
Abstract
The members of the Pediatric Task Force of the Pulmonary Vascular Research Institute (PVRI) were aware of the need to develop a functional classification of pulmonary hypertension in children. The proposed classification follows the same pattern and uses the same criteria as the Dana Point pulmonary hypertension specific classification for adults. Modifications were necessary for children, since age, physical growth and maturation influences the way in which the functional effects of a disease are expressed. It is essential to encapsulate a child's clinical status, to make it possible to review progress with time as he/she grows up, as consistently and as objectively as possible. Particularly in younger children we sought to include objective indicators such as thriving, need for supplemental feeds and the record of school or nursery attendance. This helps monitor the clinical course of events and response to treatment over the years. It also facilitates the development of treatment algorithms for children. We present a consensus paper on a functional classification system for children with pulmonary hypertension, discussed at the Annual Meeting of the PVRI in Panama City, February 2011.
INTRODUCTION
The members of the Pediatric Task Force of the Pulmonary Vascular Research Institute (PVRI) were very aware of the need to develop a functional classification system for children with pulmonary hypertension and discussed the problem at the Annual Meeting of the PVRI held in Panama City in February 2011. We now present the consensus document resulting from our deliberations. We expect that it will be modified and improved in the years to come.
BACKGROUND
Clinical classifications of functional status are created primarily so that physicians can apply a common language to describe the functional impact of the same underlying disease on individual patients. Classifications should facilitate communication between physicians, all those involved in caring for the patient and the funding agencies providing financial support. The design of clinical trials is heavily dependant on an accepted, standardized means of describing the efficacy or otherwise of the treatment being evaluated. Studying the natural history of a disease, both treated and untreated, is dependant on a universally accepted means of describing functional status. Most importantly, a good classification should encapsulate the clinical status of a patient and so make it possible to review the patient's progress with time and their response to treatment.
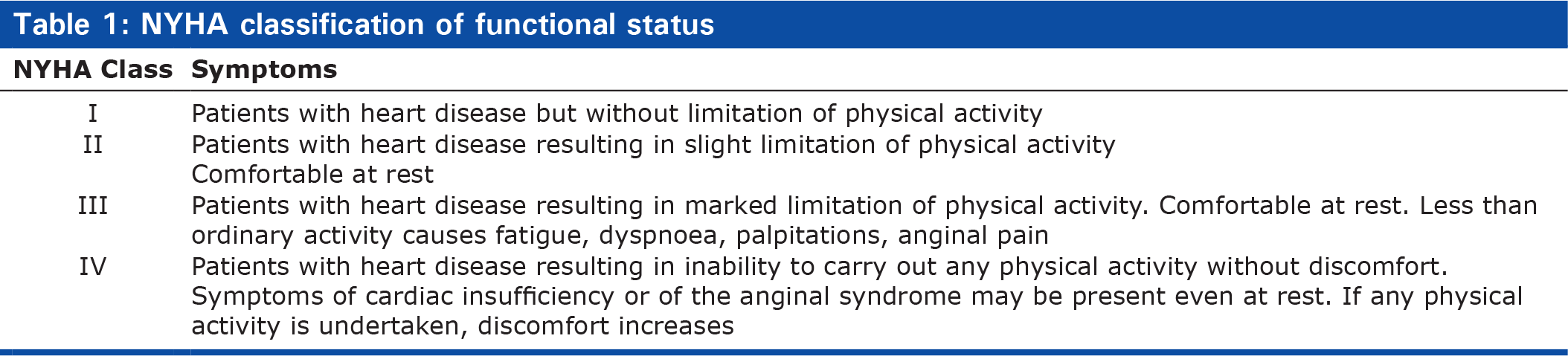
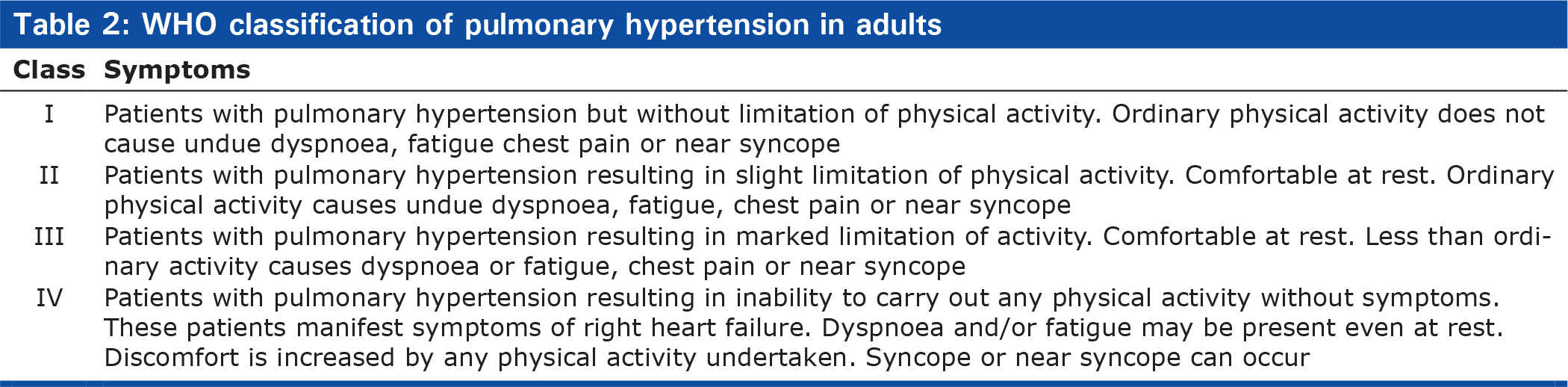
Classifications of functional status are familiar to cardiologists caring for adult patients. The New York Heart Association (NYHA), the classification most widely used by adult cardiologists since 1964 describes the functional impact of heart failure and places patients with a similar degree of limitation and similar symptoms into one of four functional classes, Class IV being the most severely disabled (Table 1).[1] The Functional Classification of Pulmonary Hypertension in adults is based on the NYHA classification (Table 2) and was published in 1998 as a consensus document of the WHO Symposium held in Evian in that year.[2]
NYHA classification of functional status
WHO classification of pulmonary hypertension in adults
Maintaining the best possible quality of life is crucial in any chronic disease. In adults, The Minnesota Living with Heart Failure (MLHF) questionnaire has been widely used in both hospital and primary care since it was designed in 1984, and has good reliability and validity.[3–5] This questionnaire can be useful in assessing patients with pulmonary hypertension,[6,7] as is the Short Form Health Survey 36 (SF-36).[8,9] The MLHF has been considered a significant predictor of outcome.[10] More recently, a disease specific questionnaire, the Cambridge Pulmonary Hypertension Outcome Review Utility Index (CAMPHOR) has been developed, primarily for cost-utility analysis but can also be useful in clinical studies.[11,12]
There is no disease specific classification to assess functional status in children with pulmonary hypertension. Nor is there a generally accepted functional classification for children with heart disease. Measures of generic health status have been developed for children, principally the Children and Youth Version of the International Classification of Functioning, Disability and Health published in 2007.[13,14] This classification assesses body structure and function, level of activity and social participation. It was designed primarily to assess children with neuromotor disabilities. Disease specific functional classifications have been developed for use in children with other conditions such as cystic fibrosis, rheumatoid arthritis and juvenile idiopathic arthritis.[15–18]
Quality of life is particularly difficult to assess in children. A Short Form Health Survey has been designed for children, SF-10[19] and can be used in children with pulmonary hypertension, but it is not disease specific. Nor does it help assess children less than 5 five years of age.
DESIGNING THE PROPOSED FUNCTIONAL CLASSIFICATION OF PULMONARY HYPERTENSION IN CHILDREN
The proposed Functional Classification of Pulmonary Hypertension in Children is based on the Evian pulmonary hypertension specific classification used in adults. It is not designed to assess quality of life and neither parent nor child makes a personal, direct contribution to the assessment. Particularly in children however, assessing function and activity does inform the physician about the quality of life.
Designing a functional classification is particularly difficult in children because the age, physical growth and maturation achieved influences the way in which the functional effects of a disease are expressed. It is essential therefore to be able to encapsulate a child's clinical status as he/she grows up in a consistent manner which makes it possible to monitor the clinical course of events over the years. In young children it is particularly challenging to distinguish whether any apparent deficiency in expectation can be attributed to the disease or is merely a normal variant in a developmental milestone. This is especially the case if pulmonary hypertension is complicated by syndromic or chromosomal abnormalities that affect motor and sensory function. Since any parent is naturally loathe to acknowledge that their child is really ill, any clinical classification needs to be as objective as possible.
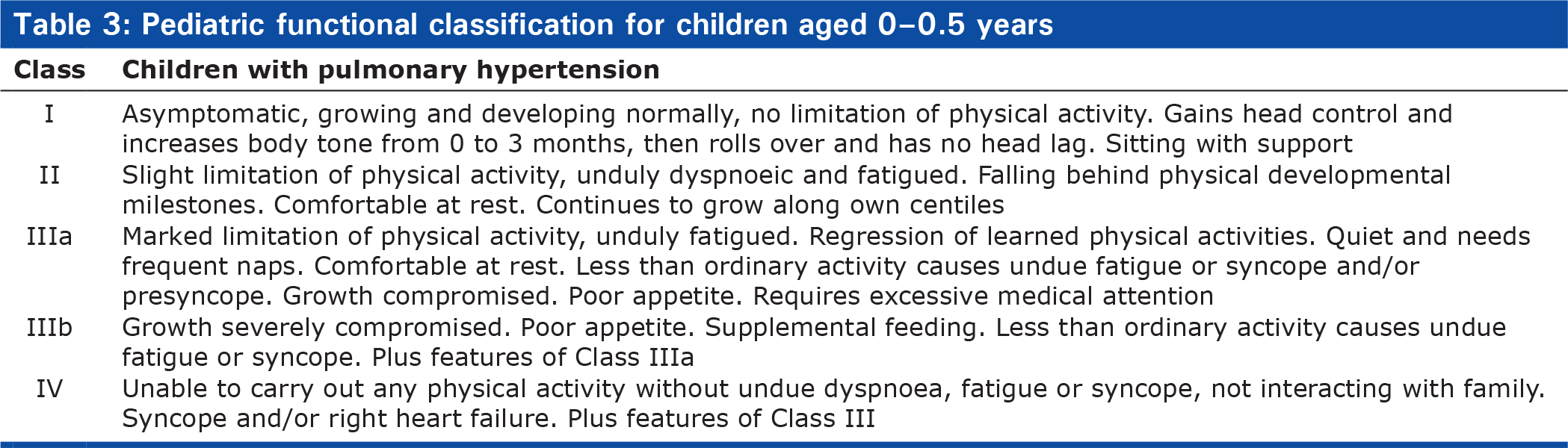
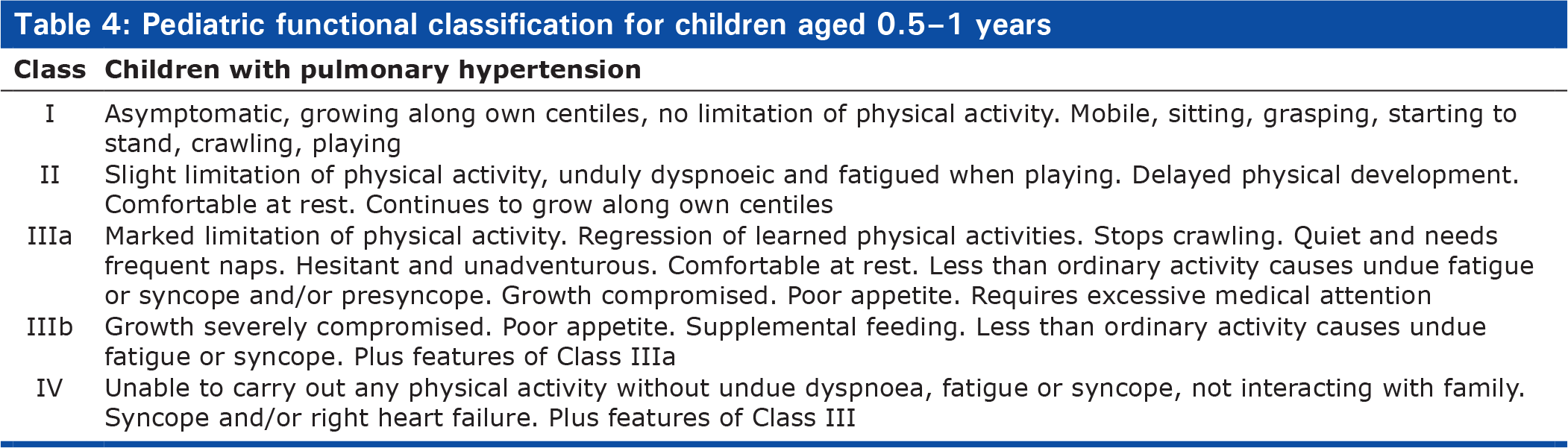
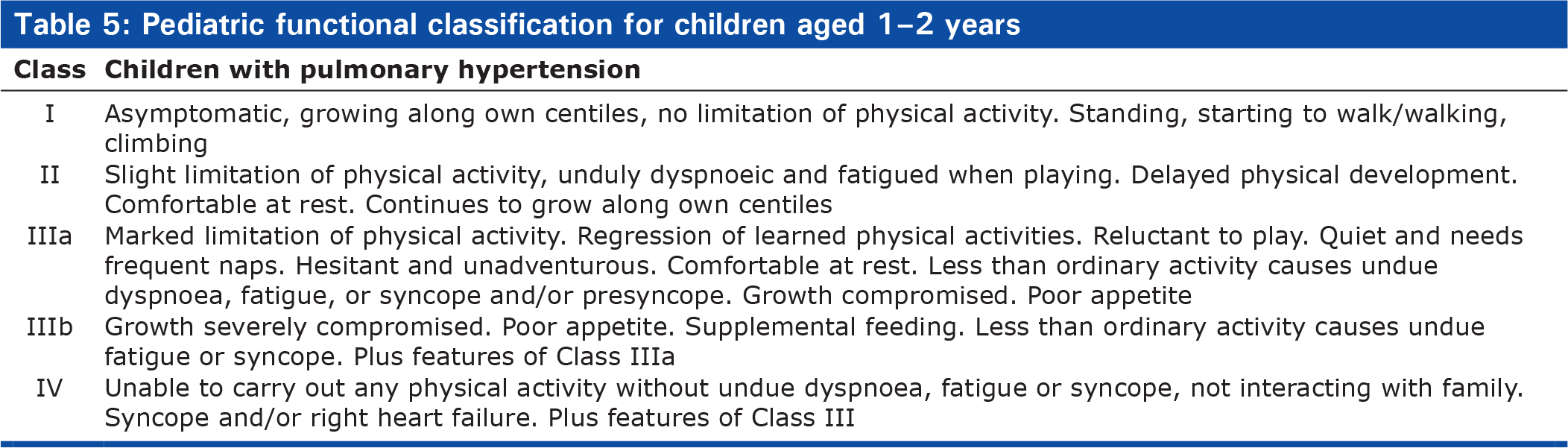
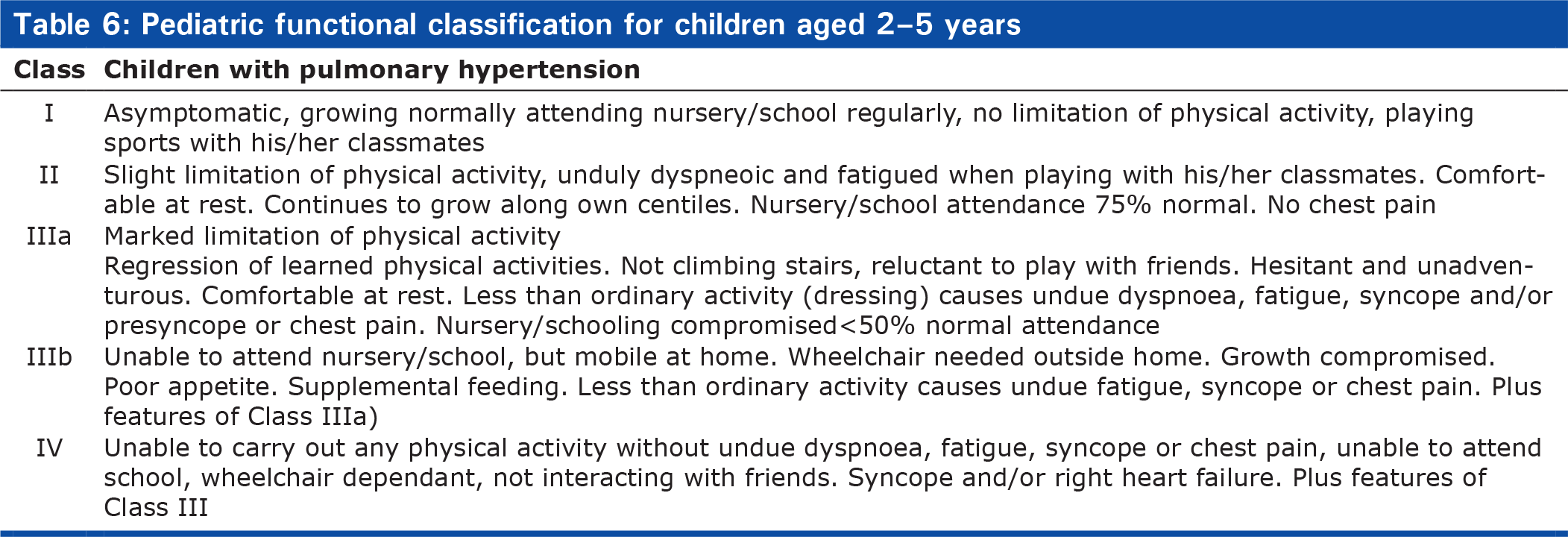
The proposed Functional Classification of Pulmonary Hypertension in Children follows the same pattern as the adult classification (Tables 3–7). There are four classes of disease severity, Class IV being the most severe. Class III has been subdivided into a) and b). We have tried to ensure that the classification will give a comprehensive summary of the child's clinical condition, while keeping it practical and easy to use. We decided to define functional class in five different age groups (Table 3). Three of the groups deal with children less than two years of age when the most rapid physical development and maturation occurs. Between the ages of two and five years it becomes easier to communicate with the child, while by six years the child is able to describe what they are able to do and how they feel. Children become increasingly articulate with age unless neurodevelopmental problems complicate the assessment. The adult classification is appropriate for those aged 16 years and over. Obviously, the patient is placed in the functional class which best summarises their clinical status and not all the descriptors of a functional class need to be fulfilled in order to place the patient in a particular class.
Pediatric functional classification for children aged 0–0.5 years
Pediatric functional classification for children aged 0.5–1 years
Pediatric functional classification for children aged 1–2 years
Pediatric functional classification for children aged 2–5 years
Pediatric functional classification for children aged 5–16 years
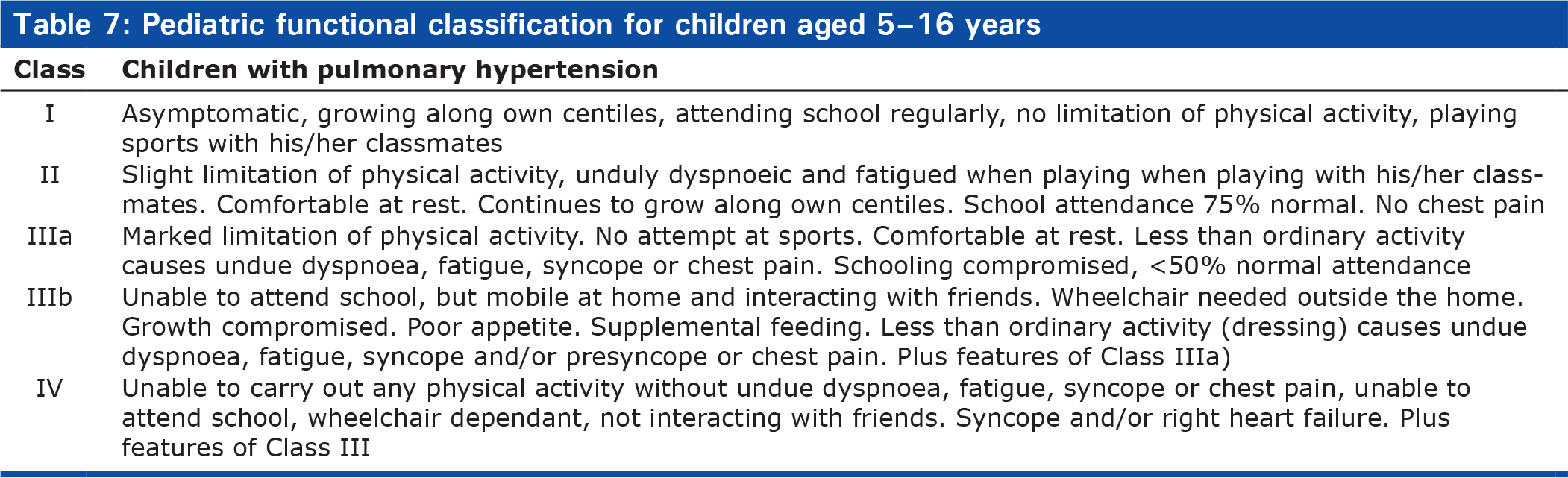
Bearing in mind that young children cannot tell one how they feel, we sought to include objective indicators such as whether or not the child is thriving, the need for supplemental feeds and the record of school or nursery attendance. The threshold for supplemental feeding can vary with age and be influenced by comorbidities but the need for supplemental feeding is usually an indication of disease severity. Parents are often reluctant to acknowledge the extent to which their child's schooling is compromised by illness, realising that absence from school reflects how sick their child really is. The days of school missed due to illness provides a measurable yardstick of illness severity. Therefore the classification includes guidelines suggesting an attendance of 75 or 50% or less to encourage them to give a realistic answer.
DESCRIPTORS OF FUNCTIONAL CLASS
Functional Class I
This is defined, at all ages, as children with pulmonary hypertension who are asymptomatic, growing and developing normally and have no limitation of physical activity. Table 8 outlines the most important features seen in normal children in the five age groups used in this classification and which we expect to find in children categorised as functional Class I. The emphasis on motor development in the first two years of life gradually shifts to the child's ability to interact with his/her peers, participate in sporting activities and go to nursery and then school.
What to expect of children in Functional Class I

Functional Class II
At all ages children with pulmonary hypertension are categorised as Functional Class II when they have only a slight limitation of physical activity due to fatigue and or dyspnoea but are comfortable at rest. Dyspnoea can interrupt feeding in young children. At this stage of their disease most children do not experience syncope or presyncope but some children can do so while still having a good exercise tolerance. During the first six months of life they fall behind their developmental milestones but continue to grow along their own centiles. Infants and young children are readily fatigued and dyspnoeic when playing. Beyond two years of age, it is important to assess attendance at school or nursery, which should be at least 75% that of healthy children.
Functional Class IIIa
Functional Class IIIa is characterised by marked limitation of physical activity. In addition to failing to achieve their developmental milestones, children between the ages of six months and two years may show regression of newly learnt activities. Inactivity is noticeable, the child being quiet and taking frequent naps. Less than ordinary activity such as dressing is tiring and can cause dyspnoea. Children frequently experience syncope and/or presyncope. Older children can become withdrawn and less confident, choosing to spend time with their families rather than their friends. Growth is compromised and appetite is poor. Nursery/school attendance is less than 50% of normal. The parents frequently say that the child has required excessive medical attention.
Functional Class IIIb
In addition to the features characteristic of Class IIIa, children in Class IIIb often require supplemental feeding by nasogastric tube or gastrostomy. Older children can no longer go to school and although mobile at home they need a wheelchair when venturing out of doors.
Functional Class IV
Children in Class IV are severely compromised and unable to carry out any physical activity without fatigue and/or dyspneoa. They are frequently syncopal, may complain of chest pain and often become quiet and withdrawn. Signs of right heart failure are frequently present, particularly in teenagers.
LIMITATIONS OF THE PROPOSED FUNCTIONAL CLASSIFICATION FOR CHILDREN
The growth and development of healthy children varies considerably and children with pulmonary hypertension will be subject to the same innate variability, increasing the difficulty facing the physician trying to assess the functional impact of disease. In addition, many children with pulmonary hypertension have multisystem disorders that may impact heavily on functional capacity independently of their pulmonary vascular disease. We have tried to ensure that the features characteristic of each functional class are objective but the opinion of the parents can influence judgement, particularly in a first child of young parents without extended family support who maybe uncertain about how their child differs from the normal. Some children are more stoical than others. Some physicians will recommend supplemental feeding more readily than others. Comorbidity further complicates assessment, primarily in children with neurodevelopmental handicap who may be syndromal. Despite all these and other caveats the Pediatric Task Force of the Pulmonary Vascular Research Institute believes that the proposed classification will facilitate the management of children with pulmonary hypertension.
CONCLUSIONS
The proposed Functional Classification of Pulmonary Hypertension in Children follows the same pattern and uses the same criteria as the adult classification, modified appropriately for children of all ages. The pediatric classification should therefore be understood readily by adult physicians during transition from pediatric to adult medical services, by all those caring for children with pulmonary hypertension and by those carrying out clinical research and designing clinical trials. It should facilitate the development of treatment algorithms for children, as has the adult classification in older patients with pulmonary hypertension.[20] This is a consensus document and we hope and expect that it will be improved upon with experience.