
Abstract
The local control of desmoid tumors constitutes a continuing treatment dilemma due to its high recurrence rates. The purpose of this systematic review was to critically examine the current treatment of these rare tumors and to specifically evaluate the local failure and response rates of surgery, radiation and systemic therapy. We comprehensively searched the literature for relevant studies across Cinahl, Embase, Medline and the Cochrane databases. Articles were categorized as surgery, radiation, surgery + radiation and systemic therapy (including cytotoxic and non cytotoxic). Methodological quality of included studies was assessed using the Newcastle-Ottawa Scale. Pooled odd ratios (OR) for comparative studies and weighted proportions with 95% confidence intervals (CI) are reported. Thirty-five articles were included in the final analysis. Weighted mean local failure rates were 22% [95% CI (16–28%)], 35% [95% CI (26–44%)] and 28% [95% CI (18–39%)] for radiation alone, surgery alone and surgery + radiation respectively. In the analysis of comparative studies, surgery and radiation in combination had lower local failure rates than radiation alone [OR 0.7 (0.4, 1.2)] and surgery alone [OR 0.7 (0.4, 1.0)]. Weighted mean stable disease rates were 91% [95% CI (85–96%)] and 52% [95% CI (38–65%)] for non cytotoxic and cytotoxic chemotherapy respectively.
The current evidence suggests that surgery alone has a consistently high rate of local recurrence in managing extra-abdominal desmoid tumors. Radiation therapy in combination with surgery improves local control rates. However, the limited data on systemic therapy for this rare tumor suggests the benefit of using both cytotoxic and non cytotoxic chemotherapy to achieve stable disease.
Introduction
The local control of desmoid tumors constitutes a continuing treatment dilemma for surgical oncologists, medical oncologists and radiation oncologists alike. 1 Despite being benign, these tumors tend to be infiltrative and invade regional normal structures making their complete extrication difficult without untoward normal tissue effects. Even when these locally aggressive tumors are successfully removed without any disease at the margins of resection, local failure is common. Although MacFarlene was the first to describe what was later called desmoid tumors or aggressive fibromatosis in 1852, 2 the clinical management of this tumor remains a challenge. Depending on the two major anatomic locations in which they are present, desmoid tumors are classified as extra-abdominal or abdominal, the latter of which can further be subdivided into superficial and intra-abdominal.3,4 Extra-abdominal desmoid tumors arising from musculoaponeurotic structures in the extremities and the limb girdle are a particularly difficult therapeutic problem and are the focus of this study. 5 Extra-abdominal desmoid tumors are frequently aggressive, with a poorly circumscribed local infiltrative pattern and have a marked propensity for recurrence.6,7
Aggressive wide local excision has become the preferred treatment; however the recurrence rates are reported well above 40%.2,8–11 Moreover, difficulty in achieving acceptable cosmesis is a central barrier to such an approach. 6 Although surgical excision has been the principle therapy, radiation has also been employed for extra abdominal desmoid tumors resulting in improved local control and recurrence rates.12,13 Radiation therapy has been given as adjuvant treatment to decrease local recurrence especially when the surgical margin is positive. 14 However, many authors still judge radiation to be of limited value in the curative treatment of patients with desmoid tumors.15,8 More recently, recurrent extra abdominal desmoid tumors have been treated with systemic therapy, including both cytotoxic and non cytotoxic chemotherapy. Such modalities are thought to stabilize the disease and increase progression free duration with the aim to induce remission and to reduce morbidity. 4
Given the diversity of study conclusions noted in the literature, there is little consensus regarding the role of radiation therapy, surgery and chemotherapy in the clinical management of extra-abdominal desmoid tumors. The purpose of this study was to perform a systematic review and meta-analysis in order to crystalize the evidence available regarding local control of this rare and challenging clinical entity.
Materials and Methods
Search strategy
A literature search with the assistance of a professional librarian was conducted of the following electronic databases: Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, MEDLINE (January 1950 to January 2011), CINAHL (January 1982 to January 2011, and EMBASE (January 1980 to January 2011). The key words used were a combination of fibromatosis, extra-abdominal tumor, desmoid tumor, and therapy with limits, English and human.
Article eligibility
Two reviewers independently scanned the retrieved articles’ abstracts for potential relevance. The inclusion criteria were the following: i) a study following patients who had treatment of extra-abdominal desmoid tumors; ii) a comparative study evaluating different modalities for treatment of extra-abdominal desmoid tumors including randomized controlled trials and observational studies; iii) use a clinical outcome marker (i.e. recurrence rate) to evaluate differences in modalities for treatment of extra-abdominal desmoid tumors; iv) or be unpublished data from studies fulfilling criteria i) or ii). The exclusion criteria were the following: i) articles exclusively examining non-living populations or animal studies; ii) articles examining intra-abdominal desmoid tumors; iii) case reports; iv) articles that studied other variables outside of the treatment of extra-abdominal desmoid tumors. Any disagreement on the potential relevance of an article was resolved by an arbitrator.
Classification and outcomes measures
Studies were categorized based on the type of modality. The modalities that were evaluated were the following: surgery, radiation (pre-operative or post-operative), surgery + radiation, and systemic therapy (including cytotoxic and non cytotoxic). Surgical procedures were described as wide, primary or complete excision as well as intralesional or marginal excision. We operationally defined cytotoxic therapies to be those directly toxic to cells. The results of each study were examined with respect to local failure rate and for systemic therapy response duration and stable disease rates (defined as complete response + stable disease).
Assessment of methodological quality
The methodological quality of the included studies was independently assessed by two reviewers using the Newcastle-Ottawa Scale for Cohort Studies. 16 This scale assesses selection bias, ascertainment of exposure, comparability of the cohorts on the basis of design or analysis, as well as the follow-up period. Although the scale contained eight items, each study could receive a maximum total score of 9 since one item (comparability) was out of two as defined by the scale creators. 16 It was decided a priori that a score of 7 or more would be considered high methodological quality, a score of 5–6 would be considered moderate and a score of less than 4 would be considered low methodological quality. The reviewers resolved any discrepancies through discussion and re-evaluation of the methodology of the study in question.
Data extraction
The following data were extracted from each primary article and used for descriptive and statistical comparisons: author, year, sample size, study design, duration of follow-up, study results and recommendations.
Data analysis
All data are summarized descriptively. A kappa statistic, a measure of chance-corrected agreement, was calculated to provide an estimate of agreement between reviewers with regard to the articles that were retrieved for evaluation. We chose an a priori criterion of k≥0.65 to indicate adequate agreement. Quality assessment scores were reported as a mean and standard deviation. Inter-rater reliability was assessed by calculating intraclass correlation coefficient. Level of agreement between the two reviewers with 95% confidence intervals (CI) is reported. Heterogeneity among studies was tested using the Cochrane Q test with a P-value set at 0.1 for significance. 17 The I-squared statistic is reported representing the percentage of total variation across studies due to heterogeneity. The I-squared of less than 25% represents low heterogeneity, 25–50% moderate heterogeneity and more than 50% high heterogeneity. 17 We planned to use a random effect model in the presence of heterogeneity and fixed effect model otherwise. A funnel plot was done as an assessment tool for publication bias (Appendix). A meta-analysis of pooled odds ratios (OR) was performed for comparative studies and weighted pooled proportion was calculated for all single group studies. An alpha or 0.05 was considered a criterion for statistical significance. Pooled estimate of OR for comparative studies and weighted proportions with 95% CI for single group studies are reported. Review Manager 5.0 (Cochran Library for Systematic Reviews) and StatsDirect 2.7. (StatsDirect Ltd, UK) was used for data analysis.
Results
Literature search and quality of included studies
The literature search identified 3010 potential articles. After application of inclusion and exclusion criteria, 35 articles were deemed relevant and included into final analysis (Figure 1). There were no randomized controlled trials identified. The weighted kappa for overall agreement between reviewers for the final eligibility decision was 0.91 [95% CI (0.85–0.96)]. From this total of 35 papers, seven were categorized as radiation therapy (all retrospective design),6,15,16,18–22 18 as surgical therapy (2 prospective design; 16 retrospective design),2,3,5,8–11,13,18,22–30 and 14 were considered combination therapy (3 prospective; 11 retrospective design).3,6,8,10,12,13,18,19,22,26,28,30–32 Furthermore, nine were considered systemic therapy, four non-cytotoxic (3 prospective; 1 retrospective design),33–36 and 5 were cytotoxic (3 prospective; 2 retrospective design).7,37–40 The mean quality assessment score was 7.23±0.84, which was considered high. The level of agreement of the quality assessment between the two reviewers was 88.2% [95% CI: (76.6–94.0%)]. Funnel plots were done and demonstrated symmetrically distributed plots (in the shape of an inverted funnel) indicating the absence of publication bias (Appendix).
Search strategy.
Local failure rates
The local failure rates for all studies are summarized in Tables 1–3.2,3,5,6,8–10,13,15,18–32 The weighted pooled proportion for local failure rate for all studies evaluating radiation alone was 0.22 [95% CI: (0.16–0.28)] with between study heterogeneity of I2=15% (P=0.315) (Table 1),6,15,18–22 and for surgery alone was 0.35 [95% CI: (0.26-0.44)] with between study heterogeneity of I2=90%, (P<0.001) (Table 2).2,3,5,8,9,13,18,23–30 The weighted pooled proportion for local failure rate of all studies evaluating the combination of surgery + radiation was 0.28 [95% CI: (0.18-0.39)] with between study heterogeneity of I2=84% (P<0.001) (Table 3).3,6,8,10,13,18,19,22,26,28,30–32 When evaluating comparative studies, the pooled OR for local failure rate indicated that surgery + radiation in combination had lower local failure rates than radiation alone [0.69, 95% CI: (0.38, 1.23), P=0.20] and surgery alone [0.69, 95% CI: (0.47, 1.00), P=0.05] (Figures 2 and 3). There was 20% between-study heterogeneity for surgery + radiation versus radiation alone (I2=20%, P=0.29), and no between-study heterogeneity for surgery + radiation versus surgery alone (I2=0, P=0.96).
Radiation therapy.

RS, retrospective study; NS, not specified.
Surgical therapy.

RS, retrospective study; PS, prospective study; PE, primary excision; NS, not specified.
Combination therapy.
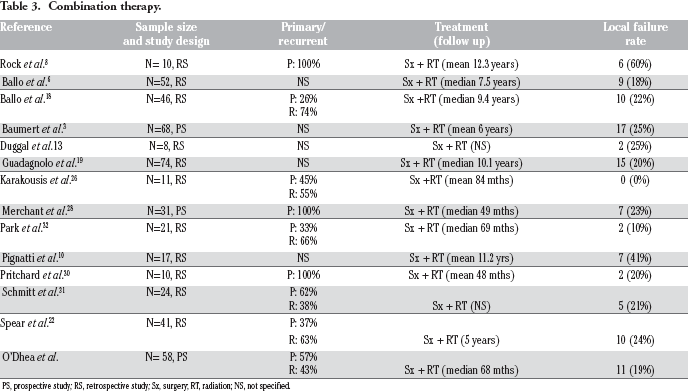
PS, prospective study; RS, retrospective study; Sx, surgery; RT, radiation; NS, not specified.
Forest plot for local failure rates for radiation vs. radiation + surgery.
Forest plot for local failure rates for surgery vs. surgery + radiation.
Response rate for systemic therapy
The response rates for systemic therapy are summarized in Tables 4 and 5.33–36 The weighted pooled proportion response rates were 0.91 [95% CI: (0.86–0.96)] for studies that evaluated non cytotoxic therapies (I2=0%, P=0.581) and 0.52 [95% CI: (0.39–0.65)] for studies that evaluated cytotoxic therapies (I2=29%, P=0.228).
Non-cytotoxic chemotherapy.

PS, prospective study; RS, Retrospective study; ITB, Imatinib; SD, stable disease; CR, complete response; 1NFa, interferon alpha; NS, not specified.
Cytotoxic chemotherapy.

PS, Prospective study; RS, retrospective study; MTX, methotrexate; VBL, Vinblastine; DRN, doxorubicin; DCB, Dacarbazine; SD, stable disease; CR, complete response; PLD, pegylated liposomal doxorubicin.
Discussion
The optimal management of extra-abdominal desmoid tumors remains an area of controversy. As such, the aim of this systematic review was to critically examine the existing literature on the local failure and response rates of surgery, radiation and systemic therapy for the treatment of desmoid tumors in order to identify the most effective treatment options. The summative results of this level III evidence suggests that surgery alone had a higher local failure rate compared to radiation alone or surgery combined with radiation. When strictly evaluating comparative studies, the combination of surgery and radiation outperformed either surgery alone (P=0.05) or radiation alone (P=0.20). This paralleled the results of a review done by Nuyttens et al. in 2000, that showed that local control after radiation or surgery combined with radiation was superior to that of surgery alone. 41
Although, wide excision advocated by Bouffier in 1899 has been deemed the treatment of choice in all age groups for local control, 42 this systematic review suggests the potential for successful outcomes using radiation alone and in combination with surgery. Specifically, adjuvant radiation is capable of destroying microscopic residual desmoid tumor left behind from positive margins following surgery.26,43 In following the sentiments of many authors that a desmoid tumor is a benign entity, this review advocates against the use of surgery as a monotherapy. In patients where cosmesis is hard to achieve, radiation is a modality associated with low complication rates due to the modest doses (50 to 60 Gy) required to control this tumor.26,42 Therefore, the evidence-based recommendation of this systematic review is to treat extra-abdominal desmoid tumours with either radiation alone or radiation + surgery to achieve local control but not with surgery alone.3,6,10,19
Due to the indolent and non-metastazing nature of extra-abdominal desmoid tumors, the use of chemotherapy has been limited. Both cytotoxic and non cytotoxic modalities have been described with varying degrees of success including agents such as doxorubicin, methotrexate, vincristine, dactinomycin, cyclophosphamide, binblastine, hormonal agents, kinase inhibitors and non-steroidal anti-inflammatory medications. 43 According to this review of level III evidence, both cytoxic and non cytotoxic treatments have very high stable disease rates (>50%). However, caution must be taken when evaluating such results of chemotherapies for local control of extra-abdominal desmoid tumors. Many patients often had many rounds of chemotherapy and extensive local management including surgery and radiation prior to the published result. Thus, it is hard to tease out the effectiveness of systemic therapy alone. In addition, many tumors that are untreated may in fact remain stable, thus the effect of systemic treatment in these cases would be overestimated. Overall, it appears there is a role for systemic therapy, more specifically non-cytotoxic chemotherapy, in treating extra-abdominal desmoid tumors having reported stable disease rates >80%.33–36
There are certain limitations to the current systematic review. First, the included studies are of lower quality (observational design) and the majority with retrospective design. Observational studies are subject to many biases i.e. selection bias and detection bias and retrospective studies are prone to data inaccuracy as well as missing information. Second, there is a variation in treatment modalities used for extra-abdominal desmoid tumors and in the follow up of patients (ranging from 2 years to 10 years). As a result, the outcomes of such modalities are very heterogeneous, which was evident in the surgery alone and surgery + radiation data. This limits the generalization of our results. In addition, genotypic status (including beta-catenin mutational status) and specific tumor characteristics were not adequately reported thus potentially causing confounding variables. In addition, the studies did not discriminate between adult and pediatric patients, although familial cases were excluded. However, we believe that the largest shortcoming of this review is its lack of large scale, well-controlled clinical trials. Due to the rarity of desmoid tumors, with an incidence rate of 0.2–0.5 per 100,000, large randomized controlled trials do not exist in the literature and therefore this meta-analysis attempts to consolidate the current evidence. 7
The strength of this systematic review, however, is that it is the most comprehensive summary data to date including studies evaluating both local and systemic therapies. This systematic review highlights the need for high quality, methodologically sound randomized controlled trials to help better differentiate treatment modalities for extra-abdominal desmoid tumors specifically radiation and systemic modalities.
Conclusions
In conclusion, the management of extra-abdominal desmoid tumors remains controversial. The data in this systematic review suggests that there is evidence to support combined radiation and surgery, but not surgery alone in the local management of these tumors. In addition, systemic treatment, particularly with non cytotoxic agents, appears to be a promising approach and should be evaluated in randomized prospective trials.
Footnotes
Acknowledgements:
The authors would thank Dr. Michael Fraumini for the database search strategy.