
Abstract
Pulmonary vein stenosis (PVS) post radiofrequency ablation for chronic atrial fibrillation poses a diagnostic challenge for the clinician. PVS presents with nonspecific symptoms, signs and radiographic features, and may be associated with significant pulmonary vascular involvement. Interestingly, others have described variation of the pulmonary artery wedge pressure between sites of the lung as a clue to pulmonary veno-occlusive disorders. We report, to the best of our knowledge, the first case that describes the regional loss of V waves while recording the mean pulmonary artery wedge pressure (mPawp) as well as the difference in pulmonary artery wedge pressure gradients as the main diagnostic clues for PVS.
INTRODUCTION
Radiofrequency ablation (RFA) procedures for chronic atrial fibrillation (AF) are being performed with increasing frequency. Pulmonary vein stenosis (PVS) following RFA for symptomatic AF occurs in 1-3% of the current series.[1,2] The clinical presentation of PVS varies widely. Symptoms, signs and radiographic findings of PVS are nonspecific and can be attributed incorrectly to a primary lung process (e.g., pneumonia, acute pulmonary embolism, interstitial lung disease or lung cancer).[3] For this reason, identification of clues to the diagnosis of PVS is important. We report a case of PVS with pulmonary hypertension (PH), where the presence and location of PVS was suggested by the observation of regional loss of the V waves during the measurement of the mPawp. To the best of our knowledge, this is the first descriptive case of this cardiopulmonary finding of PVS or occlusion.
CASE REPORT
A 65-year-old male was diagnosed with AF and underwent transcatheter RFA twice in 2007, followed by thoracoscopic pulmonary vein isolation in 2008. He was seen in the emergency room on several occasions with dyspnea on exertion, for which he was treated for a suspected pneumonia with antibiotics. He presented to our pulmonary clinic with persistent symptoms and intermittent dry cough. Transthoracic echocardiography (TTE) showed mild mitral regurgitation without signs of PH. Cardiac magnetic resonance imaging (MRI) showed an atretic and thin left inferior pulmonary vein of 2 mm in diameter, suggestive of severe PVS. He underwent right heart catheterization (RHC) for cardiopulmonary hemodynamic assessment, which showed the tracings depicted below (Fig. 1a–d).
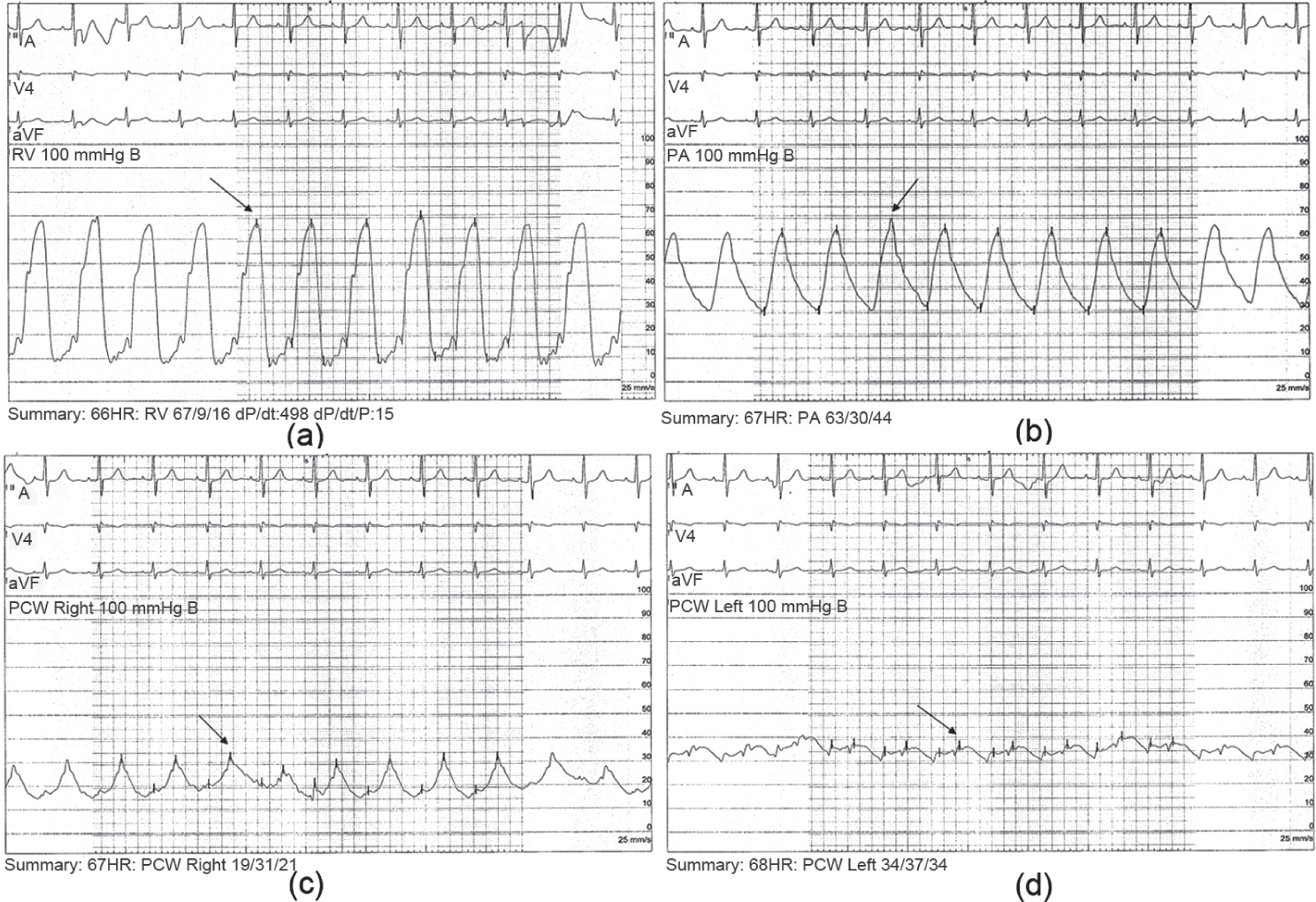
(a) Pulmonary hemodynamic tracing showing a mean right ventricular pressure (mRVP) of 42 mmHg. (b) Pulmonary hemodynamic tracings showing a mean pulmonary arterial pressure (mPAP) of 42 mmHg. (c) Pulmonary hemodynamic tracings showing a right mean pulmonary artery wedge pressure (mPawp) of 22 mmHg with the presence of tall V waves (arrow). (d) Pulmonary hemodynamic tracings showing a left mean pulmonary artery wedge pressure (mPawp) of 34 mmHg. Note the flattening of the V waves.
DISCUSSION
The development of PH with PVS has been rarely reported, and could represent complex and severe PVS with progressive pulmonary vasculopathic changes in the long term.[4–6] Our patient presented with persistent symptoms despite having involvement of only one vessel. Additionally, he had marked elevation in his left mPawp. He also demonstrated a loss of the V wave during the measurement of the left mPawp. The V wave represents the venous filling of the left atrium during ventricular systole when the mitral valve is closed.[7] Our patients tall peaked V waves noted when measuring the right mPawp may be explained by his mitral regurgitation. However, the tall V wave was not noted in the left mPawp tracing due to the lack of pressure transmission. To the best of our knowledge, this is the first description of this hemodynamic finding in the context of PVS. An additional clue suggesting PVS was the difference in the pressure gradients between the right and left mPawp (right mPawp of 22 mmHg versus left mPawp of 34 mmHg), emphasizing that equalization of pressures occurred between the right mPawp and the left atrium. Sharkey described the absence of V waves in acute pulmonary embolism. The A and V waves frequently disappear from the wedge tracing as abnormal pulmonary vasculature does not allow retrograde transmission of these pressure waves from the left atrium to the distal catheter lumen.[7]
CONCLUSION
Significant PH represents a rare complication of PVS, indicating the development of advanced pulmonary vascular disease as the stenosis progress to complete occlusion, particularly when more than two pulmonary veins are involved. Regional loss of V waves recorded during mPawp measurement represents a clue to the diagnosis and location of PVS. The difference in pressure gradients between right and left mPawp could suggest the diagnosis and location of PVS. However, we understand that given the absence of previous reports in the literature, these findings must be confirmed with reliable reproducibility in future PVS hemodynamic studies.