
Abstract
Aneurysmal bone cyst (ABC) is a rare benign cystic lesion of the bone that composes 1-2% of the entire bone tumors. Some are idiopathic, and some occur secondary to other tumors such as giant cell tumor and chondroblastoma. In this article, we report the clinical, radiographic, and histological findings of a secondary ABC following chondroblastoma of the patella with a review of the literature.
Introduction
Patella is a rare site for a tumor or tumorlike lesion to develop. Casadei et al. analyzed the literature from 1900 to 2009 and found a total of 536 cases. Among the reported tumor cases, giant cell tumor (31%) and chondroblastoma (16%) were the most common benign tumors. 1 Chondroblastoma has been reported to occur simultaneously with aneurysmal bone cyst (ABC) in 10-15% of the patients. 2 ABC is a benign cystic lesion of the bone that is separated by fibrous septa which are filled with vascular channels and blood. It is a rare tumor that composes 1-2% of the entire bone tumors. 3 ABC may present as a primary or secondary lesion following hemorrhagic change due to giant cell tumor, chondroblastoma, hemangio - endothelioma, fibrous dysplasia and teleangiectatic osteosarcoma. 4 Common sites include distal femur, proximal tibia, proximal fibula, pelvis and proximal humerus. In this report, we present a rare case of secondary ABC of the patella after chondroblastoma.
Case Report
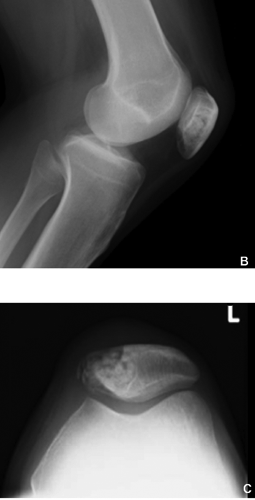
A 25 year-old male was referred to our hospital complaining of left knee pain. He had the symptom for 2 years without a prior history of trauma. The pain deteriorated after participating in a Judo competition. He visited a nearby hospital and a radiolucent area of the patella was pointed out on the plain radiograph of a knee. He was suspected of a bone tumor and referred to our hospital. He did not have any relevant family history of tumor or medical history. Physical examination showed a slight atrophy of the left thigh (42 cm compared to his right, which was 45 cm), but did not show tenderness or restriction in range of motion. The overlying skin was smooth without any hotness or redness. Plain radiograph showed a soap bubble-like radiolucent area in the medial patella measuring 1.7×2.4 cm. Periosteal reaction was absent (Figure 1A-C).

Radiograph of the left knee depicting (A) anteroposterior, (B) lateral and (C) skyline view. There is a 1.7×2.4 cm radiolucent area in the medial patella. On MRI, patella lesion is hypointense on T1WI (D) and hyperintense on T2WI (E). Gadolinium-contrast shows a diffusely enhanced lesion in the medial patella (F).
On the MRI, the lesion was depicted as low intensity on T1WI and high on T2WI, which was diffusely enhanced after gadolinium-contrast administration. The tumor was composed of multiple cavities, and fluid level was observed in each compartments. There was no obvious invasion to the adjacent muscle or joint (Figure 1D-F).
The tumor was composed mostly from blood filled cavities and intraoperative histological finding revealed a lesion with fibrotic changes and proliferation of histiocyte-like cells and fibroblasts, accompanied by multinucleated giant cells, hemosiderin deposits and bony fragments. No evidence of malignancy was present. Intralesional curettage was performed with the addition of heat ablation and was later filled with artificial bone graft.
On histopathology, the tumor was a giant cell lesion with fragmented bones with fibrosis, hemosiderin deposits and mild infiltration of chronic inflammatory cells compatible with ABC. In limited areas, there were monocytes that were short spindle-shaped and slightly positive with S-100 staining, which was consistent with chondroblastoma (Figure 2A,B).
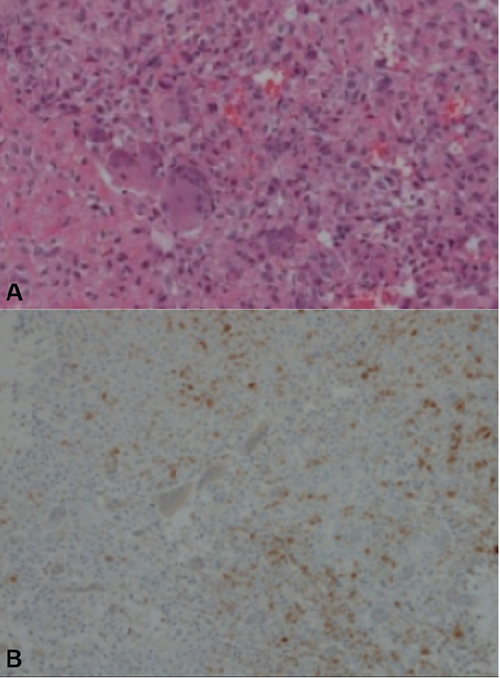
A) Under the microscope, the tumor was a giant cell lesion with fragmented bones and fibrosis, hemosiderin deposits and mild infiltration of chronic inflammatory cells (H&E stain); B) Monocytes of the lesion was short spindle-shaped and slightly positive with S-100 staining.
Postoperative period was uneventful. During his 9 months follow-up, no recurrence or arthritic change of the knee has developed (Figure 3A-C).
Radiograph at 9 months follow-up. A) Anteroposterior, B) lateral and C) skyline views of the knee. The artificial bone graft is seen in the cavity and no evidence of recurrence or arthritic change is present.
Discussion
ABC is a rare bone tumor comprising approximately 1-2% of all bone tumors and is characterized as a benign cystic lesion of the bone that is separated by fibrous septa which are filled with vascular channels and blood. It mostly occurs in the distal femur, proximal tibia, proximal fibula, pelvis and proximal humerus. Its precise pathogenesis is still unclear, although it has been associated with trauma, subperiosteal hematoma, other benign tumor, and circulation abnormalities such as venous occlusion or arteriovenous malformation. 5 Recently, translocation of TRE17/USP6 has been shown to be present in the majority of ABC, 6 however the exact role of TRE17 and USP domain needs to be further elucidated. ABC occurring on the basis of any previous lesion is referred to as secondary ABC with a reported incidence of 29-35%. 7 Giant cell tumor (GCT), chondroblastoma, chondromyxoid fibroma, telangiectatic osteosarcoma, fibrous dysplasia, and eosinophilic granuloma have been reported to precede secondary ABC.
Chondroblastoma sometimes coexist with ABC in 10-15% of the patients. 2 Chondroblastoma comprises 1-3% of primary bone tumors, occurring in patients between 10 and 20 years of age, and is more prevalent in males. It tends to occur in the epiphyses of the long bone, and the occurrence in the patella is uncommon, with a reported incidence of approximately 6%. 8 When the tumor is present in the patella, the most common complaint is the pain in the knee. Due to its proximity to the knee joint, joint swelling and limitation of motion has been also reported. Singh et al. reported a multicenter experience of 59 cases of patella tumors and tumor-like lesions, and 6 of them were aneurysmal bone cysts, including those secondary to giant cell tumor and chondroblastoma. 9 To date, there have been six reported cases of secondary ABC occurring concurrently with chondroblastoma in the literature.8,10–14 On the plain radiograph, chondroblastoma shows a feature similar to that occurring in other sites; eccentric, geographic bone destruction with lobulated margins, and thinned cortex. Calcification may sometimes be seen and periosteal reaction is uncommon. CT may be useful in identifying small diffuse calcification and MRI is useful for demonstrating typical cartilaginous pattern and the perilesional bone and soft tissue edema pattern distinctive for this tumor. 15 On MRI, fluid levels reflecting the pooling of blood within the septal cavity is a typical feature of this tumor. 1 It is sometimes difficult to distinguish between other lesions. GCT has a less distinctive margin, but it is sometimes difficult to distinguish by plain radiograph only. Fibrous dysplasia also has an eccentric lesion on plain radiograph, but the ground-glass appearance due to the increase in amounts of mineralized woven bone is typical feature in this tumor. Chondromyxoid fibroma generally has a more sclerotic margin on the plain radiograph. Telangiectatic osteosarcoma is another differential diagnosis, but this lesion in the patella rarely shows a fluid level on MRI. Peripheral chondrosarcoma is difficult to distinguish from chondroblastoma on imaging, but there are no literature reporting its formation in the patella. The most important differentiation should be made between telangiectatic osteosaromca, where delay in diagnosis could lead to death. In cases where radiological diagnosis is difficult, it is imperative to undergo biopsy to look for osteoids in case of osteosarcomas.
In our case, although the radiological findings lead to the diagnosis of ABC, we underwent intraoperative biopsy to confirm the diagnosis before attempting curettage.
Multinucleated osteoclast-like giant cells appear in various lesions such as giant cell tumor and aneurysmal bone cyst, but the presence of chondroblastic foci distinguishes chondroblastoma from other benign tumors. Chondrocytes in the chondroblastic foci contain S-100 protein which can be proven by an immunohistochemical examination. 16 Therefore every attempt is necessary for thorough examination of the resected samples to search for chondroblastic foci. When aneurysmal bone cyst coexists with chondroblastoma as in our case, multiple small vascular lesions surrounded by multinucleated giant cells are usually present. The possibility that the TRE17/USP6 oncogene, which was first identified in 1992, may play a key role in the etiology of ABC has been pointed out in a recent report. 17 This may be a next arsenal in distinguishing primary ABC from secondary lesions.
The treatment for chondroblastoma is performed by local resection or curettage of the lesion. Adjuvant treatments such as heat, phenol, and cryotherapy are often utilized to limit the risk of local recurrence. Better outcomes have been reported with the addition of bone grafting of the cavity. 2 Patellectomy is sometimes performed in cases where the tumor has invaded a substantial portion of the patella or destruction of the articular surface. The standard treatment is the same for ABCs. Although chondroblastoma is a benign tumor, local recurrence rate is 8-20% and the reason could be due to incomplete curettage. 2 Other reports young age, male gender, central location, stage and cellular component on histology as factors for local recurrence. 18 There have been several reports where, histologically benign looking chondroblastoma behave aggressively, occasionally metastasizing to the lungs. 19
Chondroblastoma is resistant to both chemotherapy and radiotherapy, therefore they are not applied in the treatment. There have been sporadic reports of sarcomatous formation after the radiotherapy. 20 Nine months after surgery, no evidence of recurrence has been observed and full range of motion of the knee has been acquired in our case.
Conclusions
We experienced a rare case of secondary ABC in the patella. The histologic findings revealed that the lesion was a secondary change to chondroblastoma. Curettage and ablation was carried out, and at 9 months post-surgery, there is no evidence of recurrence and the patient is free of symptoms. Because there are reports of local recurrence and malignant variants, further follow-up should be warranted.