
Abstract

PULMONARY ARTERIAL HYPERTENSION DIAGNOSTIC ALGORITHM
Pulmonary hypertension (PH) is defined as a mean pulmonary artery pressure (mPAP) ≥25 mmHg, irrespective of etiology. In contrast to PH, the definition of pulmonary arterial hypertension (PAH) requires the exclusion of elevated pulmonary venous pressure, an established cause of PH, as reflected by a normal wedge pressure or left ventricular end-diastolic pressure (LVEDP) (≤15 mmHg). If PH is suspected in a patient, suitable screening tests are conducted to confirm the presence of PH and delineate the etiology to appropriately tailor an optimal therapeutic regimen. The diagnostic algorithm [Figure 1] reflects an integration of assessment pathways that help differentiate patients with WHO groups II – IV of pulmonary hypertension from WHO group I PAH as well as the subgroups of PAH. Caution is advised to apply the algorithm to any individual patient as the evaluation process of any patient with suspected PH requires a variety of investigations intended to confirm PH and the specific PAH subtype and, once confirmed, evaluate the functional and hemodynamic impairments of those patients. Right heart catheterization is universally considered to be an indispensable part of the diagnostic assessment.
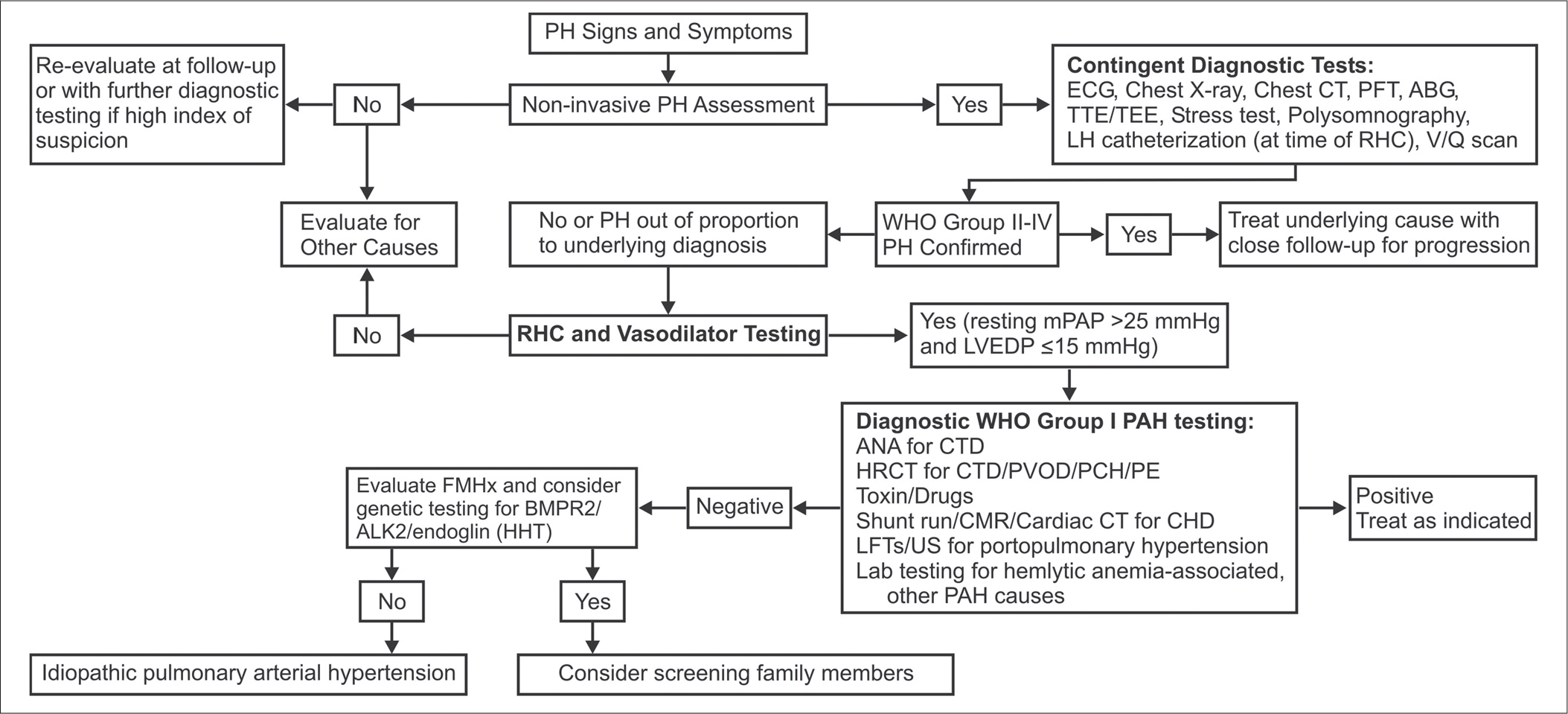
PAH diagnostic algorithm. (ABG - Arterial blood gas; ALK-1 - Activin-receptor-like kinase; ANA - Anti-nuclear antibodies; BMPR2 - Bone morphogenetic protein receptor 2; CHD - Congenital heart disease; CMR - Cardiac magnetic resonance; CT - Computed tomography; CTD - Connective tissue disease; ECG - Electrocardiogram; FMHx - Family medical history; HHT - Hereditary hemorrhagic telangiectasia; HRCT - High-resolution computed tomography; LFTs - Liver function tests; LH - Left heart; PAP - Pulmonary arterial pressure; LVEDP - Left ventricular end-diastolic pressure; PAH - Pulmonary arterial hypertension; IPAH - Idiopathic pulmonary arterial hypertension; PCH - Pulmonary capillary hemangiomatosis; PE - Pulmonary thromboembolic disease; PFT - Pulmonary function test; PH - Pulmonary hypertension; PVOD - Pulmonary veno- occlusive disease; RHC - Right heart catheterization; TEE - Transesophageal echocardiography; TTE - Transthoracic echocardiography; US - Ultrasonography; V/Q - Ventilation/perfusion lung scan; WHO - World Health Organization)
PAH RX ALGORITHM
The treatment algorithm is based on a consensus of the PH community based on the majority of randomized controlled clinical trials (RCTs) for PAH. The grading system is based on the recently published consensus for these drug trials.[1] Additionally, most trials were conducted in idiopathic or heritable PAH and PAH associated with scleroderma or anorexigen use; hence, the therapeutic effect on other PAH subpopulations may not be equal. Although there are no RCTs to substantiate the use of the following therapies, oral anticoagulation, diuretics in cases of fluid retention and supplemental oxygen in cases of hypoxemia (oxygen saturation <92%) are still considered the first line of treatment in patients with PAH. Acute vasoreactivity testing should be performed in all patients with PAH. Vasoreactivity is defined as reduction of mPAP ≥10 mmHg to reach an mPAP ≤40 mmHg with a normalized or increased cardiac output with acute pulmonary vasodilator challenge (either inhaled nitric oxide, adenosine or intravenous epoprostenol). Vasoreactive patients should be treated with high-dose calcium channel blockers with maintenance of response, defined as WHO functional class I or II with near-normal hemodynamic status, being confirmed by repeat right heart catheterization and clinical assessment after 3–6 months of treatment. Non-responders to acute vasoreactivity testing are defined both hemodynamically as well as by functional class II–IV, and should be considered candidates for other treatments as shown in Figure 2. The choice of the agent is dependent on a variety of factors, including route of administration, side-effect profile, patient preference and the physician's experience and clinical judgment. Continuous IV epoprostenol is the first-line therapy for IPAH and HPAH patients in WHO functional class IV because of its demonstrated survival benefit. Combination therapy should be considered for patients who fail monotherapy.
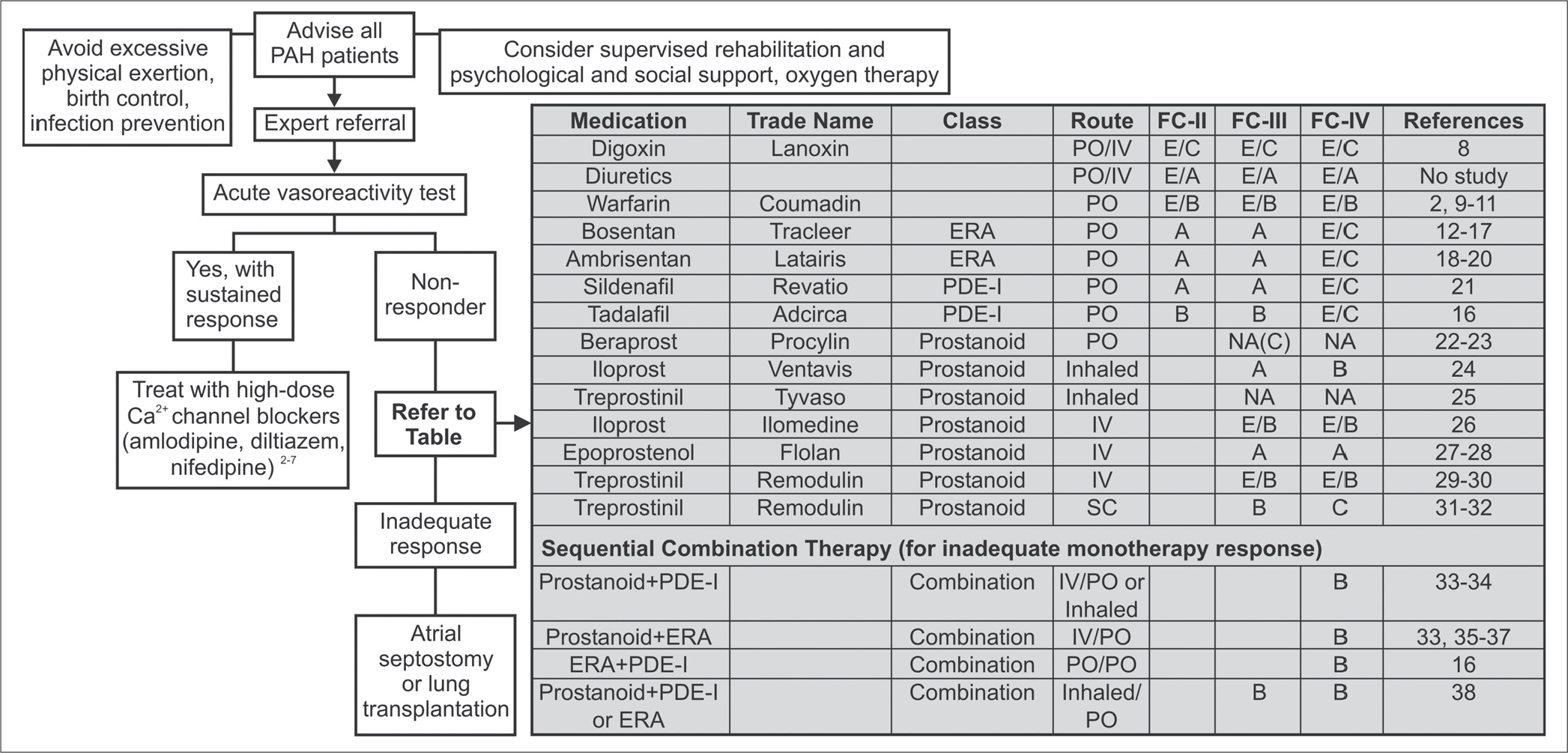
PAH treatment algorithm. (PAH - Pulmonary arterial hypertension; FC - Functional class; ERA - Endothelin receptor antagonist; PDE-I - Phosphodiesterase type 5 inhibitor; IV - Intravenous; PO - Oral; SC - Subcutaneous; NA - Not approved; WHO - World Health Organization; PAP - Pulmonary arterial pressure; RCT - Randomized controlled trial. Strength of recommendation: A - Strong recommendation; B - Moderate recommendation; C - Weak recommendation; D - Negative recommendation; E/A - Strong recommendation on the basis of expert opinion only; E/B - Moderate recommendation on the basis of expert opinion only; E/C - Weak recommendation on the basis of expert opinion only; E/D - Negative recommendation on the basis of expert opinion only)