
Abstract
Giant cell tumor (GCT) of tendon sheath is a localized form of tenosynovial GCT, which preferentially affects the joints of hands and feet. Chondroid metaplasia is a rare phenomenon in tenosynovial GCT either in localized or diffuse types. The current case investigates the cytological and histopathological features of chondroid GCT of tendon sheath in a 22-year-old female presenting with wrist swelling.
Introduction
Tenosynovial giant cell tumors (GCT) are the second most common tumors of the hand after simple ganglion cysts. 1 They are divided into localized and diffuse forms with a reported liability for recurrence. 2 Both forms show similar histopathological pictures, which are characterized by: proliferation of synovial-like mononuclear cells, variable numbers of multinucleate osteoclast-like cells form cells, siderophages and inflammatory cells. 3 The current case demonstrated chondroid metaplasia, which is a rare finding in giant cell tumors of the tendon sheath. The reported cases of tenosynovial GCT associated with chondroid metaplasia in English literature are listed in Table 1.4–8
The reported cases of tenosynovial giant cell tumor of tendon sheath with chondroid metaplasia.

NA, not available,
Range of age or size, the size is the maximal diameter of the lesion.
Case Report
A 22-year-old female presented to our hospital with a firm and painless swelling in her right wrist, 6 months before. No imaging studies were performed. The swelling was attached to the underlying tissue. Fine needle aspiration (FNA) cytology was performed and the aspirate was smeared and stained with Hematoxylin and Eosin. The aspirate was cellular and revealed many mononuclear stromal cells (histiocytes), few spindled shaped stromal cells and multinucleated osteoclast giant cells (Figure 1).

Fine needle aspiration cytology of the hand mass revealed mononuclear stromal cells with slight spindling (A) admixed with osteoclast giant cells (B). The stromal cells showed occasional grooving (arrow) (A) and intracytoplasmic vacuoles (arrow) (C) (Hematoxylin and Eosin staining 400×).
The stromal cells were mainly polygonal with abundant cytoplasm with occasional nuclear grooving (Figure 1A) and intracytoplasmic inclusions (Figure 1C). The lesion at this time was diagnosed as benign fibrohistiocytic lesion. Excision of the mass was done and the received mass was lobulated, whitish and measured 3×2×1 cm. Histological examination of excised mass revealed nodular growth formed of mononuclear and multinucleated histiocytes (Figure 2A) together with sheets of xanthoma cells and hemosidrin laden macrophages (Figure 2B). Metaplastic benign looking cartilaginous areas were also seen (Figure 2C). There was no evidence of atypia, necrosis or mitoses.
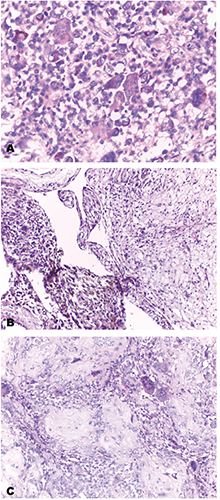
A) Mixture of proliferated mononuclear stromal cell, some of them were haemosirin laden and osteoclast multinucleated giant cells (Hematoxylin and Eosin staining 400×). B) Sheets of xanthoma cells and haemosidrin laden macrophages were also seen (Hematoxylin and Eosin staining 200×). C) Islands of metaplastic benign cartilage were detected intervening the fibrohistiocytic lesion (Hematoxylin and Eosin staining 200×).
Discussion and Conclusions
Giant cell tumor of tendon sheath is the localized form of tenosynovial GCT that preferentially affects the joints of hands and feet. Its most diffuse form is called pigmented villonodular synovitis. Since GCT is commonly presented as soft tissue mass, some cases may be submitted to FNA, which is a common practice. The cytological findings of the present case agree with previous reports on the presence of a lot of stromal mononuclear cells and few spindled admixed with osteoclast giant cells and xanthoma cells.9,10 The presence of the latter cells are responsible for its alternative name as xanthoma of tendon sheath or xanthogranuloma. 9 In the present case, we have also provided more cytological details such as the presence of nuclear grooving and cytoplasmic vacuoles similar to that reported by others.9,10 According to the present case and the previous reported ones, GCT diagnosis can be made based on fine needle aspiration data combined with classic clinical pictures.9–13
Histopathologic examination of excised specimen correlates with the FNA cytologic findings, however what was surprising is the presence of metaplastic chondroid foci. Chondroid metaplasia is a rare phenomenon in tenosynovial giant cell tumors either localized or diffuse types. 5 Cartilaginous and osseous metaplasia is a rare focal finding in giant cell tumor of tendon sheath. 14 Chondroid metaplasia is previously reported in pigmented villonodular synovitis.4-8 raising the differential diagnostic possibilities including chondroblastoma, synovial chondromatosis and chondrosracoma. According to Hoch et al., 6 chondroid matrix may range from chondromyxoid matrix with basophilic or eosinophilic matrix to chondro-osseous with dense eosinophilic matrix. Cells within chondroid component were reported to be identical to the larger mononuclear cells in the conventional tenosynovial giant cell tumor component. Although the present case demonstrates the classic cytological and histopathological features of localized form of tenosynovial giant cell tumor, it showed for the first time the presence of chondroid metaplasia in this neoplastic lesion.