverse effects and probably resulting in higher survival rate It is nonspecific, physicians reviewing the same patient could prescribe different treatment regimens, despite using the same treatment template.[9]
As of today, very few researchers had studied the adequacy of analgesia for patients presenting to the emergency room (ER) with acute pain abdomen and so the current study was undertaken to study the clinical profile of patients presenting with pain abdomen and to assess the adequacy of analgesia based on the patient satisfaction.
MATERIALS AND METHODS
This was a prospective study conducted on 200 patients reported to the ER with signs and symptoms of acute abdominal pain.
Patients with the following inclusion criteria were enrolled in the study:
Patients ≥18 years of age Ongoing abdominal pain not lasting for more than 2 days.
The following patients were excluded from the study:
Abdominal pain due to trauma, in need of immediate care Patients with any long-standing gastrointestinal pathology such as irritable bowel syndrome and inflammatory bowel disease and patients having gastritis Malignant patients Pregnant patients Those who were not willing for participation in the study.
The whole study period was divided into two halves of 6 months each. In the 1st 6 months, 100 consecutive patients who satisfied the inclusion criteria were treated with WHO pain ladder management for the relief of abdominal pain. Choice of analgesics and appropriate doses of analgesics were selected according to WHO pain ladder management. All patients were assessed for relief of pain every 15 min based on visual analog scale (VAS). As per WHO protocol, escalation of analgesics was done at the end of 15 min if pain intensity is persistent or if the difference of relief is <15 mm on VAS. Pain management was done with the help of nonopioids (paracetamol 1 g intravenous [IV] stat); then, as necessary, escalation was done to mild opioids (tramadol 50 Mg IV stat over 10 min with ondansetron 4 Mg IV); then, strong opioids such as fentanyl 0.5 μg/kg IV stat, until the patient was free of pain. Patients were monitored for adverse effects such as nausea, vomiting, rashes, drowsiness, and hemodynamic effects. Patient’s perception of the quality of care in pain management in the ED was evaluated by means of a patient questionnaire. Patients were monitored during the period of stay in ER to note their outcomes. Outcome parameters which were measured were pain intensity, time from arrival to analgesic administration, escalation of analgesics and frequency, relief of pain intensity, patient perception of quality of care in pain management, and duration of ED stay.
Over the next 6 months, the abdominal pain management in 100 consecutive patients presenting to ER was done based on their intensity of pain. Pain severity was determined by VAS and it was classified into mild (10–30 mm), moderate (31–60 mm), or severe (61–100 mm) kind of pain. In this group of patients, paracetamol was administered for mild pain. If mild pain was not relieved, rescue analgesic (injection fentanyl 0.5 mg/kg IV stat) was administered. As per intensity of pain in case of moderate pain, patients received tramadol 50 mg and IV fentanyl (0.5 μg/kg) was used as an analgesic if pain was not relieved. If pain still persisted, then repeat bolus dose of 50% of the initial dose of the drug administered was given. All patients were assessed for relief of pain every 15 min based on VAS. Patients were monitored for adverse effects such as nausea, vomiting, rashes, drowsiness, and hemodynamic effects. Patient’s perception of the quality of care in pain management in the ED was evaluated by means of a patient questionnaire. Analysis was done by correlating the severity of pain, diagnosis, and pain relief to intervention. In patients of both groups, relevant history including symptoms and signs at presentation, past medical history, drug history, and examination findings was noted. Informed consent for study participation was obtained from the patients and confidentiality was maintained throughout the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval for the present study was also sought from the Institutional Ethics Committee and Review Board (Reg. no. ECR/320/Inst/KA/2013; dated 9th Mar, 2017).
Statistical methods
The collected data were entered in MS Excel and analyzed using GraphPad Prism (Vs. 9.0) by Dotmatics, Boston, U.S.A. Mean and standard deviation were derived for all the parametric variables. Comparison of quantitative variables between the study groups was done using Student’s t-test while for comparing categorical data, Chi-square (χ2) test was performed. P ≤0.05 was considered statistically significant.
RESULTS
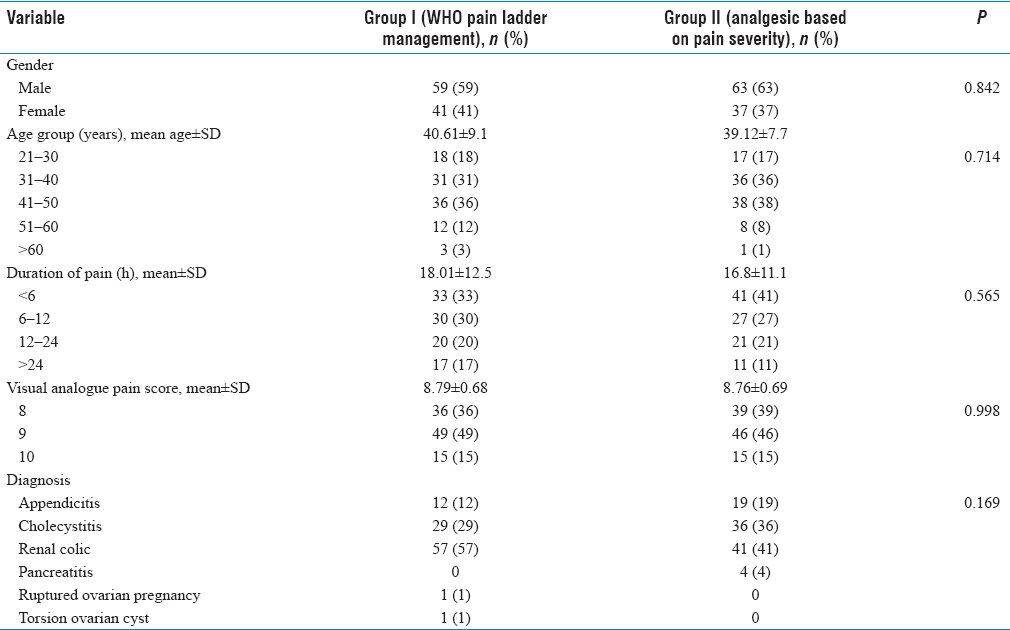
Minimum age of the subjects was 22 years and the maximum age was 63 years and the mean age among the Group I subjects was 40.6 ± 9.1 years while the mean age of the patients in Group II was 39.12 ± 7.7 years. There was no significant statistical difference between the two groups in terms of age distribution (P = 0.714). Male dominance was observed in the study. The male:female ratio was 1.4:1 and 1.7:1 in Group I and Group II, respectively. There was no significant difference between the two groups regarding the distribution of gender (P = 0.842). Majority of the patients in both groups had the complaint of acute pain for <12 h, and the mean duration of pain in Group I was 18.01 ± 12.5 h, and in Group II, it was 16.8 ± 11.1 h with no significant statistical difference (P = 0.565). Maximum number of patients in both groups had a score of 9, followed by 8 and 10. The average VAS score in Group I was 8.79 ± 0.68 and the average VAS score in Group II was 8.76 ± 0.69. There was no statistically significant difference between the two groups in terms of VAS score (P = 0.998). Majority of the study subjects in both groups had renal colic (49%), cholecystitis (32.5%), and appendicitis (15.5%). Patients in Group I, one (1%) patient had ruptured ovarian pregnancy and one patient (1%) had torsion ovarian cyst [Table 1].
Baseline characteristics of the subjects
The mean time for administering the first dose of analgesic was <10 min in both groups (9.4 ± 3.6 min and 8.1 ± 4.2 min in Group I and II, respectively). There was no significant statistical difference (P = 0.0815). The mean duration in the change of analgesic was 23.2 ± 4.9 min and 14.4 ± 8.1 min in Group I and Group II, respectively. The mean duration in the change of analgesic was earlier in Group II as compared to Group I and this difference was found to be statistically significant (P = 0.0218) [Table 2]. The most common initial analgesic used for pain severity was fentanyl 0.5 mg/kg, followed by tramadol (50 mg). Fifty-seven percentage of the patients in Group II received fentanyl and the rest 43% of the patients received tramadol [Table 3]. In both groups, fentanyl drug was used as an additional dose of analgesic and the majority of the patients in both groups had received two doses of fentanyl and only 14 patients in Group I and 17 patients in Group II did not require any additional dose of analgesic. The difference between the two groups in the requirement of an additional dose of analgesic did not show any statistical significance (P = 0.581) [Table 4]. Visual analog pain scores started decreasing after the administration of analgesics in both groups. The VAS was monitored once every 15 min for 60 min and in each measurement, the score was slightly lower in Group II when compared to Group I. However, the difference was not statistically significant (P > 0.05). At the end of 60 min, the mean score was <4 in both groups [Table 5]. Eighty-six percentage of the patients in Group II and 79% of the patients in Group I were satisfied with their pain relief. Although the satisfaction level of patients was higher in Group II, it was not found to be statistically significant (P = 0.282) [Table 6].
Time of administering the first dose of analgesic and its duration

Initial analgesics used among Group II patients (analgesic based on pain severity)

Additional doses of analgesics given among the study subjects

Mean visual analog pain score at different time intervals after the administration of analgesic between the two groups

Patients satisfaction levels for pain relief among the two groups

DISCUSSION
The daunting task encountered by the physicians in the ER is the management of acute abdominal pain. Appropriate analgesia depends on the assessment of the individual patient’s pain, thorough understanding of the underpinning etiologies of the abdomen pain and pharmacological action of the relevant pain relievers. There is a paucity of data in the timing of administration of analgesics and the type of pain relievers to be administered to treat acute abdominal pain. This ambiguity arouses from the concerns that analgesic administration before diagnosis may perplex the patient evaluation, especially the abdominal examination.[10] The evaluation process of abdominal pain often consumes time as it involves the physical assessment of the abdomen, laboratory evaluation, and imaging. Meta-analysis has established that if the diagnosis is awaited, opioid analgesics can be given to patients with acute abdominal pain to comfort the patient as it did not interfere with the results of the diagnosis.[11,12]
The present study was conducted among 200 patients presented to the ER with acute abdominal pain. The mean age of the study subjects was found to be 40 years and the majority of the patients were in the age group between 30 and 50 years. The present study had male: female ratio as 1.7:1, and the male dominance was similar to the study by Nega.[13] In our study, renal colic was the most common cause for acute abdominal pain, followed by cholecystitis and appendicitis which was incongruent with the results of the study by Hwang et al.[14] In the present study, the majority of the patients had severe-to-very severe abdominal pain with a VAS score of 8 or 9 similar to the findings of Hastings and Powers.[15]
McHale and LoVecchio in their review of prospective trials observed that, before the mid-1980s, withdrawing the opioid pain therapy in patients suffering from acute abdominal pain relied on the tenet and belief instead of the scientific findings.[16] However, now, there is a wide range of recommendations available on the use of pain relievers in the supportive care of patients. The superior among the guidelines is WHO’s analgesic ladder which forms the basis for others. This analgesic ladder encompasses three stages relating to different levels of pain relief and is progressed to base on the accomplishment of each stage. Initially, nonopioid is advocated, and then using relating to different levels of pain relief and progressed to base on the accomplishment of each stage. The first recommends a nonopioid, moving to a weak opioid (such as codeine, dihydrocodeine, or tramadol) along with an adjuvant and nonopioid analgesic for moderate pain. If the treatment is ineffective, for severe pain, WHO advocates the usage of a strong opioid (such as morphine, methadone, oxycodone, or hydromorphone) along with an adjuvant and nonopioid analgesic.[17] It is estimated that when used in combination in precise doses, the WHO ladder provides sufficient analgesic activity in 70% and 90% of the patients receiving supportive care.[18]
The two nonopioid analgesics used in the study are paracetamol and tramadol to reduce abdominal pain in ED. Tramodol is the drug synthetic drug which acts centrally by activating the μ-receptor. It can be prescribed in moderate and severe pain and we used it because the efficacy of this drug is the same as morphine and it also has very few side effects.[19] Paracetamol is used to relieve pain and to control the fever and it can be used safely in older and young children. In the present study, both drugs had analgesic action and the action was seen after 20 and 40 min of the administration. Tramadol and paracetamol provided a decrease of 20 mm on a 100 mm VAS scale at 20 and 40 min. This is consistent with previous research findings which observed that a reduction of 12–16 mm on 100 mm VAS scale is required to produce clinically significant improvement in patients with acute pain.[20-22]
Along with these concerns, insufficient management of pain in the patient might be due to communication issues, anxious about analgesic side effects, and overcrowding in ER.[23] The mentioned apprehensions and constraints result in significant delays in the relevant pain management as disclosed by Mills et al. who established that nearly half of patients in the ER were administered analgesics greater than an hour after admission.[24] Finally, the delay in treatment and inappropriate dosing of the analgesics affects patient care and satisfaction. In the case of postoperative analgesia, patient satisfaction was >90%, while with preoperative pain therapy, the satisfaction was only 40%–60%.[25]
In contrast to the portrayed convictions and fears, the proof-based research supports the usage of analgesic medication administration before the diagnosis in the management of acute abdominal pain. Several studies, including one Cochrane review published in 2007 and updated in 2011, have shown that administering analgesia for acute abdominal pain before the diagnosis is appropriate irrespective of the reason of the abdominal pain.[11,25] The Cochrane authors review stated that the administration of the narcotic analgesics did not either enhance the risk of false diagnosis or increased the risk of incorrect treatment decisions being implanted. They also suggested that patients with abdominal pain can be evaluated smoothly by the administration of analgesics. The present study also proves the same, where we observed that there was a notable amount of patient satisfaction with respect to pain relief in both groups (79% in Group I and 86% in Group II) and the administration of analgesics did not interfere in the clinical diagnosis of the patients with acute abdominal pain. In comparison to placebo, experimental findings indicate that the administration of analgesics to patients with acute abdominal pain does not considerably increase the chance of diagnostic error or faulty management decisions. Finally, the usage of analgesics in acute abdominal pain does not impact on the delayed diagnosis.
In the present study, the mean time interval between the time of arrival to our ED room and the administration of the first dose of the analgesic was 8–10 min after the initial assessment of the pain severity by VAS score. The VAS score was measured once every 15 min and the change in the analgesic was done every 15–20 min; however, the level of pain intensity at which pain relief should be administered is still debated in the research. Stork and Hofmann-Kiefer do not agree with the preclinical use of pain therapy if the score of numerical rating scale (NRS) ≤3.[23]
The most recent S3 guidelines and the authors of this article advocated the usage of nonopioid analgesic agents if the pain intensity of NRS ≤3 and nonopioids and opioids should be used conjunctively if the NRS >3.[26] The intensity of the pain has to be repeatedly assessed within the time span of 15–30 min relying on the analgesic’s onset of action and efficacy. The same principle was also followed in our study where we assessed the intensity of the pain scale once every 15 min and the scale, we used to be VAS score which is one of the most commonly used pain scales in India. Except for nausea and vomiting which had occurred in few patients after administering fentanyl, no other adverse events were reported in our patients which was in par with few of the previous studies. In the current research, no severe analgesics-related adverse events were observed in the study subjects administered with tramadol, paracetamol, and fentanyl. As all the previous studies conducted so far had only compared the different analgesics used for pain management and none of the studies had compared between WHO pain ladder management and pain management based on patient severity. Hence, this study is unique in its own sense and observed that patient’s satisfaction in pain relief is almost the same in both these groups.
CONCLUSION
The satisfactory level of pain relief was almost equal in both the groups which were treated based on WHO pain ladder management and based on the patient pain severity and so it can be concluded that the usage of analgesics for pain management can be decided based on the severity of the pain instead of following the pain ladder management proposed by WHO which can prevent the unnecessary usage of analgesics such as paracetamol and certain side effects following its administration.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Funding
Nil.
Author’s contribution
MC & NM: Concept and design of the study, carried out review of literature; NM & JSR: prepared first draft of manuscript, data collection and data analysis; MC & NM: critical review and language edits. All authors reviewed the final draft of the manuscript.