
Abstract
Second primary malignancies (SPMs) are issues for patients with multiple myeloma (MM). There may have been some limitations in prior studies, such as difficulties in a longer follow-up and absence of established screening methods. Therefore, we studied autopsied cases to overcome these limitations. This study aimed to examine SPMs using autopsy reports. Ninety-one cases of MM autopsied at our institution from 1979 to 2013 were analyzed. Median age of autopsied patients was 64.1 years, and proportion of male/female was 59/32. Autopsy was performed in 35.3% of patients died of MM. There were five cases of SPMs with a median confirmation time of 38 (12-132) months from the diagnosis of MM. In three of the five patients, the diagnosis of SPMs was established at autopsy. One case was of myelodysplastic syndrome, and the others were of non-hematological malignancies. The annual risk of SPM estimated using the Kaplan-Meier method was approximately 1%. Three of five SPM cases were detected at autopsy. Analysis of autopsy may contribute to estimate the actual risk of SPMs in MM.
Introduction
In the recent decades, the treatment of multiple myeloma (MM) has markedly improved, however second primary malignancies (SPMs) have become problematic for long-term sur-vivors. 1 The development of SPM in MM may reflect a combination of several causes such as host-related, disease-related, treatment-related, and environmental or behavioral factors. For host factors, MM develops in older popula-tions. 2 A gene expression microarray analysis revealed that germline polymorphisms may play a role in the development of MM and might have some role in the development of SPMs.3,4 Among the disease-related factors, epigenetic changes and alterations in signaling pathways may occur with the progression of MM.5,6 Furthermore, MM may influence immune cells including macrophages, T cells, or NK cells and disturb tumor immunity.7,8 Treatment-related factors have been intensively studied. 1 The tumorigenicity of nitrosourea is a well-known phenomenon. 9 Since Bergsagel et al. observed an increased the incidence of acute leukemia with the use of alkylating agents, 10 their role in the development of SPM has been widely assessed. 1 Cuzick et al. reported a positive association between the duration of L-PAM therapy and the subsequent risk of developing leukemia. In addition, they showed the cumulative doses of L-PAM given up to 3 years before the diagnosis of leukemia was the most important risk factor. 11 Although the Finnish Leukemia Group showed no significant correlation between the development of SPM and the use of L-PAM, 12 LPAM is widely viewed as a risk factor. 13 The risk of SPM after the use of high-dose L-PAM, as a preconditioning regimen for autologous stem cell transplantation, is not considered to increase the risk of SPM compared with lower doses of L-PAM. 14 However, the results of the Intergroupe Fraccophone du Myeloma (IFM) study suggested that the risk may be higher after double transplantation. 15 Recently immunomodulating agents (IMids) including thalidomide (Thal) and lenalidomide (Len) were identified as agents that may increase the risk of SPMs;16–18 however, this is controversial. For example, a meta-analysis by Palumbo et al. showed that SPMs were linked to Len and L-PAM combination therapy rather than Len monotherapy. 19
The exact mechanism by which SPMs develop remains elusive. 1 Although SPMs in patients with MM have been intensely studied since the 1960s, previous studies have some limitations. For example, they did not follow patients throughout life and the method used to screen for SPMs was not established in earlier studies. 20 Therefore, some SPMs may have been missed. Thus, we studied autopsied cases because an autopsy allows systemic pathological diagnosis and follow-up throughout the entire lifespan of a patient. The aim of this study was to examine SPMs using autopsy reports from patients with MM, although we are aware that focusing only on autopsies may yield some selection bias.
Materials and Methods
As shown in Table 1, this study included 91 consecutive cases of MM autopsied at National Center for Global Health and Medicine, Tokyo, Japan, from 1979 to 2013 (median patient age, 64.1 years; male/female ratio, 59/32). Autopsy was performed in 35.3% of patients died of MM. Most cases were Durie-Salmon stage III (M-proteins IgG/IgA/IgD/BJP/uncertain = 46/12/7/18/8). All patients had undergone conventional treatments. Twenty-one patients also underwent autologous stem cell transplantation (ASCT) during their treatment course. Thal and Len were used in six and three patients, respectively (the duration of Len use was 3-6 months; all three patients underwent ASCT before the administration of Len).
Characteristics of patients.

MM, multiple myeloma; IG, immunoglobulin; BJP, Bence Jones protein; ASCT, autologous stem cell transplantation; Thal, thalidomide; Len, lenalidomide.
Statistical Analysis
The cumulative incidence of SPMs was estimated using the Kaplan-Meier method. Statistical analyses were performed using SPSS (version 17.0).
Results
As shown in the Table 2, there were five cases of SPM (5.5% of all cases), with a median confirmation time of 38 (12-132) months since the diagnosis of MM. Prostate (n=2), lungs (n=1), and thyroid (n=1) were the sites of SPMs; there was also one case of myelodys-plastic syndrome (MDS). The diagnosis of SPM was established at autopsy in three of the five patients. SPMs tended to develop in older patients with median ages of 68.6 and 62.4 years in patients with or without SPMs, respectively (P=0.300; Table 3).
Characteristics of 5 second primary malignancies (SPMs) cases.

MDS, myelodysplastic syndrome. Median confirmation time form multiple myeloma diagnosis: 38 (12-132) months. Three SPMs cases are diagnosed at autopsy.
Comparison of age and overall survival (OS) between second primary malignancies (SPMs) positive and negative patients.

All five patients with SPMs were administered L-PAM, with a median cumulative dose of 784 mg. Three patients also received nitrosourea. Three and none of the five had used Thal and Len previously, respectively. One patient had previously undergone ASCT (Table 4). The estimated annual risk of SPM is shown in Figure 1.
Treatment history of 5 second primary malignancies (SPMs) cases.
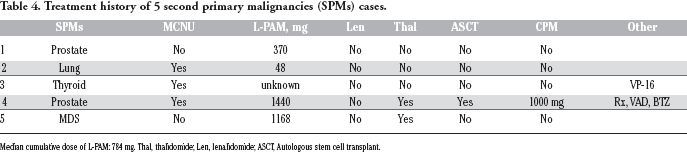
Median cumulative dose of L-PAM: 784 mg. Thal, thalidomide; Len, lenalidomide; ASCT, Autologous stem cell transplant.

Cumulative incidence of second primary malignancies estimated using the Kaplan–Meier method.
Discussion
SPMs are a potential risk in long-term MM survivors. 1 There have been challenges associated with studies of SPMs in MM, such as insufficient long-term follow-up and absence of an established screening method. 20 The aim of this study was to overcome these limitations using autopsies, which allows the systemic pathological diagnosis and the follow-up of patients’ whole life. We found three cases of SPM that were diagnosed at autopsy. This suggests that studying SPMs using autopsy is feasible. The 5.5% incidence of SPM and the median time of 38 months since the diagnosis of MM observed in the current study are consistent with previous reports.14,21,22 In addition, the annual risk of SPM estimated using the Kaplan-Meier method was similar to data based on 33,229 patients with MM between 1973 and 2008 in the United States, reported by Thomas et al. 1
Among the five cases of SPM, two were prostate cancer. In contrast, Razavi et al. reported a significantly lower overall risk of prostate cancer in patients with MM. 23 The incidence of hematological malignancies in the current study was similar to a recently published report from the Mayo clinic, which reported the long-term follow-up data of newly diagnosed patients with MM treated with Len and dexamethasone. 24 They found that 12 (4.2%) patients had an SPM and only two patients developed hematological malignancies.
Three of the five patients with SPMs were treated with nitrosourea in the current study. All five patients received L-PAM with a median cumulative dose of 784 mg, which is compatible with prior reports. 25 Because of the small number of patients with SPM in the current study, it is difficult to discuss a causal link between the use of IMids or ASCT and the development of SPMs. However, no SPM developed in the three patients who received Len, three of six patients who received Thal developed SPMs, and only one of the 21 patients treated with ASCT later developed an SPM.
The current study has some limitations that must be discussed. First, we could not avoid selection bias because we studied only autopsied cases. Second, the sample size was small. Nevertheless, our data provide several unique insights; especially 3 SPMs were found at autopsy and this may suggest the availability of studying SPMs based on autopsied cases. Because few similar approaches have been previously undertaken, therefore, we recommend that the current results should be explored in a larger cohort of patients.