
Abstract
This paper reviews a case of metastatic 1p/19q codeleted oligodendrioglioma causing diffuse osteosclerosis and pain. Primary central nervous system (CNS) tumors rarely metastasize outside the CNS, and metastatic oligodendroglioma is rarer still. The patient in this study had relief of pain after being treated with temozolomide. We discuss this rare presentation and potential treatment options, and review the literature in regards to metastatic oligodendrogliomas.
Introduction
Primary brain tumors are very unlikely to metastasize outside of the central nervous system (CNS). Recent advances in patient care have led to significantly prolonged survival in brain tumor patients. Consequently, metastatic lesions from primary brain tumors have been more often described.1–4 In 1969 a published report of 8000 primary CNS tumors reported 35 (0.4%) extracranial metastasis with GBM being the most common to metastasize. 5 Another review of the literature reported 21 cases of metastatic glioblastoma (GBM) from 1928-1967, and 107 reports of metastatic GBM from 1968-2006. 6 The increase in reported primary brain tumor extracranial metastasis may be due to a number of factors including: longer survival, better diagnostic technologies, and more aggressive surgical and medical treatments. Rarer still are metastatic oligodendrogliomas.
Bailey and Cushing originally postulated that gliomas never metastasize outside the nervous system as treatment and diagnostic paradigms of the times were limited. Over the years several case series have been described in the literature. In 1927, Liwnicz and Rubinstein reported 116 cases of metastasis from primary brain tumors. In addition, Pasquier
Oligodendroglioma (ODG) is a neuroepithelial origin brain tumor, representing 5% of intracranial gliomas. 8 Anaplastic oligodendroglioma has a median age of diagnosis of 49-years and an incidence rate of 0.17/100,000 persons. 9 Although local recurrence is common among oligodendrogliomas, extracranial metastasis is extremely rare. Described cases of metastatic ODG report various target sites including: bone, bone marrow, lymph nodes, liver, lung, and scalp.5,10–27 In a series of 116 patients with primary brain tumors which metastasized extracranially, only seven (5.25%) of the metastatic lesions were caused by oligodendrogliomas. 28
We describe a unique case of anaplastic oligodendroglioma with metastasis to the bone causing severe symptomatic skeletal hyperostosis along with a literature review and discussion of possible mechanisms of the metastasis.
Case Report
A 59-year-old female was referred to our service in 2011 for evaluation of osteosclerosis of unclear origin and a 6 year history of diffuse, progressive polyarthralgia and myalgia. She was diagnosed 16 years previously with a WHO grade III anaplastic oligodendroglioma which was treated with subtotal resection followed by radiation therapy. She was followed radiographically for a number of years without any evidence of tumor recurrence, and was eventually dismissed from follow-up and instructed to return if she developed neurological symptoms.
She developed diffuse pain 10 years after her initial resection which was treated as fibromyalgia, and questionable polymyalgia rheumatic. At the time of evaluation, she had been on 3.5 years of oral corticosteroids which had offered her moderate pain relief. A bone survey was ordered 16 years after her initial resection which showed diffuse mixed areas of sclerosis and lucency involving the axial and appendicular skeleton (Figure 1). Her bone density test showed markedly increased bone mineral density in her bilateral hips and lumbar spine (T-scores +5.4 to +9.7), except for her left femoral neck which was in the normal range for premenopausal women. Additionally, a nuclear medicine bone scan showed diffuse radiotracer uptake in the axial and appendicular skeleton. A CT scan of her abdomen and pelvis showed no evidence of a primary malignancy. The diagnosis was thought to be sclerosing bone dysplasias, myeloproliferative disorders including myelofibrosis, or granulomatous processes including sarcoid. Metastatic disease could not be entirely excluded, but was considered less likely.
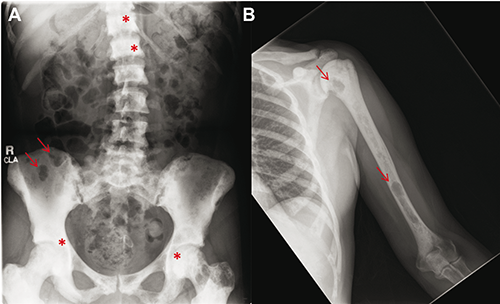
Bone survey for metastatic lesions. A) Diffuse mixed areas of lucency (arrows) and sclerosis (*) in the axial skeleton. B) Scattered areas of erosive scalloping most evident along the left humeral neck and distal region (arrows).
Neurological examination was normal. Laboratory analysis including complete blood cell count (CBC),erythrocyte sedimentation rate (ESR), chemistry profile, creatine kinase (CK), aldolase, 25-hydroxyvitamin D, 1,25-dihydroxyvitamin D, serum protein electrophoresis, fungal serologies, sensitive TSH, parathyroid hormone, C-reactive protein (CRP), serum angiotensin converting enzyme (ACE) and urinalysis were unremarkable.
Ten months after the initial evaluation, the patient developed new bilateral L5 radiculopathies and unintentional weight loss. An MRI of the lumbar spine revealed retroperitoneal, epidural and paraspinal enhancing soft tissue masses concerning for metastatic disease (Figure 2). The patient was unable to tolerate MRI imaging of the head and therefore a CT was obtained that showed low attenuation in the deep and subcortical white matter of the right pareital region underlying her previous parietal craniotomy as well as the left frontal convexity hypodensity without contrast enhancement. Given lack of recent intracranial imaging for comparison this was considered indeterminate for post-operative changes versus local recurrence.
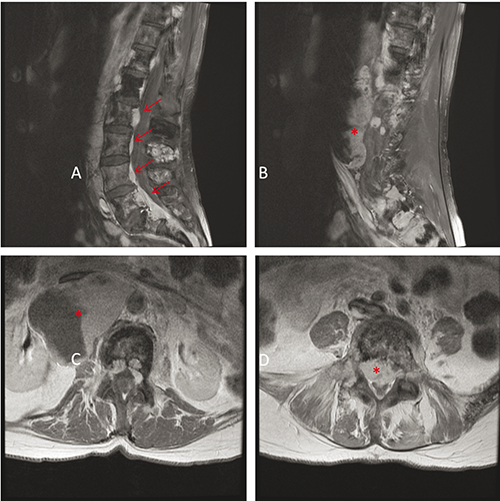
Lumbar spine magnetic resonance imaging (MRI). A,B) Sagittal T1-weighted MR image with contrast showing paraspinal enhancing soft tissue masses (arrows) and a large heterogeneous retroperitoneal mass extending from L1 through S1 (*). C) Axial T1 T1-weighted MR image with contrast showing partially cystic and partially enhancing retroperitoneal mass measuring 6.0×6.8×11.9 cm3 (*). D) Severe narrowing of the spinal canal below the level of L5 (*).
CT-guided biopsies of both the sizable retroperitoneal mass and right pelvic ilium were obtained. Each location demonstrated a 1p/19q co-deleted anaplastic oligodendroglioma (Figure 3).
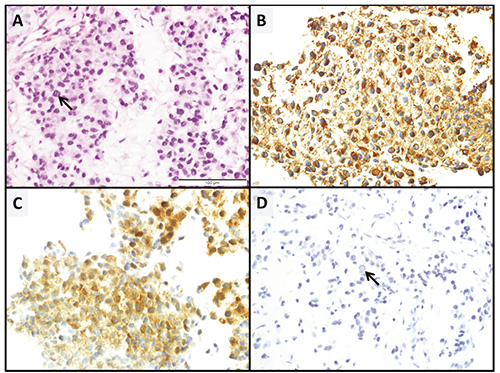
A) Right iliac bone fine needle aspiration/biopsy, 400× original magnification. Hematoxylin and Eosin (H&E) demonstrates the tumor cells to have relatively round nuclei and the tumor has a loose somewhat myxoid background. Mitotic figures are readily identified on the H&E as well as on the immunohistochemical stained slides (arrows). B) GFAP C) Mutant IDH (IDH1-R132H), and D) Oscar Keratin immunohistochemical stains. The tumor cells are noted to be strongly positive for GFAP and Mutant IDH while being negative for Oscar Keratin. This staining profile in conjunction with the morphology and the clinical history of an oligodendroglioma, support the diagnosis of a metastatic oligodendroglioma.
As oligodendroglioma is a chemotherapy-sensitive neoplasm, particularly in the setting of 1p/19q co-deletion, treatment with oral temozolomide was recommended. 29 In June 2013, she completed 14 cycles of temozolomide with a good response resulting in radiologically stable disease and improvement of her diffuse pain. However, in December 2013, she was seen at an outside hospital in consultation with our service with increasing bone pain and signs of cranial nerve III palsy. A MRI was performed with a new finding of a T2 hyperintense, solid/cystic mass involving the clivus and skull base, extending to the optic chiasm. (Figure 4). Due to a progression of the disease, the patient started Lomoustine (CCNU) and Avastin with good clinical response and stable radiologic disease.

Brain magnetic resonance imaging (MRI) taken on 2015. A) Axial Tl-weigthed MR image showing an expansile complex cystic/solid mass involving clivus ans skull base. B) Axial T2-weigthed MR image. C) Sagittal T1 MRI showing involvement of sphenoid sinus and considerable cystic feature of the lesion. D) T1 MRI coronal section.
Discussion
It is extremely rare for primary brain tumors to metastasize outside of the CNS.17,27,28,30 Lungs and lymph nodes are the most involved sites with distant metastasis from primary CNS tumors suggesting hematogenous and lymphogeneous pathways of dissemination.
Without surgical disruption, brain tumors are unlikely to metastasize via a hematogenous route. The thick walled larger veins of the brain present a difficult barrier to tumor invasion and the fast growth rate of CNS tumors within a space limited organ may compress and thrombose smaller veins further preventing metastatic escape. However, in event of a surgery, these conditions may be violated, increasing risk of metastasis.17,31
Lymphatic spread may present a more viable avenue for metastasis in the undisturbed brain tumor. In 1983 McComb demonstrated lymphatic drainage of cerebrospinal fluid into extracranial tissue which may explain the high incidence of metastasis from CNS tumors in cervical or retroauricular lymph nodes. More recently, functional lymphatic vessels have been described lining the dural venous sinuses. 32
It has been previously suggested that due to the paucity of connective tissue stroma in the brain, sub-populations of cells capable of invasion and spread through connective tissue are not selected for as they are in non-CNS tumors.17,31
A systematic review of the literature found a total of 21 papers reporting 34 cases of bony metastasis from oligodendrogliomas between 1951 and 20 1 4.5,10–27,33,34 From the total of 34 cases, 21 (61.7%) were male and the mean age was 38 years (range: 7-71 years). The most common site of bony metastasis was the spinal vertebral body (90%), while the appendicular skeleton involvement was reported in only 6 studies. The mean time between the primary tumor and the first symptoms of the metastasis manifestation was 45 months and the overall survival was 54 months on average. The patient's survival after the metastasis diagnosis was 11.9 months. 28
Two primary patterns of ODG metastasis have been described.
18
Pattern 1 is characterized by regional recurrence with scalp and cervical lymph node involvement and is associated with multiple craniotomies. Pattern 2 shows distant metastases without regional recurrence, as in this case, and is associated with radiation and chemotherapy, raising the possibility that early aggressive therapy alters the biology of the disease in a way that favors metastasis. It is unknown whether the characterization of
A particular predilection for bone has been reported in oligodendrogliomas. Our patient presented with a disseminated mixed lesion throughout the axial and appendicular skeleton. The predilection for bone tissue was explained by Zustovich

A) Lumbar spine X-ray showing sclerotic lesion in L1 vertebral body. B) Bone densitometry scan showing higher scores in L1 vertebral body (t-score 9.0; z-score 10.2). C) Sagittal lumbar magnetic resonance imaging showing decreased T1 signal at L1 vertebral body corresponding to the area of sclerosis seen on radiographs.
Conclusions
Metastatic oligodendroglioma is a very rare disease with a variety of different manifestations. Our paper presented a new manifestation of oligodendroglial bony metastasis causing osteosclerosis. This suggests a new yet rare differential diagnosis in patients with rheumatologic manifestations and previous history of malignant gliomas.