
Abstract
Undifferentiated mammary sarcoma is extremely rare and the diagnosis is made only after exclusion of metaplastic carcinomas and malignant phyllodes tumor. Mammary sarcomas mostly display specified entities like liposarcomas or angiosarcomas. A 18-year-old female presented in 2010 with a right breast lump for which lumpectomy was done and on histopathological examination benign phyllodes tumor was diagnosed. In 2011, there was a recurrence at site of excised margin and on fine needle aspiration (FNA) the diagnosis of benign breast disease was made; a small biopsy was received for which diagnosis of myoepithelial lesion was given. Then, the whole mass was excised, but histopathological examination report could not be followed up. In 2013, she again presented with a mass arising from the previously excised margin; on FNA, it was diagnosed as malignant sarcomatous lesion. Microscopy showed spindle shaped cells in diffuse and fascicular pattern with plump ovoid nuclei; coarse chromatin and eosinophilic cytoplasm were seen. Few round to ovoid cells with eccentric nuclei and showing bi- or multi-nucleation were present. Large area of necrosis and hemorrhage was present, too. No breast glands were found. Later on, diagnosis was confirmed on immunohistochemical examination. The case was considered worth due to the young age of the patient and lack of differentiation of the lesion in any specific type of sarcoma and CD10 positivity.
Introduction
Undifferentiated mammary sarcoma (UMS) is a rare malignant tumor arising from the mesenchymal tissue of the mammary gland. 1 The mean age of presentation is 52 years (range 22-82). 2 The diagnosis of UMS is made only after exclusion of metaplastic carcinomas and malignant phyllodes tumor (MPT). Mammary sarcomas mostly shows features of liposarcomas or angiosarcomas and rarely pleomorphic sarcoma or malignant fibrous histiocytoma. 3 Hence, we present an unusual case of UMS which presented at early age with frequent recurrences.
Case Report
A 18-year-old female presented with a right breast lump for which lumpectomy was done in 2010. Two nodular masses with attached skin measuring 10×9×3.5 cm and 10×8×6 cm in size were removed (Figure 1A). Cut surface was lobulated with extensive areas of necrosis and hemorrhage. Histopathological examination (HPE) showed double layered epithelial component arranged in clefts with hypercellular stroma organized in leaf-like structures. The stroma consisted of hyperchromatic pleomorphic cells with prominent nucleoli. Mitosis was less than 4/hpf (high power field), hence a diagnosis of benign phyllodes tumor (PT) was made (Figure 1B). One year later, recurrence occurred at the site of excised margin of the tumor. Fine needle aspiration (FNA) showed scant cellularity with plump spindle cells arranged in clusters and also scattered singly. Mitosis was rare. No epithelial cell clusters were seen. A diagnosis of benign breast tumor was made (Figure 1C). A biopsy was received which showed 0.5×0.5 cm spindle cells in diffuse sheets. Few vacuolated cells were also found. No acini or epithelial lining was seen (Figure 1D). A diagnosis of mesenchymal/myoepithelial lesion was given and excision was advised. Patient was lost to follow up and no histopathological examination could be done.

Panel of representative photomicrographs showing (A) gross nodular, solid tissue piece. Inset: inflamed recurrent mass. B) Benign phylloides showing cleft like spaces. Inset showing benign glandular elements. C) Cytology showing scant cellularity. Inset shows plump spindle cells. D) Spindle to ovoid cells with hyper chromatic nuclei, inconspicuous nucleoli and ill defined pale cytoplasm. E) Cytology from recurrent nodule showing increased cellularity and pleomorphism. Inset showing high mitosis. F) Spindle shaped cells arranged in diffuse and fascicular pattern. Inset showing bi- and multi-nucleation and mitosis.
Two years later, the patient again presented with the second recurrence at the excised margin. Clinically, the mass was nodular, firm and inflamed measuring 3×3 cm (Figure 1A). This time the cytological and histological features suggested an aggressive tumor. On FNA, cellularity was increased with pleomorphic spindle cells arranged in clusters and scattered singly. Mitosis was more than 10/hpf. Again no epithelial elements were seen. A cytological impression of malignant sarcomatous lesion (Figure 1E) on FNA was given. Later, the mass got ulcerated, was excised and sent for HPE. Gross examination showed necrotic and hemorrhagic areas. On microscopic examination large areas of necrosis and hemorrhage were present in center. Spindle shaped cells arranged in diffuse and fascicular pattern with plump ovoid nuclei, coarse chromatin and eosinophilic cytoplasm were seen. At the periphery, few round to ovoid cells with eccentric nuclei and showing bi- or multinucleation were present. Mitosis was more than 8/10 hpf (Figure 1F). No epithelial elements were found.
On the basis of cytohistomorphological features, differential diagnosis considered were: MPT, UMS, nodular fasciitis (NF), metaplastic carcinoma (MC), myoepithelial carcinoma (MEC) and leiomyosarcoma (LMS). A large panel of antibody were used for immunohistochemistry (IHC) for further differentiation. The clone, antibody dilution and source of antibody are shown in Table 1. As seen in Table 2, only CD10 (15-30%), vimentin (70-80%), EGFR (60-70%) (Figure 2A-C) and Ki67(15-30%) were positive in present case. CD34 showed positivity around blood vessels whereas it was negative in tumor cells. On the basis of clinical presentation, cytology, histology and IHC (Table 2) a final diagnosis of CD10 positive UMS was made.
Specification of immunohistochemical markers used in present case.
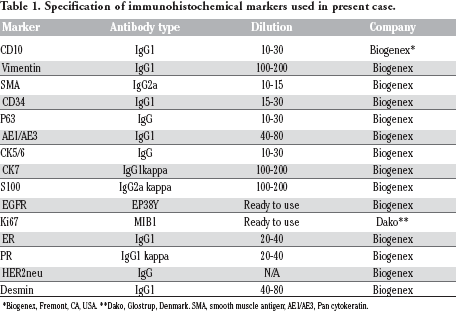
Biogenex, Fremont, CA, USA.
Dako, Glostrup, Denmark. SMA, smooth muscle antigen; AE1/AE3, Pan cytokeratin.
Comparison of immunohistochemical findings of present case with various differential diagnosis considered.

MPT, malignant phylloides tumor; NF, nodular fascitis; MC, metaplastic carcinoma; MEC, myoepithelialcarcinoma; LMS, leiomyosarcoma, UMS, undifferentiated mammary sarcoma; NR, no role; HPE, histopathological examination; IHC, immunohistochemistry.

Immunohistochemical findings. Tumor cells show (A) strong CD 10 positivity (B) Vimentin diffusely positive (C) EGFR strongly and diffusely positive (D) CD 34 positivity around the blood vessels and negative in tumor cells.
Discussion
Undifferentiated mammary sarcoma, are rare histologically and heterogeneous non-epithelial malignancies that arise from the mammary stroma. 1 They account for less than 1% of all breast malignancies and less than 5% of all soft tissue sarcomas. 4 They can develop de novo (primary) or secondary after radiation therapy (RT) or lymphedema of the arm or breast after treatment of another malignancy.5–7 Our case was a case of primary UMS.
The mean age for mammary sarcoma is reported to be 52 years (range 22 to 82). Out of all the lesions considered in differential diagnosis only nodular fascitis can present at an early age group (2nd-3rd decade) as shown in Table 3. Our case was relatively younger (18 years). 8 On the basis of histopathological and cytopathological examination various main differential diagnosis considered were: MPT, UMS, NF, MC, MEC and LMS. The common presenting and cytohistomorphological features of various lesions have been summarized in Table 3. Comparative IHC panel as shown in Table 2 helped in coming to a final diagnosis. MPT was considered as a first diagnosis but young age of the patient and CD34 negativity in tumor cells (Figure 2D) ruled out this diagnosis. 2 NF has a rare recurrence in breast and because of early age of presentation in 2nd-3rd decade of life, it was kept as a differential diagnosis. SMA and Desmin were negative in present case, hence NF was ruled out. 9 Negative IHC for CK5/6, CK7, p63, ER, PR and weak positivity for EGFR ruled out MC (Table 2). 10 MEC is predominantly composed of myoepithelial cells and showed positivity for S-100, p63, CK5/6 and SMA, which were negative in this case.11,12
Histopathological findings of various differential diagnosis considered on microscopy.

D/D, differential diagnosis; MPT, malignant phylloides tumor; NF, nodular fascitis; MC, metaplastic carcinoma; MEC, myoepithelialcarcinoma; LMS, leiomyosarcoma, UMS, undifferentiated mammary sarcoma; NR, no role; HPE, histopathological examination.
LMS are hypercellular with nuclear atypia high mitotic counts and with areas of necrosis. They are immunoreactive for SMA, Desmin, Calponin, H-caldesmon, and Vimentin.13,14
In our patient SMA and Desmin (Table2) were negative and hence this diagnosis was ruled out. The patient also showed positivity for CD10 (10-15%). CD10 is a new stromal marker which is important in prognostication and possible therapeutic intervention in invasive breast carcinoma.15,16
Expression of CD10 in stromal cells is associated with poor prognosis, estrogen receptor negativity and high grade. 17
Conclusions
On the basis of cytohistomorphological features and IHC a final diagnosis of CD10 positive UMS was made. Patient is clinically well with no systemic symptom and had been referred to higher center for further follow up and treatment. Later, she did not report back for further follow up.